3829
Value of Adopting Fast Brain MRI Techniques for Outpatient Brain MRI: Proof of Principle and Operational Impact During the COVID-19 Pandemic1Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 2Siemens Medical Solutions, Boston, MA, United States, 3Medically Engineered Solutions in Healthcare Incubator, Massachusetts General Hospital, Boston, MA, United States
Synopsis
We report our clinical experience of implementing fast MRI sequences into the most performed brain MRI protocols at a large academic center, which resulted in significant decrease of gradient times on both 1.5T and 3T scanners. The overall scan times were reduced by up to 40% for the longest examinations, with all included brain MRI protocols now being under 20 minutes. The potential benefits of reduced scan time include increased imaging volume throughput and improved patient access. During the ongoing COVID-19 pandemic, the decreased scan times also accommodated heightened infection control protocols to help protect both patients and healthcare workers.
Introduction
In an era of increasing medical imaging utilization and declining reimbursements, fast MRI techniques promise to decrease imaging times and improve access to MRI. Clinical validation studies have demonstrated the ability of highly accelerated MRI sequences to decrease acquisition time and motion artifact while preserving image quality.1-3 The operational benefits achieved using fast MRI techniques have been less explored. Here, we report our initial clinical experience in implementing fast MRI techniques across a variety of brain MRI protocols for outpatient imaging during the COVID-19 pandemic. We hypothesized that the aggregated time savings from performing multiple fast MRI sequences would result in significant reductions in scan time across a variety of brain MRI examinations.Methods
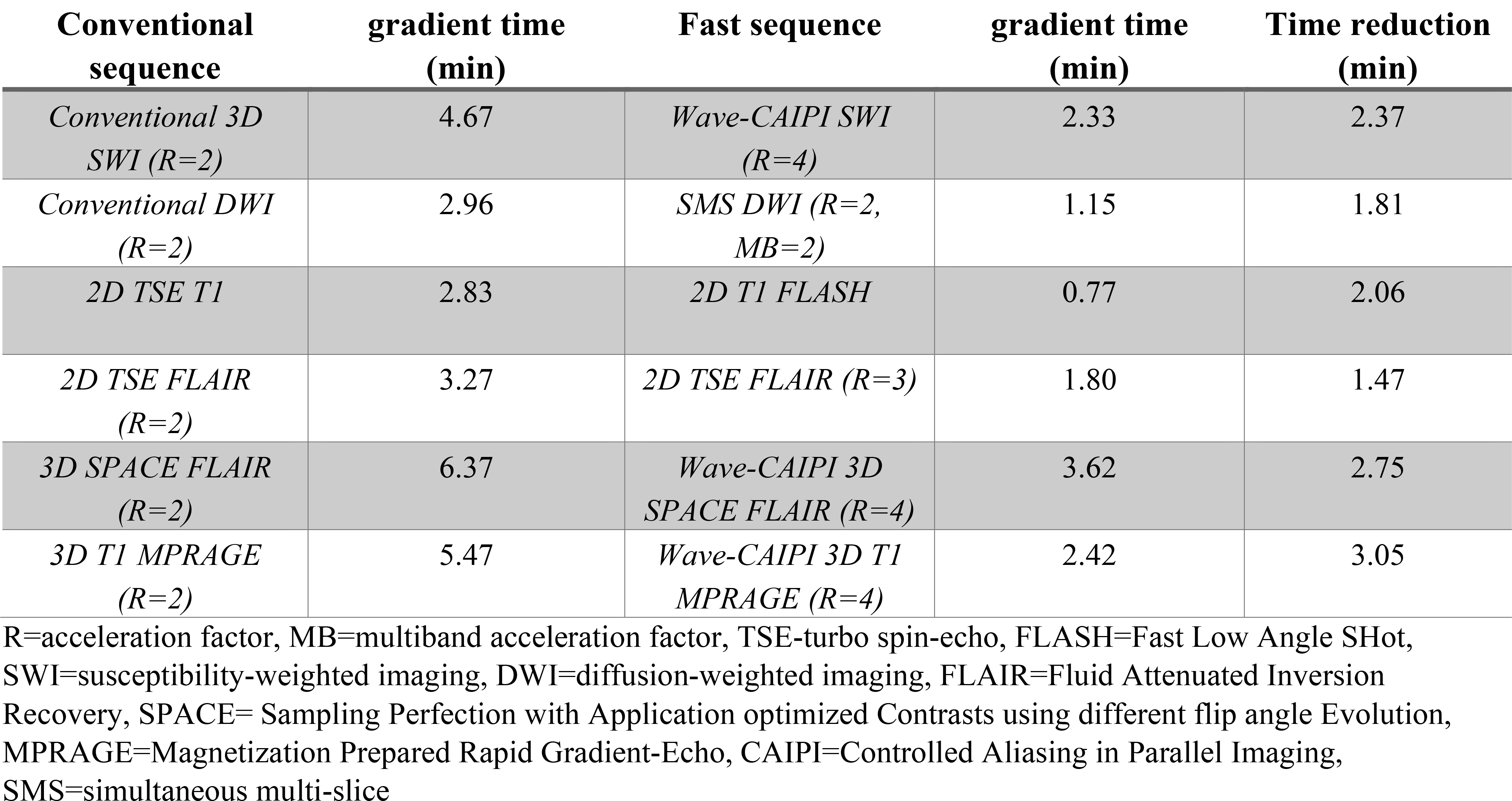
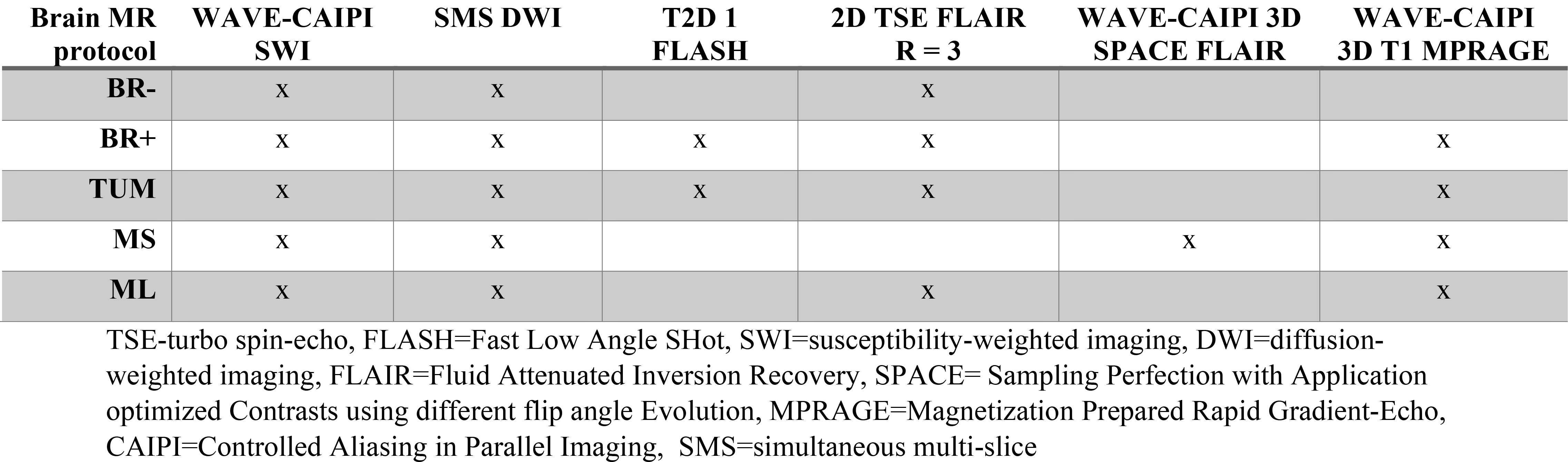
