3831
The relationship between hepatic and pancreatic steatosis and cardiometabolic risk factors1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2MR Research, Beijing, China
Synopsis
This study assessed the correlation between hepatic and pancreatic steatosis and cardiometabolic risk factors. The results showed that hepatic and pancreatic FF were associated with specific risk factors, and the correlation coefficient varied by sex. This plays an important role in our further understanding about the association between ectopic fat deposition and cardiometabolic risk factors. Hepatic and pancreatic steatosis might have important implication for prevention cardiometabolic risk factors.
Synopsis
This study assessed the correlation between hepatic and pancreatic steatosis and cardiometabolic risk factors. The results showed that hepatic and pancreatic FF were associated with specific risk factors, and the correlation coefficient varied by sex. This plays an important role in our further understanding about the association between ectopic fat deposition and cardiometabolic risk factors. Hepatic and pancreatic steatosis might have important implication for prevention cardiometabolic risk factors.Introduction
Obesity is a heterogeneous condition that can be defined as abnormal or excessive fat accumulation, and it becoming one of the most significant public health problems and is a leading cause of preventable death. Previous studies have shown that abdominal fat distribution and ectopic fat deposition were associated with cardiovascular disease risk factors, including hypertension, type 2 diabetes mellitus (T2DM), dyslipidemia [1-3].Purpose
To evaluate the association between hepatic and pancreatic steatosis and a list of cardiometabolic risk factors.Methods
A total of 320 subjects (148 men and 172 women) were included in the study. In this study, the MRI scanner (GE Medical Systems, Inc., Waukesha, WI, USA) with an eight-channel phased-array body coil was used. IDEAL-IQ sequence parameters were as follows: TR/TE = 6.9 ms/3.0 ms, slice thickness of 10 mm, 200 KHZ bandwidth, FOV = 36 cm×36 cm, matrix = 256 ×160, flip angle = 3 °, NEX = 1, breath holding for less than 24 s. The images were processed using IDEAL Research software provided by the manufacturer to generate water-phase, fat-phase, in-phase, out-phase, along with R2* and FF maps. On the post-processing platform (Intellispace portal, ISP, Philips, Holland), the software algorithm defined the margins of the liver in three dimensions, and whole liver was semi-automatically traced on FF maps. If the margins needed tweaking, the operator made corrections; if margins were included within the contours of liver segmentation, the main portal vein, inferior vena cava, and the gallbladder were manually removed. Then liver was segmented, and the whole hepatic FF was automatically calculated (Fig 1A). This methodology was also used to measure pancreatic FF (Fig 1B). All data were analyzed using SPSS Ver.25.0 (SPSS Inc., Chicago, IL, USA). The intraclass correlation coefficient (ICC) was used to check the consistency of the two observers. To assess the associations between fat measurements, age and sex-adjusted correlation coefficients (r) among various MR-acquired fat depots were computed.Results
Patients’ clinical characteristics were shown in Table 1. Two-observer measurement consistency was great (ICC > 0.75) (Table 2). Hepatic and pancreatic fat fraction were associated with specific risk factors (P<0.05) (Table 3), and the correlation coefficient varied by sex (table 4).Conclusion
Hepatic and pancreatic fat fraction were associated with various cardiometabolic risk factors, and the correlation varied by sex and specific risk factors.Discussion
This study assessed the correlation between hepatic and pancreatic fat fraction and cardiometabolic risk factors. The results showed that hepatic and pancreatic fat fraction were associated with specific risk factors, and the correlation coefficient varied by sex. This plays an important role in our further understanding about the association between hepatic and pancreatic fat fraction and cardiometabolic risk factors. Hepatic and pancreatic steatosis might have important implication for prevention cardiometabolic risk factors.Acknowledgements
No acknowledgement found.References
1.Barik A, Shah RV, Spahillari A, et al. Hepatic steatosis is associated with cardiometabolic risk in a rural Indian population: A prospective cohort study. Int J Cardiol. 2016; 225:161-166.
2.Fabbrini E, Magkos F. Hepatic Steatosis as a Marker of Metabolic Dysfunction. Nutrients. 2015;7(6):4995-5019.
3. Wang CY, Ou HY, Chen MF, et al. Enigmatic ectopic fat: prevalence of nonalcoholic fatty pancreas disease and its associated factors in a Chinese population. J Am Heart Assoc. 2014;3(1): e000297.
