3873
Uterine cervical adenocarcinomas associated with lobular endocervical glandular hyperplasia: MR imaging manifestations
Mayumi Takeuchi1, Kenji Matsuzaki2, and Masafumi Harada1
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Radiological Technology, Tokushima Bunri University, Sanuki, Japan
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Radiological Technology, Tokushima Bunri University, Sanuki, Japan
Synopsis
Lobular endocervical glandular hyperplasia (LEGH) is considered as a precursor lesion of cervical adenocarcinomas with poor prognosis, and early diagnosis on MRI is important. MRI of 9 LEGH-associated adenocarcinomas (LEGH-ACs) and 10 LEGHs were retrospectively evaluated. Both LEGH-AC and LEGH appeared as multicystic masses with solid components. 4 of 9 LEGH-ACs (44%) showed diffusion restriction, whereas 5 of 9 LEGH-ACs (56%) and all LEGHs showed no diffusion restriction. On DCE-MRI, 4 of 4 LEGH-ACs (100%) and 2 of 6 LEGHs (33%) showed rapid and prolonged contrast-enhancement pattern, whereas 4 of 6 LEGHs (66%) showed gradual contrast-enhancement pattern suggesting their benignity.
Introduction
Lobular endocervical glandular hyperplasia (LEGH) is a benign cervical lesion, and excessive surgical procedure should be avoided in patients of reproductive age to preserve fertility. LEGH has been considered as a precursor lesion of cervical adenocarcinomas, especially of gastric-type adenocarcinoma (GAS), and early diagnosis is directly linked to improved prognosis, thus making imaging diagnosis an important role 1. GAS including minimal deviation adenocarcinoma (MDA) is a subtype of cervical adenocarcinomas with poor prognosis that occurs more frequently in young women, and is characterized by the absence of human papillomavirus (HPV) infection in its pathogenesis 2-4. The purpose of this study was to evaluate the capability of MR imaging for the diagnosis of LEGH-associated uterine cervical adenocarcinoma (LEGH-AC).Methods
MR imaging features of pathologically proven 9 LEGH-ACs (5 GAS; 2 MDA; 2 Adenocarcinomas, NOS) (Table 1) were retrospectively evaluated. All patients were studied by using 3T (4 patients) or 1.5T (5 patients) superconducting MRI units with body coil transmission and phased-array receiver. T2WI, T1WI and DWI (b=800 s/mm2) were obtained in all 9 lesions. The contrast-enhanced study was performed in 7 patients (including dynamic contrast-enhanced (DCE) MRI study in 4 patients). The parameters of each sequence varied because this study was retrospective and involved a long study period (2007 to 2020). The ADC measurement was performed and computed DWI (b=1500 s/mm2) was synthesized on the workstation (Ziostation2, Ziosoft) in all 9 lesions. MR imaging features of pathologically proven 10 benign LEGH (Table 2) were also evaluated as comparisons.Results and Discussions
On T2WI, all LEGH-ACs appeared as multicystic masses with large or small solid components. The solid components showed slight high signal intensity with/without sponge-like appearance reflecting tiny glandular cysts on T2WI (Fig. 3, 4). The solid components of all 7 lesions with contrast-enhancement study showed contrast-enhancement (weak 5; intense 2, compared with the myometrium), and all 4 lesions with DCE-MRI showed rapid and prolonged contrast-enhancement pattern (Fig. 3, 4). All 9 lesions showed increased signal intensity on DWI (high 5, slight high 4), and 5 of 9 lesions showed significant signal decrease on computed DWI with higher b-value (1500 s/mm2) (Fig. 4). Mean ADC value of all 9 lesions was 1.84 +/- 0.44 x 10-3 mm2/s. The mean ADC value of 5 lesions with significant signal decrease on computed DWI (2.16 x 10-3 mm2/s) was higher than that of the other 4 lesions without significant signal decrease (1.44 x 10-3mm2/s) (p<0.05).On the other hand, all LEGH appeared as multicystic masses with low to slight high signal intensity sponge-like solid components on T2WI. The solid components of all 10 lesions showed contrast-enhancement (weak 6; intense 4, compared with the myometrium), and 6 lesions with DCE-MRI showed rapid and prolonged contrast-enhancement pattern (2 lesions) or gradual contrast-enhancement pattern (4 lesions) (Fig. 5). LEGH showed increased signal intensity on DWI (slight high: 7 lesions) or iso intensity (3 lesions), and all 10 lesions showed significant signal decrease on computed DWI with higher b-value (1500 s/mm2) (Fig. 5). Mean ADC value of 10 lesions was 2.07 +/- 0.23 x 10-3 mm2/s. There was no statistically difference between ADC values of 10 LEGH-ACs and 10 LEGHs, however, ADC value of 4 LEGH-ACs which did not show signal decrease on computed DWI (b=1500) was significantly lower than that of LEGH (p<0.01).