In the summer of 2020, our tertiary-care academic medical center implemented previously optimized fast MRI sequences1-3 into the clinical brain MRI protocols on three outpatient MRI scanners. This was done to help address a backlog of outpatient MRI studies and allow for increased time between scans for room sanitization and social distancing. Fast brain MRI sequences incorporating techniques such as parallel imaging,4 simultaneous multislice imaging (SMS),5 and Wave-CAIPI for highly accelerated 3D imaging6,7 (Figure 1) were implemented on two 3T scanners and one 1.5T scanner (MAGNETOM Vida, Prisma-Fit, and Avanto-Fit, respectively; Siemens Healthineers, Germany). Total gradient time, start time of the first sequence, and end time of the last sequence were extracted from the medical record on consecutive imaging examinations performed on these scanners during matched pre-implementation (8/1/2019-11/30/2019) and post-implementation periods (8/1/2020-11/30/2020). Gradient times were compared for the five most performed brain MRI protocols pre- and post-implementation: brain without contrast (BR-), brain with and without contrast (BR+), brain tumor (TUM), multiple sclerosis (MS), and memory loss (ML). The fast MRI sequences included in these protocols are listed in Figure 2. The expected gradient time reduction for each MR sequence was calculated by subtracting the gradient time of the fast sequences from those of the corresponding pre-implementation conventional MRI sequences; this was achieved by manual collection of gradient times for 5 representative studies for each sequence. Multiple variables including patient characteristics, scanner type, field strength, and other non-optimized MR sequences affected the gradient times and contributed to gradient time variability. The gradient times for each protocol were not normally distributed and were compared using the nonparametric Wilcoxon rank sum test.Results
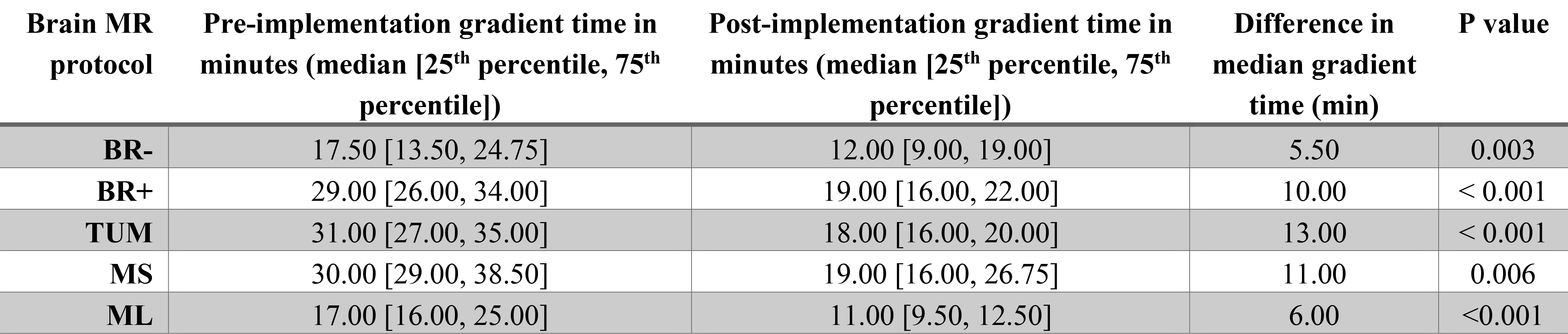
The overall study volumes for the BR-, BR+, TUM, MS, and ML protocols were 134, 374, 31, 160, and 35, respectively, during the pre-implementation period and 111, 525, 51, 107, and 29, respectively, during the post-implementation period. The expected gradient time reductions from implementing the fast sequences in the BR-, BR+, TUM, MS and ML protocols were 6.48 