Figures
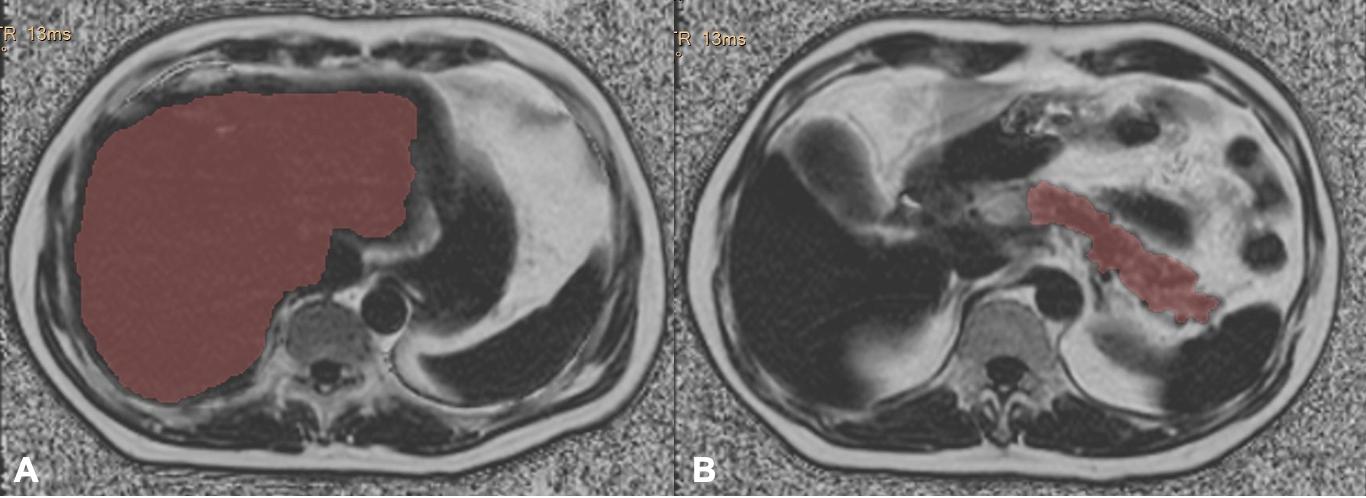
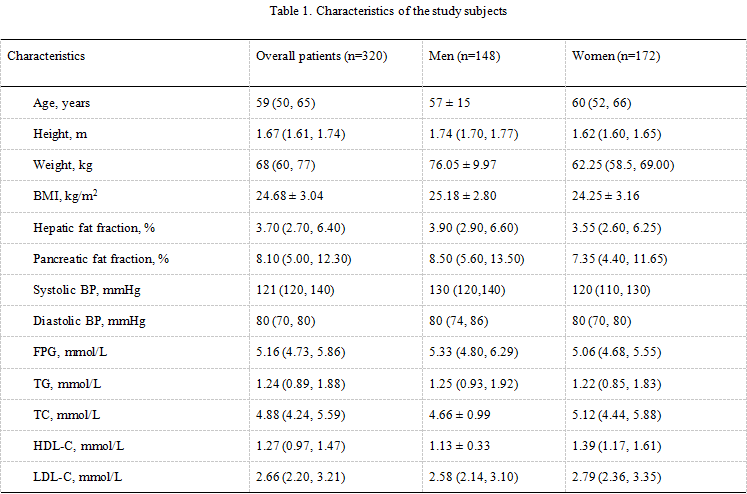
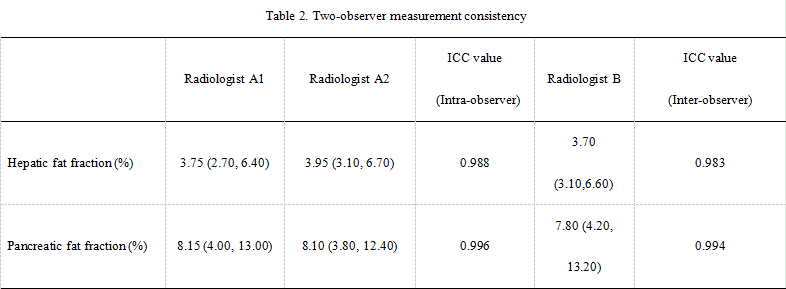
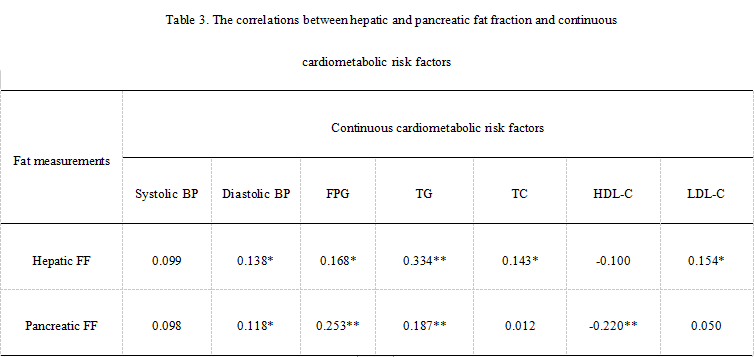
Table 3. The correlations between hepatic and pancreatic fat fraction and continuous cardiometabolic risk factors
*P<0.05, **P<0.001.
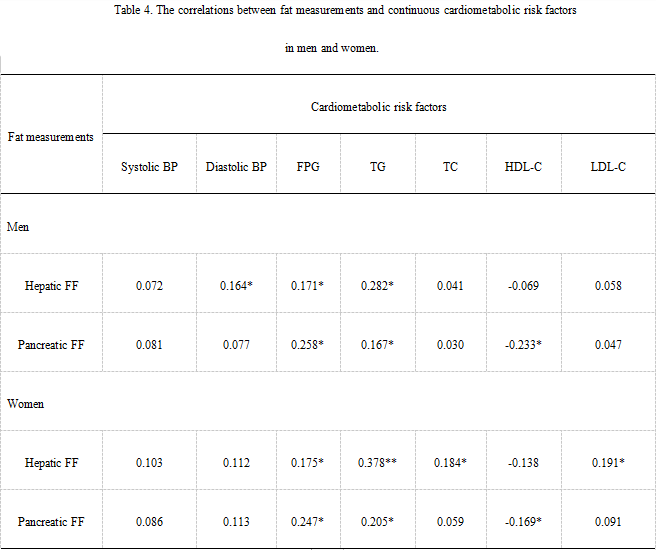
Table 4. The correlations between fat measurements and continuous cardiometabolic risk factors in men and women.
*P<0.05, **P<0.001.