3835
MRI-Based Fat Fraction of Psoas and Puborectalis Muscle Increases with Severity of Rectal Prolapse1Radiology, Stanford University, Palo Alto, CA, United States, 2Gastroenterology, Stanford University, Palo Alto, CA, United States, 3General Surgery, Stanford University, Palo Alto, CA, United States, 4Stanford University, Palo Alto, CA, United States
Synopsis
Pelvic floor disorders (PFDs) are a very common group of clinical conditions that affect nearly 50% of women aged 80 years or older. While pelvic floor disorders are thought to be associated with pelvic floor muscle weakness, there has not been an established correlation between sarcopenia and PFDs. This single institution, retrospective study evaluates the effect of decreased muscle quantity/quality on severity of pelvic organ prolapse. Our findings suggest increased psoas and puborectalis muscle fat fraction are associated with higher grades of pelvic organ prolapse.
Introduction
Pelvic floor disorders (PFDs) refer clinical conditions including pelvic organ prolapse, urinary and fecal incontinence, chronic constipation, and pelvic pain (1). PFDs are common with increasing prevalence with age: affecting nearly 50% of women aged 80 years or older (2). While the exact etiology of PFDs is unknown, a combination of anatomical, physiological, genetic, lifestyle, and reproductive factors likely interact to contribute to PFDs (3).Pelvic floor MRI is a recommended part of the standard pelvic floor evaluation (4). MR defecography allows multi-compartment evaluation of the pelvic floor with superior contrast resolution and without ionizing radiation compared to fluoroscopic defecography (5).
