3878
The feasibility of the combination of APT and DCE in preoperative risk assessment of endometrial carcinoma
Ye Li1, Shifeng Tian1, Ailian Liu1, Jiazheng Wang2, and Peng Sun2
1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijin, China
1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijin, China
Synopsis
Preoperative risk assessment of endometrial carcinoma (EC) is crucial to therapy planning. The present study explores the feasibility of the combination of APT and DCE in preoperative risk assessment of endometrial carcinoma. Compared with low-risk EC, the APT values and volume transfer constant (Ktrans) derived from DCE in high-risk EC increased significantly. Our results suggest that both APT and Ktrans can differentiate high-risk EC and low-risk EC. However, a combination of APT and DCE does not improve the AUC statistically significantly.
Introduction
Surgery remains the first-line treatment for endometrial carcinoma (EC). For surgery planning, patients need to be classified as high-risk or low-risk according to the pathology and tumor invasiveness, which determines whether systemic lymph node dissection is required [1]. Amide proton transfer-weighted (APTw) MRI is sensitive to endogenous proteins and peptides in tissues[2]. DCE-MRI has been extensively used for diagnosis, prognosis and therapy tracking of various diseases including cancer[3]. Several quanfication parameters, the volume transfer constant (Ktrans), exchange rate between EES and blood plasma (Kep), extravascular volume fraction (Ve) and plasma volume fraction (Vp) derived from DCE reflect status of tissue, which is sensitive to tumor. This study aimed to investigate the potential of a combination of APT and DCE in the preoperative risk assessment of EC.Methods
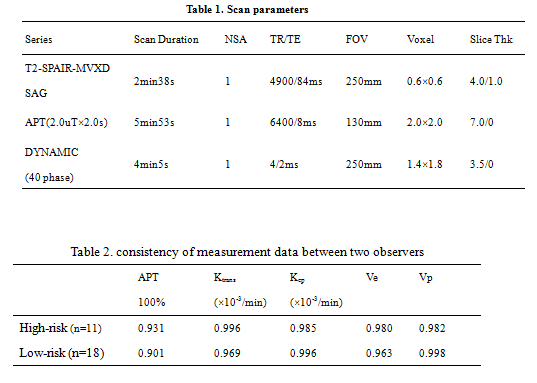
This retrospective study was approved by the institutional IRB and the written informed consent was waived. 29 patients with surgery-confirmed EC were included, who underwent pre-operative 3.0T MRI examination (Ingenia CX with a 16-channel abdominal coil, Philips Healthcare, Best, the Netherlands) including 3D APTw imaging and DCE imaging (Table 1). The patients were categorized into high-risk (n=11) group and low-risk (n=18) group based on the surgical pathology. ROIs were drawn independently by two radiologists (10 and 12 years of radiology experiences respectively) on the DCE images on the slice that shows the largest lesion area(Figure 1). The ROI-based mean APT, Ktrans, Kep, Ve, and Vp values and the standard deviations were calculated. The measurement consistency between the two observers was evaluated using intra-class correlation coefficients (ICC). The APT, Ktrans, Kep, Ve and Vp values of the high- and low-risk groups were compared using the Mann-Whitney U test. The differential diagnosis performance of APT and DCE parameters was evaluated with ROC curves. The Delong test was used to compare the diagnostic efficacy.RESULTS
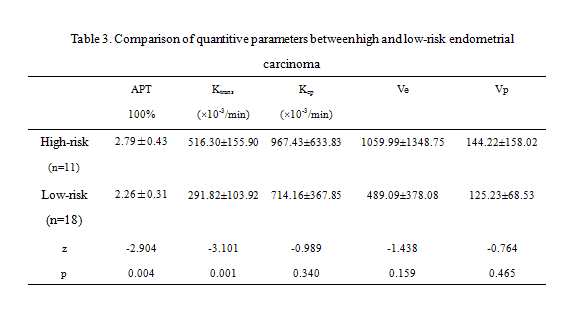
