3899
Improved differential diagnosis between Prostate Cancer and Benign Prostate Hyperplasia using APT and IVIM1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijing, China
Synopsis
It is difficult to differentiate prostate tumors and prostate hyperplasia using conventional MR imaging methods. Amide proton transfer-weighted imaging is a novel MRI imaging tool for detection of amide protons in mobile cellular proteins and peptides. We aimed to evaluate the differential diagnosis of prostate cancers and benign prostatic hyperplasia using APT and IVIM. Results showed that prostate cancers were associated with higher APT values than benign prostate hyperplasia, while diffusion and perfusion parameters of IVIM were lower in prostate cancers. The diagnostic efficiency between prostate cancer and prostatic hyperplasia was higher with combinational use of APT and IVIM parameters.
Introduction
IVIM imaging has been previously explored in the differential diagnosis of benign and malignant prostate tumors, and the diagnosis confidence remains to be elevated1-2. Amide proton transfer-weighted (APTw) imaging is a novel MRI imaging tool to detect amide protons in mobile cellular proteins and peptides3. This study aimed to differentiate prostate cancers and benign prostate hyperplasia with combinational use of APT and IVIM.Materials and Methods
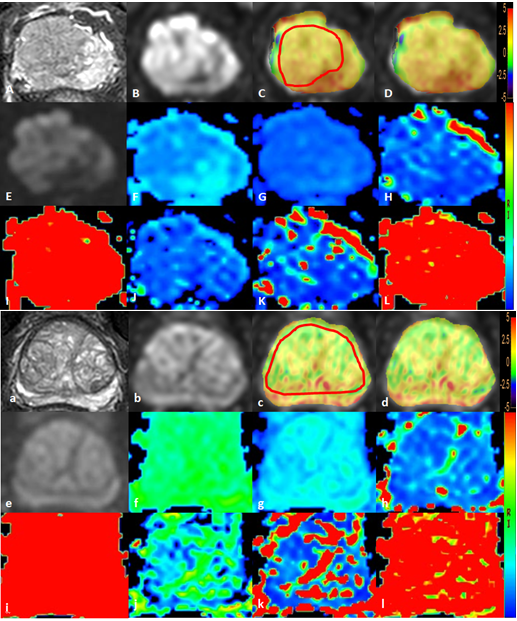
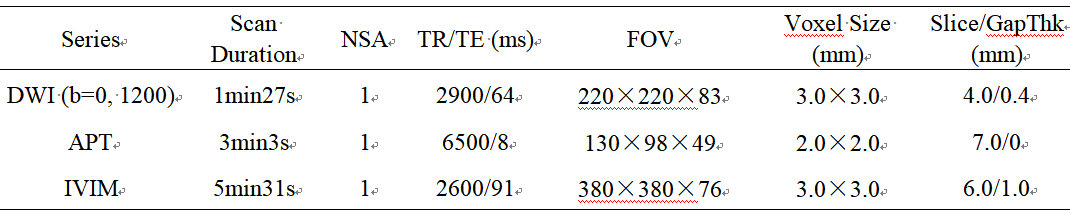
The study was approved by the institutional IRB. A total of 54 patients were prospectively included. According to pathology results, the patients were categorized into two groups: Group A prostate cancers (n=21, mean age 68.95±6.68 years, range 58-84 years) and Group B benign prostate hyperplasia (mean age 67.97±7.76 years, range 48-84 years). All the patients underwent MRI at 3.0T (Ingenia CX, Philips Healthcare, the Netherlands) with a 16-channel abdominal coil. The MR protocol included: DWI, APT, and IVIM, parameters detailed in Table 1. After the MRI scanning is completed, all data were interpreted independently by two radiologists (CM and LC, with 2 and 5 years of experiences respectively, blinded to the clinical information of the patients). Regions of interest (ROIs) were manually placed on the hyperintense signal area of DWI slice with the largest lesion demonstration. Then APT images were fused onto the DWI images to ensure the ROI measurement at the same