Pelvic floor physical therapy (PFPT) is a conservative option to treat pelvic floor dysfunction (6). While evidence based PFPT suggests PFDs are partly due to pelvic floor muscle weakness, there have been no studies describing the correlation between sarcopenia and PFDs. Several MRI biomarkers of sarcopenia have been studied, including psoas muscle cross-sectional area and fat fraction (7). The goal of this study was to establish a correlation between these biomarkers of sarcopenia and severity of rectal prolapse.
Methods
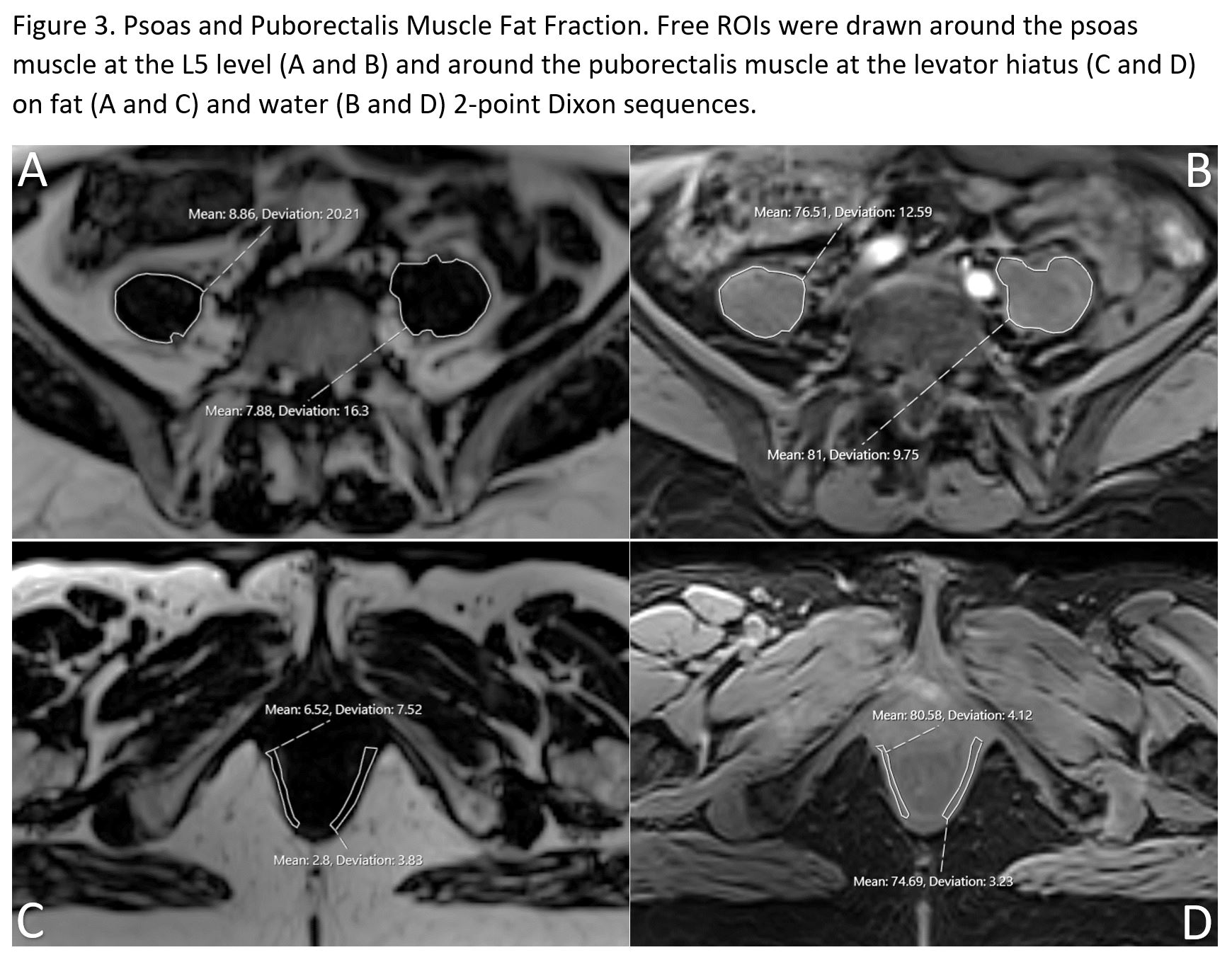
With institutional review board (IRB) approval, female patients who underwent a MR defecography from January 1, 2020 to November 15, 2020 were retrospectively reviewed at a single institution. All exams were individually reviewed, and pelvic organ descent/prolapse was reassessed. Patient demographics, H and M lines, levator hiatus width, and pelvic organ prolapse were recorded. Rectal intussusception/prolapse was graded using the Oxford Classification (8). In addition, the psoas muscle cross-sectional area and fat fraction at the L5 level was quantified by utilizing a 2-point Dixon technique. The puborectalis muscle cross-sectional area and fat fraction at the inferior pubic symphysis was also quantified using the same 2-point Dixon technique (Figure 3). Exclusion criteria included male patients, patients unable to defecate/dyssynergic defecation, patients with prior pelvic floor surgery, and if the 2-point Dixon was not included or not reliable.Results
