3865
Quantitative evaluation of infrapatellar fat pad in knee osteoarthritis by using hydrogen proton MR spectroscopy (1H-MRS)1Department of Medical Imaging, The Third Affiliated Hospital of Southern Medical University, Guangzhou, China, 2China International Center, Philips Healthcare, Guangzhou, China
Synopsis
Infrapatellar fat pad (IPFP) is an adipose structure of knee joint, which plays an important role in the progression of knee osteoarthritis(KOA). In this paper, we evaluate the fat content and composition of the IPFP in normal subjects and different stages of knee osteoarthritis patients using hydrogen proton MR spectroscopy (1H-MRS). In addition, we investigate the relationship between the fat content and composition of the IPFP and Hoffa-synovitis. The results showed that the quantitative parameters of the IPFP by MRS were correlated with the progression of KOA and Hoffa-synovitis.
Introduction and Purpose
The infrapatellar fat pad (IPFP), also known as Hoffa’s fat pad, is an intracapsullar and extrasynovial adipose tissue structure in the knee joint[1] . IPFP has become a focus of growing interest in recent years for two main reasons: adipose-derived stem cells are being evaluated for their ability to induce cartilage repair, and a role for the IPFP in the pathogenesis of osteoarthritis is being considered[2]. Hoffa-synovitis are emerging as potentially important imaging biomarkers in knee osteoarthritis (KOA), and have been associated with pain, cartilage thinning, bone marrow lesions (BML),etc[3]. Adipose tissue not only secretes adipokines and cytokines but also lipids. The main lipids secreted in this process are fatty acids released in the process of lipolysis. Interestingly, fatty acids not only are an important source of energy for tissues but also display immune modulatory properties [4] . However, the characteristics of fatty acids for IPFP in KOA has not been clear. The purpose of this study is to quantitatively assess the change of fat content and fat composition in different periods of KOA and describe their associations with Hoffa-synovitis using the non-invasive hydrogen proton MR spectroscopy (1H-MRS), which is based on measuring the relative amplitudes of the peaks in the fat spectrum.Materials and Methods
For this prospective study, a total of forty-five subjects including both healthy volunteers (n=15) and the patients with knee osteoarthritis (n=30) who underwent X-ray of the knee were divided into three groups (normal (K/L=0, n=15), mild OA (K/L=1-2, n=15), and advanced OA (K/L=3-4, n=15)) based on Kellgren-Lawrence (K/L) grade. 1H-MRS of the IPFP were performed to calculate the fat content and composition. Lipid (1.3 ppm) to water (4.7 ppm) ratio (LWR) and fat fractions (FF) were measured. Unsaturation index (UI) was calculated as the ratio of the sum of unsaturated fat peaks including 2.05 ppm, 2.25ppm, 4.2ppm and 5.3ppm to all lipid peaks including the methylene protons (-(CH2) n-) at 1.3 ppm in addition to the above-mentioned four unsaturated fat peaks (Figure 1) . Moreover, the Hoffa-synovitis was semi-quantitatively evaluated using the MRI Osteoarthritis Knee Score (MOAKS) on proton density-weighted spectral attenuated inversion recovery (PDW-SPAIR) images. The LWR, FF and UI values of IPFP were compared between three groups and correlated with the Hoffa-synovitis scores .Results
The mean age of normal group, mild OA group and advanced group was 54 ± 3 years old, 56 ± 4 years old and 57 ± 6 years old,respectively (P > 0.05). The mean BMI in the three group was 24.3 ± 2.8 kg/m2, 25.8 ± 3.0 kg/m2 and 27.4 ± 3.1 kg/m2,respectively (P<0.05). Other detailed characteristics were listed in table 1. Table 2 show the LWR, FF and UI of IPFP were all significantly decreased in the advanced OA group when compared with that of the mild OA group and the normal group (P<0.05). After controlling BMI, the differences of LWR,FF and UI among the three groups were still statistically significant (P<0.05).The Hoffa-synovitis scores were negatively correlated to the LWR, FF, and UI values of IPFP (r = -0.687, -0.687,-0.535,P<0.01) (Figure 2).Conclusions
With the progression of KOA, the fat content and Unsaturated fatty acid of the IPFP decreased gradually. The LWR, FF and UI were significantly related to Hoffa-synovitis scores. 1H-MRS is helpful in quantitatively evaluating the IPFP changes in KOA and may be a new biomarker for KOA.Acknowledgements
Corresponding author: Xiaodong Zhang.