min, 11.25 min, 12.05 min, 8.13 min, and 6.76 min, respectively (Figure 1). The median gradient time was significantly reduced in all protocols during the post- versus pre-implementation period (Figure 3). The median gradient time was reduced by 5.5 min (19.78%) for BR-, 10.0 min (29.30%) for BR+, 13.0 min (39.55%) for TUM, 11.0 min (38.40%) for MS, and 6.0 min (38.87%) for ML. Using the weighted proportion of each different brain MRI protocol, the overall average reduction in gradient time was 33.54% (9.52 min).Discussion
Fast MRI sequences have been previously evaluated in clinical settings with a primary focus on diagnostic and image quality compared to their conventional counterparts.1-3,8-10 The operational benefits of fast MRI sequences, including their synergistic time savings, have not been studied as fully. Our results indicate that the implementation of fast MRI sequences into the most performed brain MRI protocols significantly decreased the gradient times on both 1.5T and 3T scanners, offering up to 40% reduction in overall scan time for the longest examinations and bringing the scan times for all included brain MRI protocols down to <20 minutes each. During the COVID-19 pandemic, the time saved in each protocol accommodated heightened infection control procedures adopted by our department to reduce the spread of the virus, without requiring longer booking slots. In the near future, the substantial time saved per examination and increased operational efficiency may enable shortening examination slot times – a key strategy for improving MRI efficiency and increasing annual throughput while mitigating downstream costs.11 Our findings provide compelling evidence that fast MRI acquisitions can minimize protocol length, increase imaging throughput, and improve patient access to valuable MRI resources.Conclusion
The implementation of fast brain MRI sequences significantly reduced the gradient times for the most performed brain MRI protocols. The projected benefits to the clinical workflow and patient care include increased imaging volume throughput, improved patient access, and improved patient and healthcare worker safety during the COVID-19 pandemic.Acknowledgements