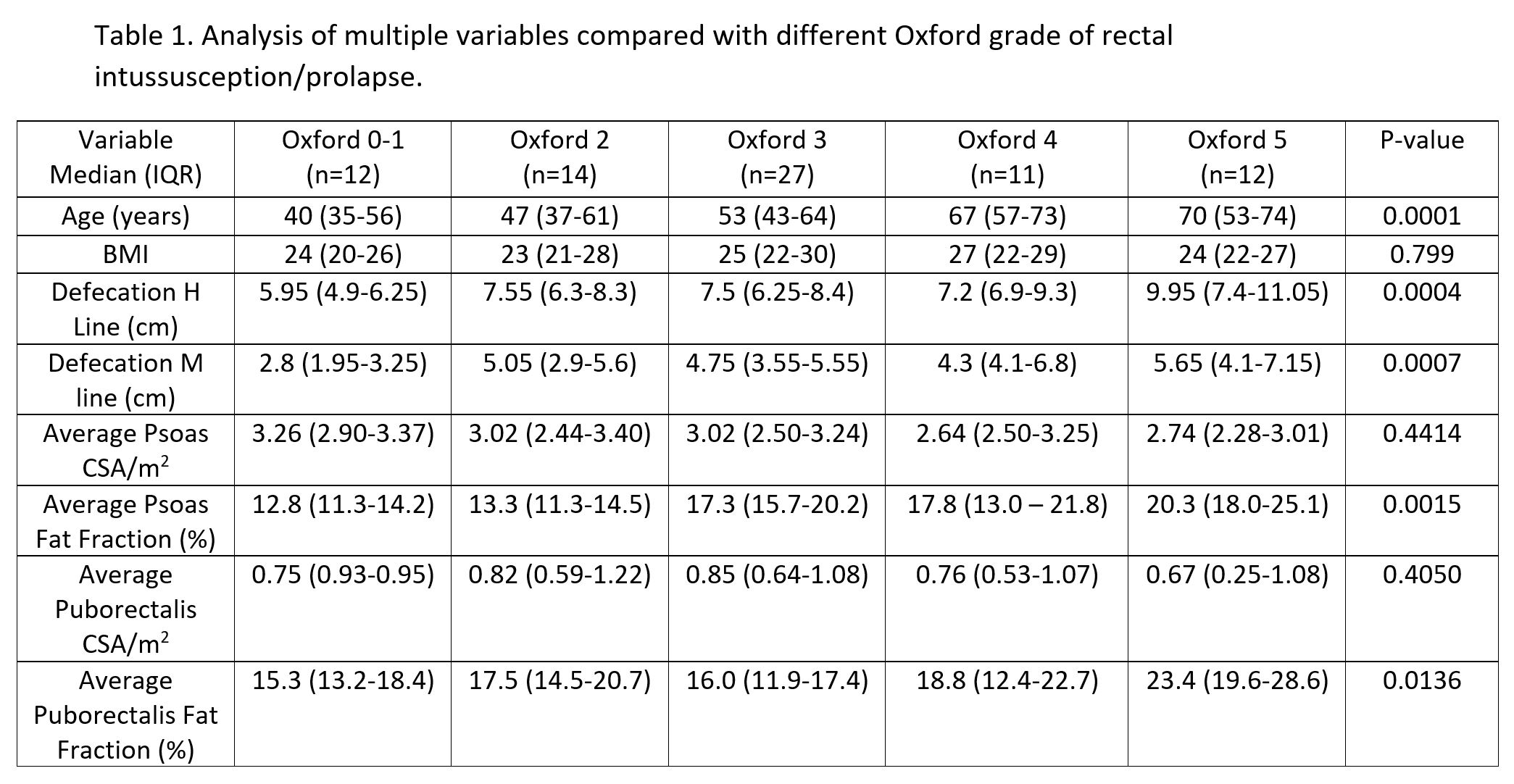
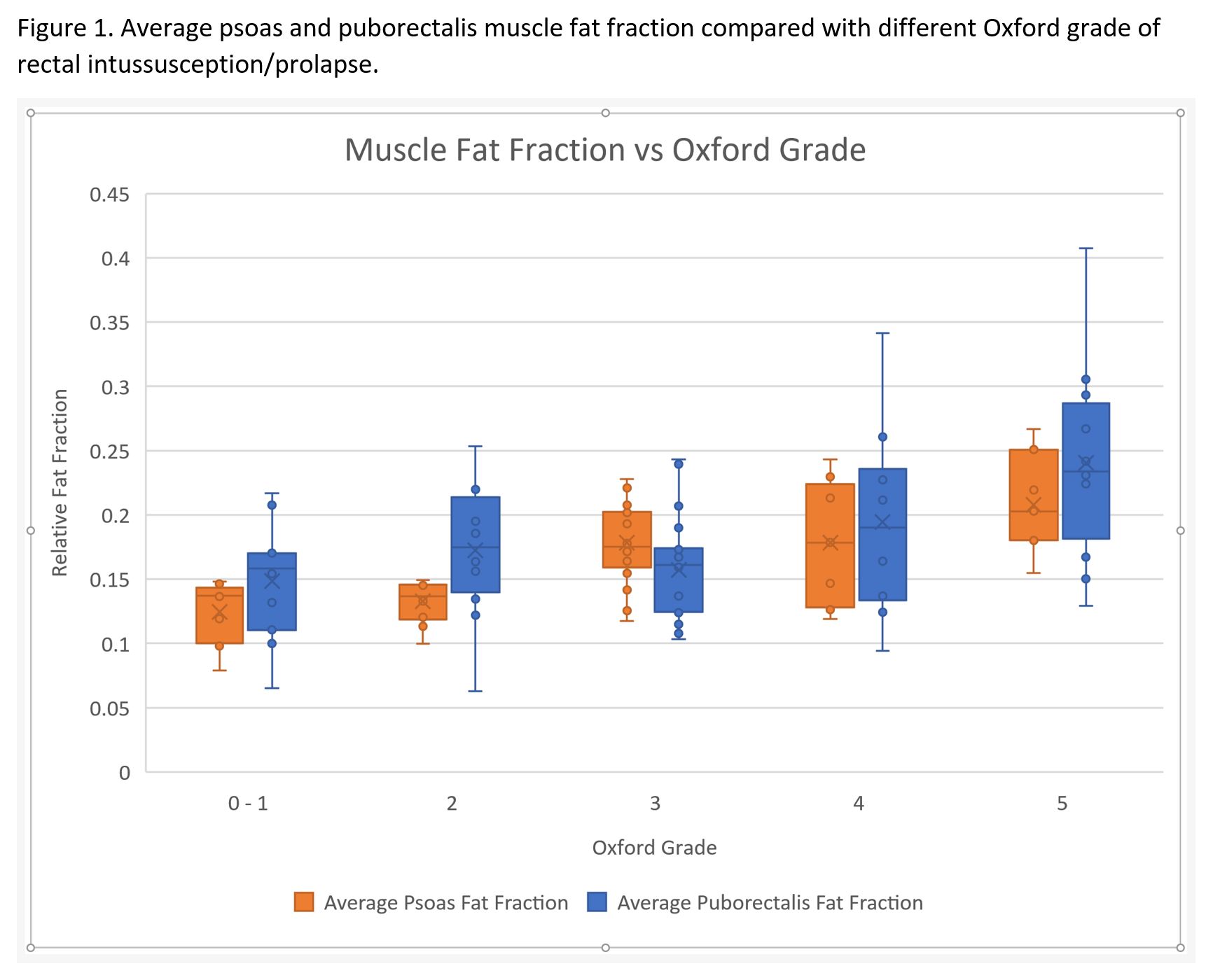
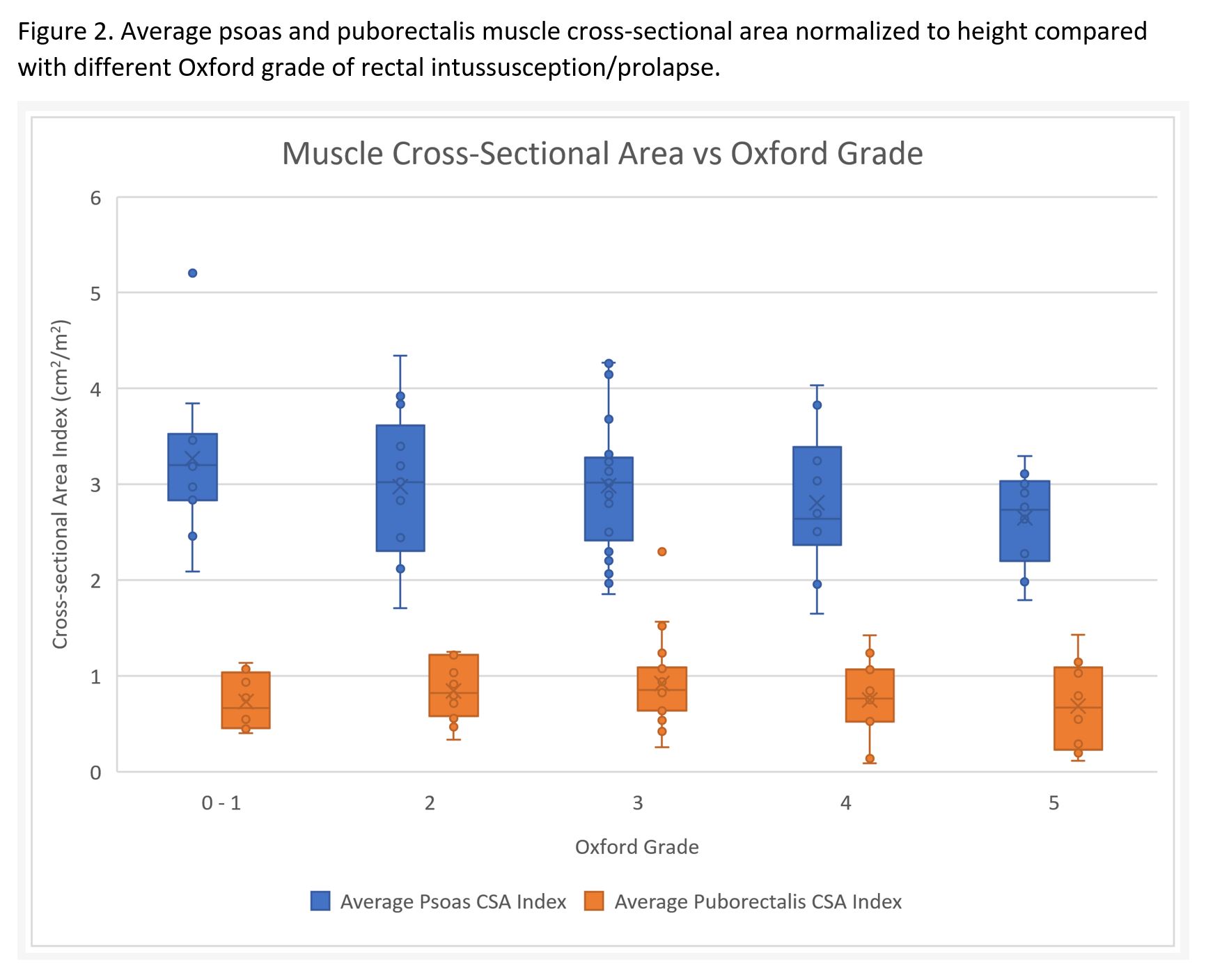
77 female patients were included with an average age of 54.8 years and average BMI of 24.9. Multiple variables and their relationship with Oxford radiological grading of rectal prolapse are displayed in Table 2. Age, defecation H/M lines, average psoas muscle fat fraction, and average puborectalis fat fraction were significantly different among patients with different degrees of rectal intussusception/prolapse (P < 0.05). Figure 1 displays the average psoas and puborectalis muscle fat fraction among different Oxford grade groups. BMI, average psoas muscle cross-sectional area index, and average puborectalis muscle cross-sectional area index did not show a significant difference among patients with rising grades of rectal intussusception/prolapse (P > 0.05). Figure 2 displays the average psoas and puborectalis muscle cross-sectional area normalized to height among different Oxford grade groups.Discussion
In the past decade, the importance of sarcopenia as a parameter of frailty has been shown (9). Patients with sarcopenia have higher risk of postoperative complications and mortality including cardiovascular complications when undergoing colorectal surgery (10-12). The European Working Group on Sarcopenia in Older