Funding: The National Natural Science Foundation of China (grant No.81801653).
References
[1] O'Donnell BT, Al-Ghadban S, Ives CJ ,et al. Adipose Tissue-Derived Stem Cells Retain Their Adipocyte Differentiation Potential in Three-Dimensional Hydrogels and Bioreactors (dagger)[J].Biomolecules, 2020, 10(7):
[2] Abramoff B, Caldera FE. Osteoarthritis[J].Med. Clin. North Am., 2020, 104(2): 293-311.
[3] de Vries BA, van der Heijden RA, Poot DHJ ,et al. Quantitative DCE-MRI demonstrates increased blood perfusion in Hoffa's fat pad signal abnormalities in knee osteoarthritis, but not in patellofemoral pain[J].Eur. Radiol., 2020, 10.1007/s00330-020-06671-6:
[4] Zapata-Linares N, Eymard F, Berenbaum F ,et al. Role of adipose tissues in osteoarthritis[J].Curr. Opin. Rheumatol., 2021, 33(1): 84-93.
Figures
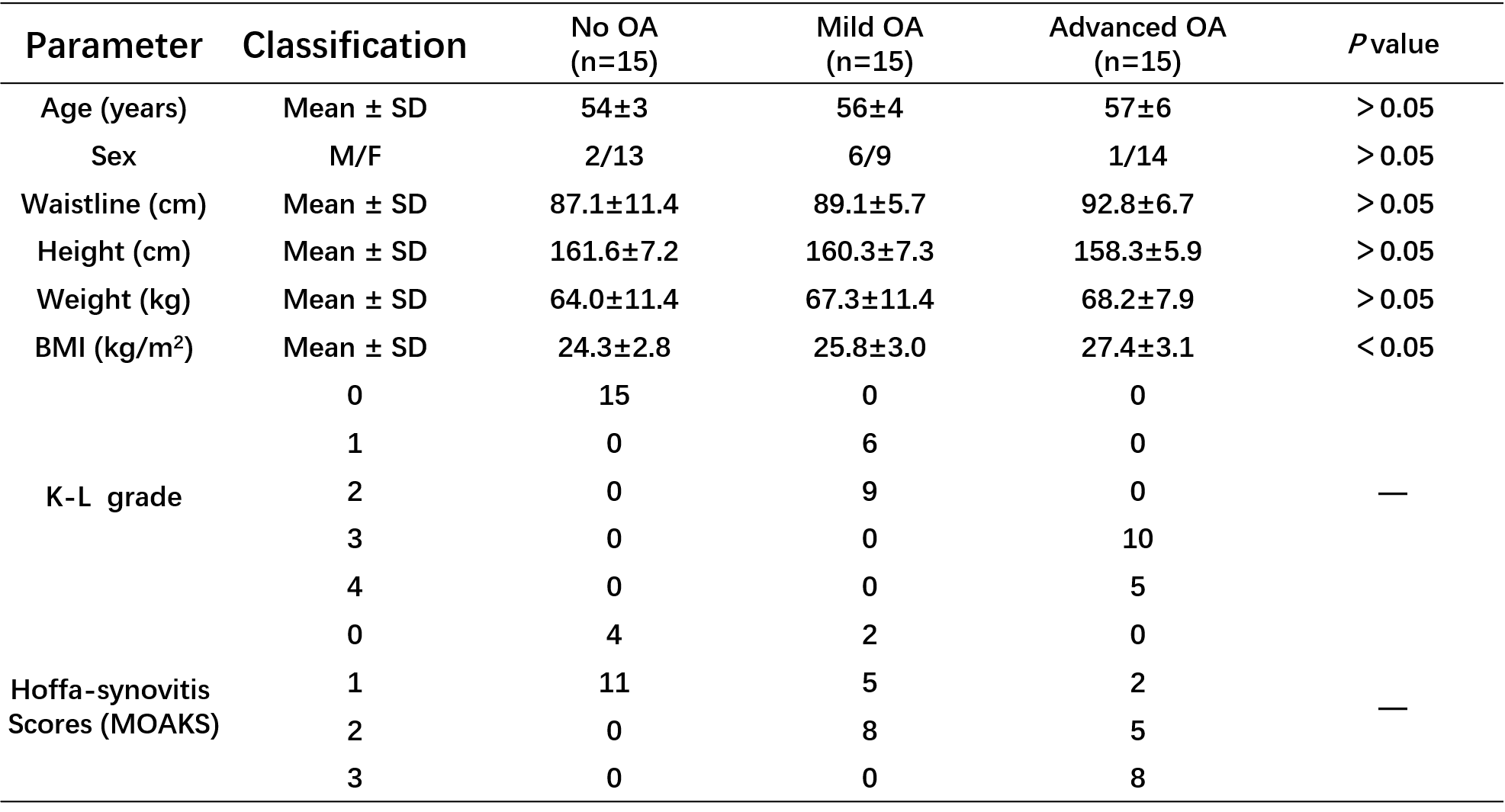
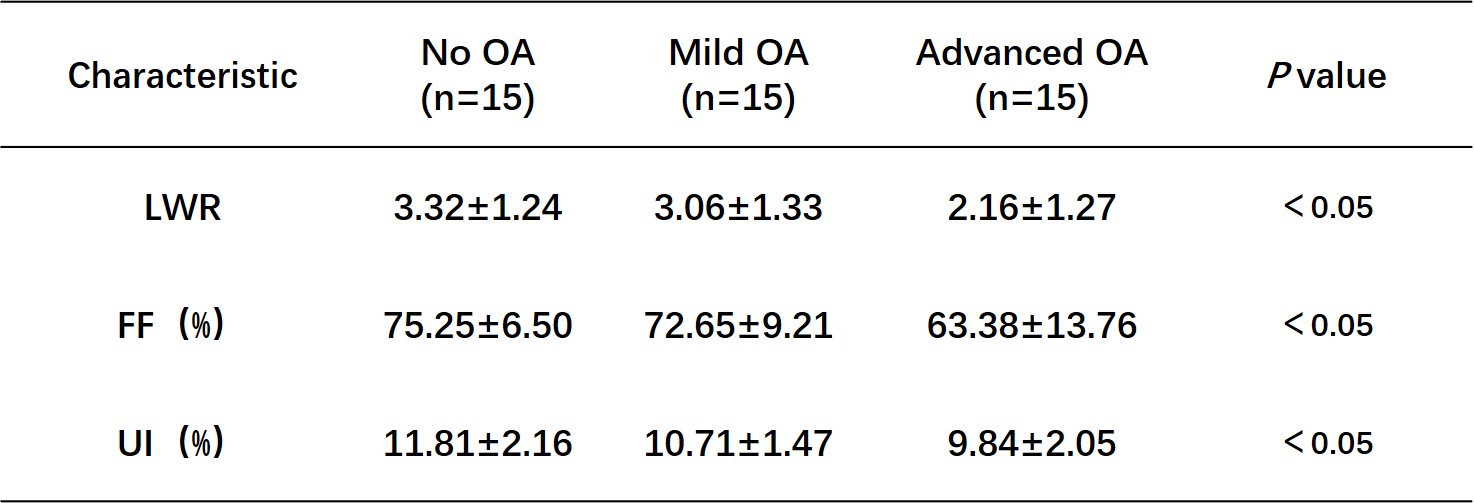
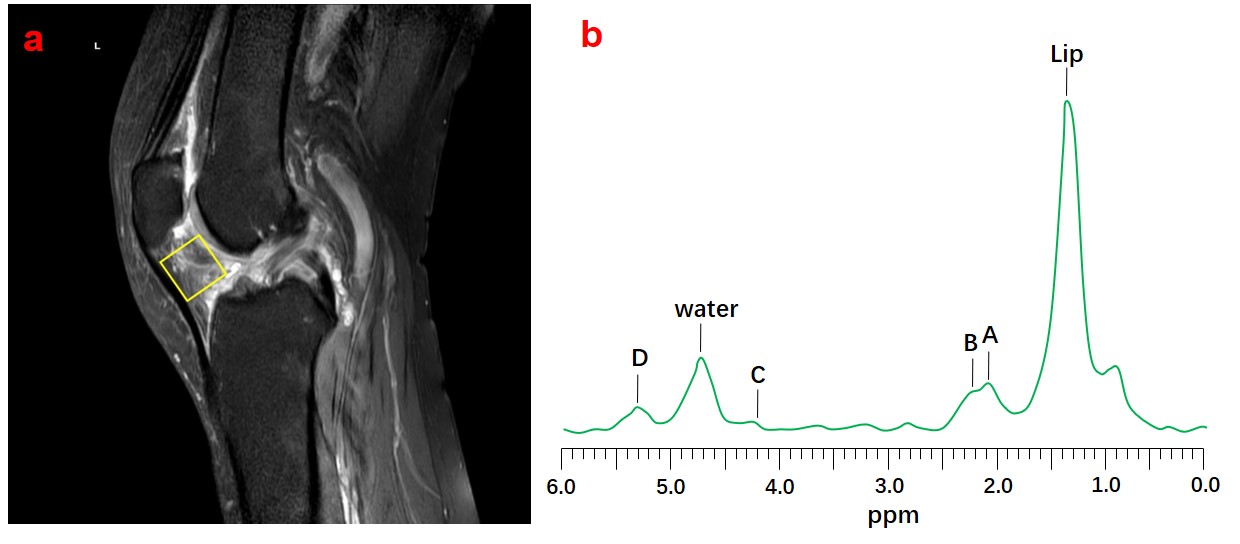