In this study, the presence of multicystic area in LEGH-AC may suggest co-existing LEGH, and the solid component exhibiting water diffusion restriction may be suggestive for carcinomatous component. However, this finding was observed in 4 of 9 LEGH-ACs (44%) and the other 5 lesions (56%) showed increased signal intensity on DWI possibly due to T2 shine-through effect reflecting abundant mucinous material-filled tiny cystic components within the tumor. Whereas 7 of 10 LEGHs also showed increased signal intensity on DWI possibly due to T2 shine-through effect reflecting mucinous material-filled aggregated tiny cysts and may be undifferentiable from LEGH-AC. Ohya et al. evaluated DWI of 7 LEGH-ACs and diffusion restriction was observed in 4/7 lesions (57%) 5. These results suggest that there might be the limitation in differentiating LEGH-AC and benign LEGH based on DWI. All 4 LEGH-ACs (100%) and 2 of 6 LEGH (33%) with DCE-MRI showed rapid and prolonged contrast-enhancement pattern, whereas no LEGH-ACs and 4 of 6 LEGHs (66%) showed gradual contrast-enhancement pattern which may be suggestive for benign lesions without angiogenesis.
Conclusion
We conclude that uterine cervical multicystic mass with diffusion restricted solid components may be suggestive for LEGH-AC, and computed DWI with higher b-value may be helpful for the diagnosis. Some LEGH may be undistinguishable from LEGH-AC on unenhanced MRI including DWI, gradual contrast-enhancement pattern on DCE-MRI may be suggestive for their benignity.Acknowledgements
No acknowledgement found.References
- Takatsu A, et al. Preoperative differential diagnosis of minimal deviation adenocarcinoma and lobular endocervical glandular hyperplasia of the uterine cervix: a multicenter study of clinicopathology and magnetic resonance imaging findings. Int J Gynecol Cancer. 21:1287-1296, 2011.
- Mikami Y. Gastric-type mucinous carcinoma of the cervix and its precursors - historical overview. Histopathology 76:102-111, 2020.