People (EWGSOP) consensus definition of sarcopenia includes measures for three parameters: muscle strength, muscle quantity/quality, and physical performance as an indicator of severity. Validated measures of low grip strength are defined as < 26 kg for men and < 16 kg for women; and low lean body mass is defined as appendicular lean mass adjusted for height < 7.0 kg/m2 for men and < 6.0 kg/m2 for women or appendicular lean mass adjusted for BMI < 0.789 for men and < 0.512 for women (13-14). Dual-energy x-ray absorptiometry (DEXA) is the traditional method of measuring appendicular lean body mass (15). Multi-modality imaging biomarkers of sarcopenia have been proposed including different muscle cross sectional areas and fat fractions (16). Morrell et al, proposed psoas cross-sectional area measured at the vertebral level L4–L5 as an accurate predictor of sarcopenia (17).Our results indicate that psoas and puborectalis muscle fat fraction are associated with severity of rectal intussusception/prolapse. The psoas and puborectalis muscle cross sectional area did not have a significant correlation with rectal intussusception/prolapse. Several studies have shown the importance of measuring both muscle quantity and muscle quality in the assessment of sarcopenia (7,16, 18). Muscle quantity is measured as the cross-sectional area or muscle mass, while the muscle quality is measured as the muscle fat fraction. The loss of muscle strength occurs at least 2-4 times faster than the loss of muscle mass, which has been proposed to be partially related to the presence of muscle fat infiltration (14).