Fig 1. The measurement of LWR , FF and UI values using MRS
Note: a. The ROIs were placed centrally in each IPFP;b. A, B, C and D are unsaturated fat peaks 2.05 ppm, 2.25ppm, 4.2ppm and 5.3ppm , respectively.
Lipid-water ratio (LWR) = Lipid peak amplitude/Water peak amplitude;
Fat fraction (FF%)=AreaLip / (AreaLip+ AreaH2O)×100;
Unsaturation Index (UI%) = (A+B+C+D)/(A+B+C+D+Lip) ×100.
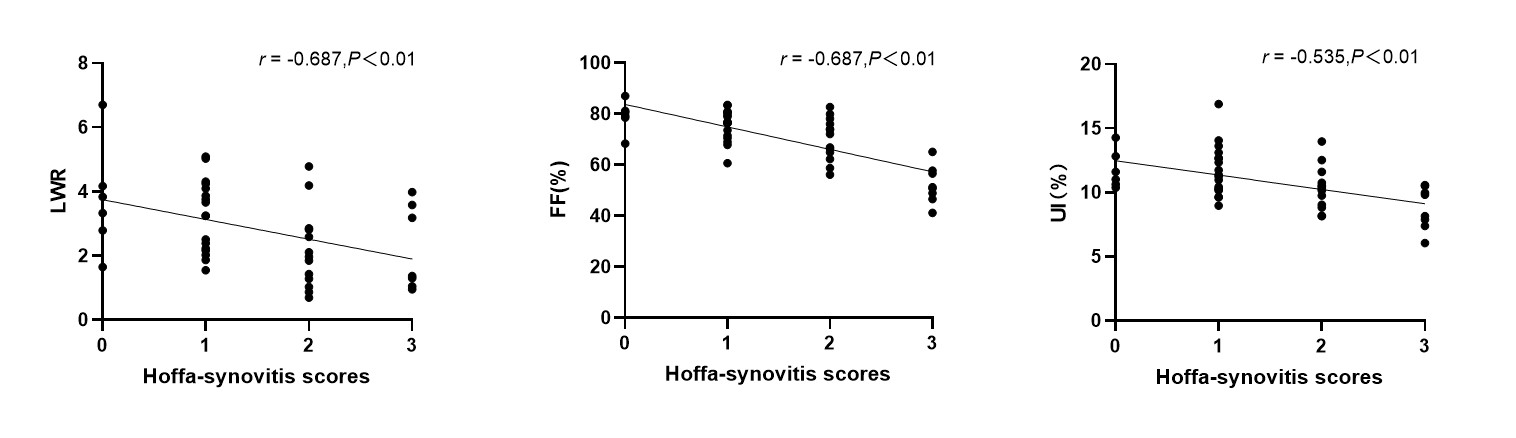
Fig 2. Scatterplots between the LWR , FF and UI and Hoffa-synovitis