No acknowledgement found.References
1. Prakkamakul, S. et al. Ultrafast Brain MRI: Clinical Deployment and Comparison to Conventional Brain MRI at 3T. J Neuroimaging 26, 503-510, doi:10.1111/jon.12365 (2016).
2. Conklin, J. et al. Validation of Highly Accelerated Wave-CAIPI SWI Compared with Conventional SWI and T2*-Weighted Gradient Recalled-Echo for Routine Clinical Brain MRI at 3T. AJNR. American journal of neuroradiology 40, 2073-2080, doi:10.3174/ajnr.A6295 (2019).
3. Longo, M. G. F. et al. Evaluation of Ultrafast Wave-CAIPI MPRAGE for Visual Grading and Automated Measurement of Brain Tissue Volume. AJNR. American journal of neuroradiology 41, 1388-1396, doi:10.3174/ajnr.A6703 (2020).
4. Griswold, M. A. et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 47, 1202-1210, doi:10.1002/mrm.10171 (2002).
5. Setsompop, K. et al. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 67, 1210-1224, doi:10.1002/mrm.23097 (2012).
6. Bilgic, B. et al. Wave-CAIPI for highly accelerated 3D imaging. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 73, 2152-2162, doi:10.1002/mrm.25347 (2015).
7. Polak, D. et al. Highly-accelerated volumetric brain examination using optimized wave-CAIPI encoding. Journal of magnetic resonance imaging : JMRI 50, 961-974, doi:10.1002/jmri.26678 (2019).
8. Ahamed, S. H., Lee, K. J. & Tang, P. H. Role of a modified ultrafast MRI brain protocol in clinical paediatric neuroimaging. Clin Radiol 75, 914-920, doi:10.1016/j.crad.2020.07.009 (2020).
9. Ha, J. Y. et al. One-Minute Ultrafast Brain MRI With Full Basic Sequences: Can It Be a Promising Way Forward for Pediatric Neuroimaging? AJR Am J Roentgenol 215, 198-205, doi:10.2214/AJR.19.22378 (2020).
10. JM, U. K.-I. et al. Utility of an ultrafast magnetic resonance imaging protocol in recent and semi-recent strokes. J Neurol Neurosurg Psychiatry 76, 1002-1005, doi:10.1136/jnnp.2004.046201 (2005).
11. Boland, G. W. & Duszak, R., Jr. Modality Access: Strategies for Optimizing Throughput. J Am Coll Radiol 12, 1073-1075, doi:10.1016/j.jacr.2015.06.012 (2015).
Figures