Age was also significantly correlated with severity of rectal intussusception/prolapse. This association is consistent with the increased prevalence of PFDs with age (19), and age-related muscle changes include skeletal muscle mass decline and muscle fat infiltration (20).
Conclusion
The severity of pelvic organ prolapse appears associated with MRI biomarkers of sarcopenia, relative psoas and puborectalis muscle fat fraction, may be evaluated during MR defecography exams with MRI-based fat fraction measurements and provide supplementary clinical information. Sarcopenia has been shown to be correlated with higher risk of postoperative complications and mortality. Future prospective research is needed to determine if sarcopenia may predict poor postsurgical outcomes after pelvic organ prolapse repair.Acknowledgements
No acknowledgement found.References
1. Savoye-Collet C, Koning E, Dacher JN. Radiologic evaluation of pelvic floor disorders. Gastroenterol Clin North Am. 2008 Sep;37(3):553-67.
2. Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, Schaffer J, Spino C, Whitehead WE, Wu J, Brody DJ, Pelvic Floor Disorders Network. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008 Sep 17;300(11):1311-6.
3. Delancey JO, Kane Low L, Miller JM, Patel DA, Tumbarello JA. Graphic integration of causal factors of pelvic floor disorders: an integrated life span model. Am J Obstet Gynecol. 2008 Dec;199(6):610.e1-5.