position (Figure 1). The average APT values (MTRasym) and parameter values of IVIM were calculated to reduce measurement error. Inter-observer consistency of all the values was tested using intra-class correlation coefficients (ICC) with SPSS (IBM). All the parameter values between two Groups were detected using the t test. Logistic regression and ROC plot were used to evaluate the differential diagnostic efficiency of malignant tumours. Delong test was used to compare the diagnostic efficacy.Results
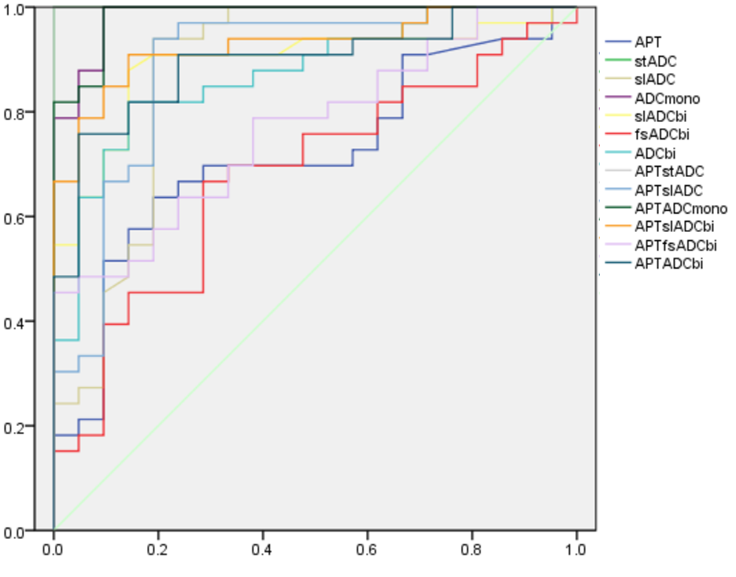
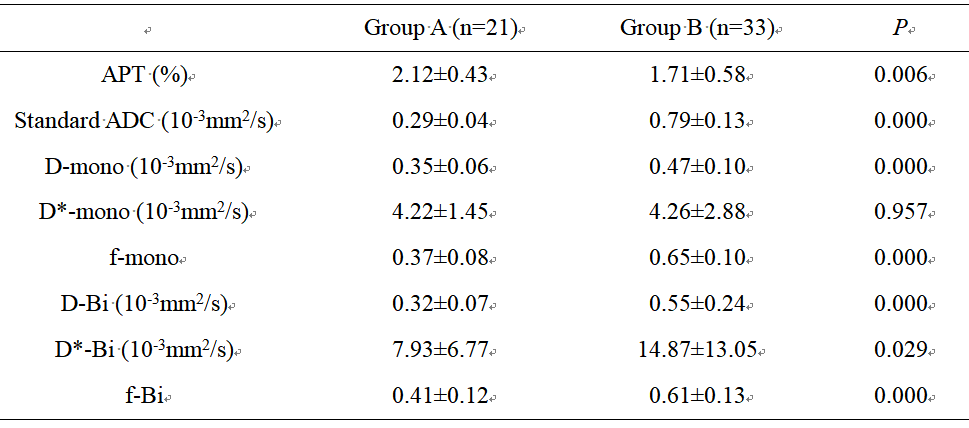
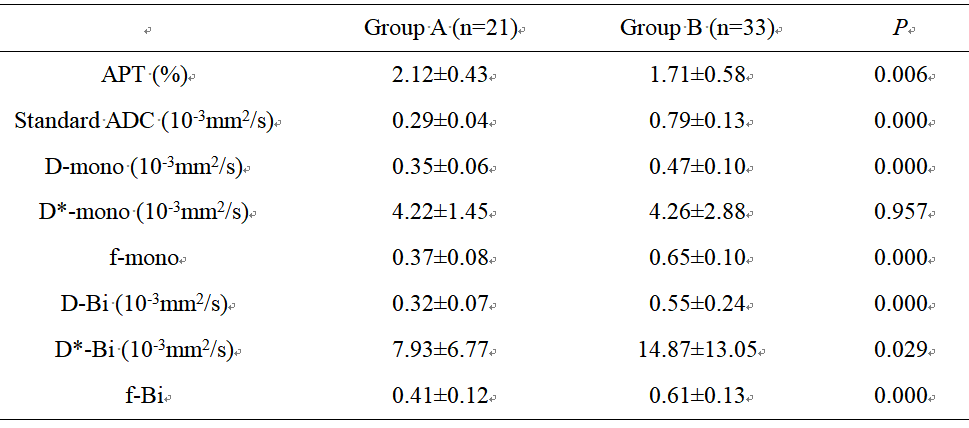
The measurement consistency between the two radiologists was good (ICC> 0.75, data not shown). APT values in Group A was significantly higher than in group B (P<0.05), diffusion and perfusion parameters (D-mono, D-Bi, D*-mono, D*-Bi, f-Bi, et al) of IVIM in Group A was significant lower than in group B (P<0.05, Table 2). As for ROC curves, the AUC values of all the parameters were more than 0.7. The diagnostic efficiency of APT combining with parameters of IVIM was higher than those of either APT or IVIM parameters if used separately (Table 3, Figure 2).Discussion and Conclusion
Significantly higher APT and lower diffusion and perfusion parameters in prostate cancers were observed than in benign prostate hyperplasia, which might be attributed to higher proliferation rate, elevated cancer cells metabolism, and more dense and more complicated microstructure in the cancers. In conclusion, APT together with IVIM may provide a non-invasive tool to distinguish prostate cancers and benign prostate hyperplasia.Acknowledgements
No acknowledgement found.References
[1] Murat Beyhan, Recep Sade, Erdem Koc, Senol Adanur, Mecit Kantarci. The evaluation of prostate lesions with IVIM DWI and MR perfusion parameters at 3T MRI. La Radiologia medica. 2019; 124(2):87-93.[2] Ying Liu, Xuan Wang, Yadong Cui, Yuwei Jiang, Lu Yu, Ming Liu, Wei Zhang, Kaining Shi, Jintao Zhang, Chen Zhang, Chunmei Li, Min Chen. Comparative Study of Monoexponential, Intravoxel Incoherent Motion, Kurtosis, and IVIM-Kurtosis Models for the Diagnosis and Aggressiveness Assessment of Prostate Cancer. Frontiers in Oncology. 2020;10:1763.[3] Zhou J, Heo HY, Knutsson L, et al. APT-weighted MRI: Techniques, current neuro applications, and challenging issues.J MagnReson Imaging. 2019; 50(2):347-364.
Figures