The interobserver measurement agreement for APT, Ktrans, Kep, Ve, and Vp values was good (Table 2). The Ktrans values in the high-risk group were significantly higher than in the low-risk group (p < 0.05, Table 3), and there were no statistical differences for Kep, Ve and Vp values s in the two groups (Table 3). For the diagnosis of high-risk EC, APT and Ktrans yielded an AUC of 0.816, 0.848 with a cut-off value at 2.775%, 372.51×10-3/min (Figure 2). The sensitivity and specificity were 63.6% and 94.4%, 90.9% and 72.2%, respectively. The AUC of the combination of APT values and Ktrans was 0.909. (Figure 2). However, no statistical improvement was detected compared with independent use of APT or Ktrans.Discussion
High-risk EC is associated with high Ki-67 and elevated expression of VEGF [4], which leads to a high proliferation rate of tumor cells, exuberant protein synthesis. This explains why APTw values in High-risk EC are higher than those in Low-risk EC. The endothelial transfer constant (Ktrans) reflects the microvascular changes in the lesion area, and the Ktrans value in the tumor area is markedly increased compared with that in normal tissue, which suggests the vascular permeability changes of the tumor tissues[5]. Our results demonstrate the Ktrans value of High-risk EC is higher than that of Low-risk EC. Therefore, both APT and Ktrans can differentiate high-risk EC and low-risk EC, which might be promising in clinical applications.Conclusions
Both APT and DCE-MRI are potentially promising methods in the preoperative risk assessment of EC.Acknowledgements
No acknowledgement found.References
[1] Marin F, Plesca M, Bordea CI, et al. Postoperative surgical complications of lymphadenohysterocolpectomy. J Med Life, 2014, 7(1):60-66. [2] Meng N, Wang J, Sun J, et al. Using amide proton transfer to identify cervical squamous carcinoma/adenocarcinoma and evaluate its differentiation grade. Magn Reson Imaging 2019, 61:9-15.[3] Kim HJJon, science. Variability in Quantitative DCE-MRI: Sources and Solutions. J Nat Sci. 2018;4(1):e484.[4] Yu CG, Jiang XY, Li B, et al. Expression of ER, PR, C-erbB-2 and Ki-67 in Endometrial Carcinoma and their Relationships with the Clinicopathological Features. Asian Pac J Cancer Prev, 2015, 16(15):6789-6794.[5] Jianzhi Li, Feng Xue, Xinghua Xu, Qing Wang, Xuexi Zhang. Dynamic contrast-enhanced MRI differentiates hepatocellular carcinoma from hepatic metastasis of rectal cancer by extracting pharmacokinetic parameters and radiomic features. Exp Ther Med. 2020 Oct; 20(4): 3643–3652.Figures
Table
Table
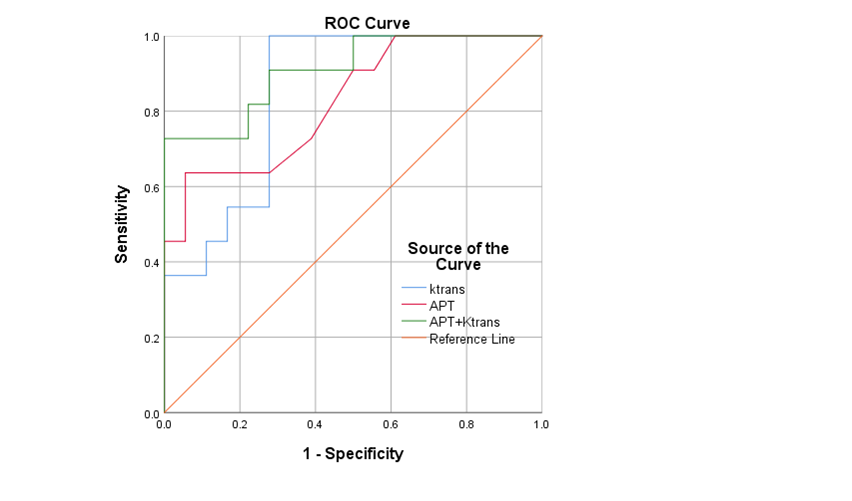
Figure 1. ROC curves of APT, Ktrans and a combination of APT and Ktrans value
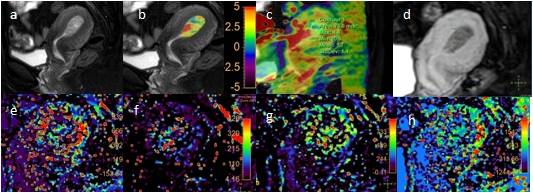
Figure 2 A 39 year-old woman with stage Ia endometrial cancer (low risk group), a is the T2WI image. b is the fusion image of APT and T2WI.c is the ROI position in APT image. d is ROI position in DCE-MRI image. e is ktrans image, f is kep image, g is ve image, h is hep image.