4. Lalwani N, Khatri G, El Sayed RF, Ram R, Jambhekar K, Chernyak V, Kamath A, Lewis S, Flusberg M, Scholz F, Arif-Tiwari H, Palmer SL, Lockhart ME, Fielding JR. MR defecography technique: recommendations of the society of abdominal radiology's disease-focused panel on pelvic floor imaging. Abdom Radiol (NY). 2019 Aug 05.
5. Ramage L, Simillis C, Yen C, Lutterodt C, Qiu S, Tan E, Kontovounisios C, Tekkis P. Magnetic resonance defecography versus clinical examination and fluoroscopy: a systematic review and meta-analysis. Tech Coloproctol. 2017 Dec;21(12):915-927.
6. Wallace SL, Miller LD, Mishra K. Pelvic floor physical therapy in the treatment of pelvic floor dysfunction in women. Curr Opin Obstet Gynecol. 2019 12;31(6):485-493.
7. Codari M, Zanardo M, di Sabato ME, Nocerino E, Messina C, Sconfienza LM, Sardanelli F. MRI-Derived Biomarkers Related to Sarcopenia: A Systematic Review. J Magn Reson Imaging. 2020 04;51(4):1117-1127.
8. Collinson R, Cunningham C, D'Costa H, Lindsey I. Rectal intussusception and unexplained faecal incontinence: findings of a proctographic study. Colorectal Dis. 2009 Jan;11(1):77-83.
9. Pinotti E, Montuori M, Borrelli V, Giuffrè M, Angrisani L. Sarcopenia: What a Surgeon Should Know. Obes Surg. 2020 May;30(5):2015-2020.
10. Barbalho SM, Flato UAP, Tofano RJ, Goulart RA, Guiguer EL, Detregiachi CRP, Buchaim DV, Araújo AC, Buchaim RL, Reina FTR, Biteli P, Reina DOBR, Bechara MD. Physical Exercise and Myokines: Relationships with Sarcopenia and Cardiovascular Complications. Int J Mol Sci. 2020 May 20;21(10)
11. Jochum SB, Kistner M, Wood EH, Hoscheit M, Nowak L, Poirier J, Eberhardt JM, Saclarides TJ, Hayden DM. Is sarcopenia a better predictor of complications than body mass index? Sarcopenia and surgical outcomes in patients with rectal cancer. Colorectal Dis. 2019 Dec;21(12):1372-1378.
12. Nakanishi R, Oki E, Sasaki S, Hirose K, Jogo T, Edahiro K, Korehisa S, Taniguchi D, Kudo K, Kurashige J, Sugiyama M, Nakashima Y, Ohgaki K, Saeki H, Maehara Y. Sarcopenia is an independent predictor of complications after colorectal cancer surgery. Surg Today. 2018 Feb;48(2):151-157.
13. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M, Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jul 01;48(4):601.
14. Boutin RD, Yao L, Canter RJ, Lenchik L. Sarcopenia: Current Concepts and Imaging Implications. AJR Am J Roentgenol. 2015 Sep;205(3):W255-66.
15. Albano D, Messina C, Vitale J, Sconfienza LM. Imaging of sarcopenia: old evidence and new insights. Eur Radiol. 2020 Apr;30(4):2199-2208.
16. Sanz-Requena R, Martínez-Arnau FM, Pablos-Monzó A, Flor-Rufino C, Barrachina-Igual J, García-Martí G, Martí-Bonmatí L, Pérez-Ros P. The Role of Imaging Biomarkers in the Assessment of Sarcopenia. Diagnostics (Basel, Switzerland). 2020 Jul 30;10(8)
17. Morrell GR, Ikizler TA, Chen X, Heilbrun ME, Wei G, Boucher R, Beddhu S. Psoas Muscle Cross-sectional Area as a Measure of Whole-body Lean Muscle Mass in Maintenance Hemodialysis Patients. J Ren Nutr. 2016 07;26(4):258-64.
18. Sergi G, Trevisan C, Veronese N, Lucato P, Manzato E. Imaging of sarcopenia. Eur J Radiol. 2016 Aug;85(8):1519-24.
19. Delancey JO, Kane Low L, Miller JM, Patel DA, Tumbarello JA. Graphic integration of causal factors of pelvic floor disorders: an integrated life span model. Am J Obstet Gynecol. 2008 Dec;199(6):610.e1-5.
20. Larsson L, Degens H, Li M, Salviati L, Lee YI, Thompson W, Kirkland JL, Sandri M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol Rev. 2019 01 01;99(1):427-511.
Figures