- Holl K, et al. Human papillomavirus prevalence and type-distribution in cervical glandular neoplasias: Results from a European multinational epidemiological study. Int. J. Cancer 137:2858-2868, 2015.
- Nishio S, et al. Analysis of gastric-type mucinous carcinoma of the uterine cervix — An aggressive tumor with a poor prognosis: A multi-institutional study. Gynecol Oncol 153:13-19, 2019.
- Ohya A, et al. Uterine cervical adenocarcinoma associated with lobular endocervical glandular hyperplasia: Radiologic–pathologic correlation. J Obstet Gynaecol Res. 44:312-322, 2018.
Figures
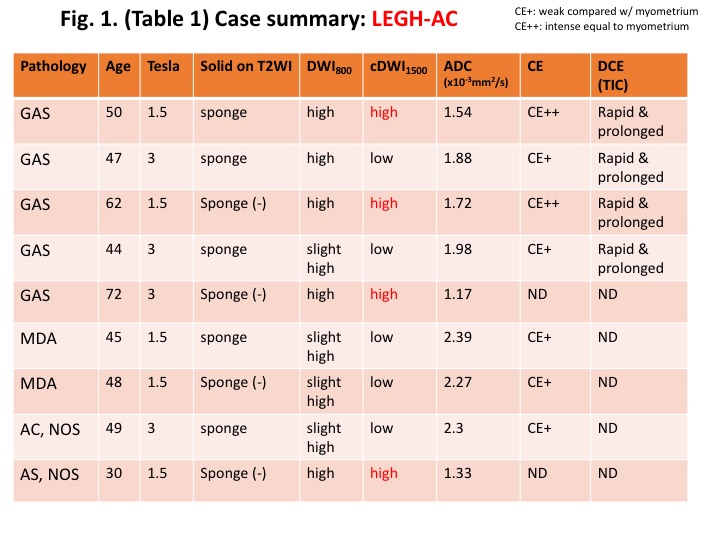
Table. 1. Case summary: LEGH-AC (LEGH-associated adenocarcinoma)
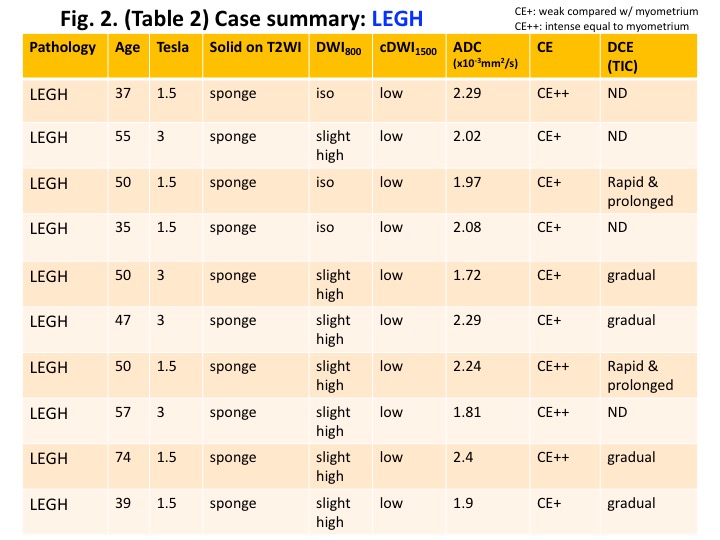
Table. 2. Case summary: LEGH
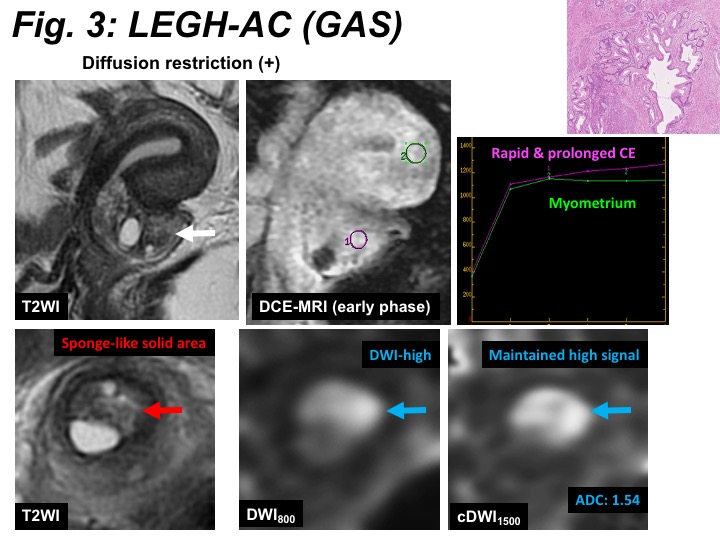
LEGH-AC: Multicystic mass with solid components exhibiting sponge-like slight high intensity on T2WI, high intensity on DWI with relatively low ADC (1.54 x 10-3mm2/s), maintained high signal intensity on computed DWI (b=1500s/mm2) suggesting diffusion restriction, and rapid & prolonged contrast-enhancement pattern on DCE-MRI.
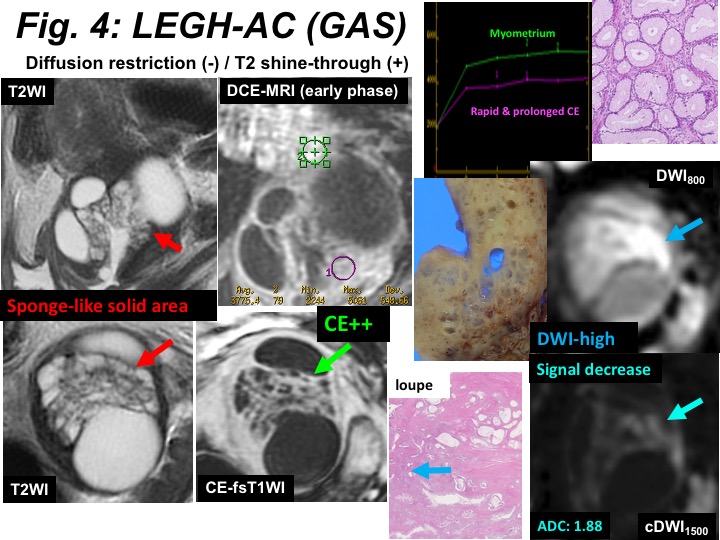
LEGH-AC: Multicystic mass with solid components exhibiting sponge-like slight high intensity on T2WI, intense contrast-enhancement on CE-fsT1WI, high intensity on DWI with relatively high ADC (1.88 x 10-3mm2/s), decreased signal intensity on computed DWI (b=1500s/mm2) suggesting T2 shine-through effect, and rapid & prolonged contrast-enhancement pattern on DCE-MRI.
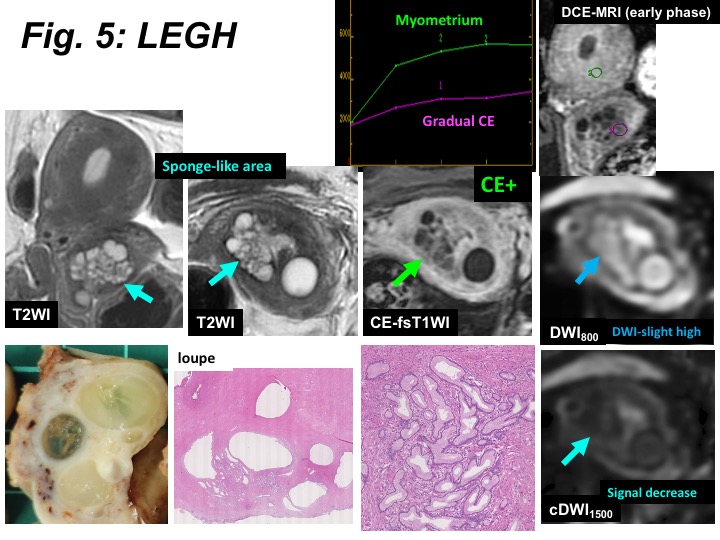
LEGH: Multicystic mass with solid components exhibiting sponge-like slight high intensity on T2WI, high intensity on DWI with relatively high ADC (2.29 x 10-3mm2/s), decreased signal intensity on computed DWI (b=1500s/mm2) suggesting T2 shine-through effect, and gradual contrast-enhancement pattern on DCE-MRI.