3750
Adding an absolute chest position regressor to RETROICOR for spinal cord fMRI during atypical breathing patterns
Neha A Reddy1,2, Andrew D Vigotsky1,3, Rachael C Stickland2, and Molly G Bright1,2
1Department of Biomedical Engineering, Northwestern University, Evanston, IL, United States, 2Department of Physical Therapy and Human Movement Sciences, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 3Department of Statistics, Northwestern University, Evanston, IL, United States
1Department of Biomedical Engineering, Northwestern University, Evanston, IL, United States, 2Department of Physical Therapy and Human Movement Sciences, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 3Department of Statistics, Northwestern University, Evanston, IL, United States
Synopsis
RETROICOR (Retrospective Image Correction) is a commonly used technique for physiological noise correction, but it may not be optimal in its standard implementation for use in studies of the human spinal cord involving atypical breathing patterns. We test the inclusion of an absolute chest position regressor derived from respiratory belt data, in addition to standard RETROICOR regressors, in modeling fMRI scans of the cervical spinal cord with and without breath-hold challenges. The chest position regressor may be a simple approach towards explaining additional noise variance in spinal cord fMRI data during breath-hold tasks.
Introduction
Physiological noise caused by respiratory motion and blood vessel pulsation is especially important to account for in fMRI studies involving regions such as the spinal cord and brainstem1,2. RETROICOR (Retrospective Image Correction) is a technique commonly used for physiological noise correction that uses pulse and respiratory data3. RETROICOR assumes regular breathing patterns and calculates respiratory regressors using the distribution of participant chest positions during a scan. However, fMRI experiments that involve atypical breathing patterns, such as breath-hold or potentially motor task studies4, violate this assumption and have more varied distributions of chest position across the scan. The proper approach for mitigating respiration-related artifacts in these studies is unclear.Here, we test two methods of physiological noise correction with fMRI data collected in the spinal cord during a breath-hold challenge and a resting-state scan. We compare two models: (1) using RETROICOR (2) using RETROICOR and an additional regressor that describes absolute chest position across the scan.
Methods
Data Collection: Four resting-state and breath-hold task fMRI scans of the cervical spinal cord were collected from three healthy subjects (3M, 30±3.5 years). Data were acquired on a Siemens 3T Prisma MRI system with a 64-channel head coil and spine matrix coil. All scans were collected using an EPI sequence with ZOOMit selective excitation: TR/TE=2000/30ms, FA=90°, in-plane resolution=1x1mm2, 25 transverse slices, slice thickness=3mm, slice gap=3mm. During the breath-hold task, subjects were visually cued to perform 9-10 breath-hold cycles: 24s paced breathing, end-expiratory 18s hold, 2s exhalation, 8s recovery. During resting-state scanning, subjects viewed a fixation cross. Chest position was measured with a BIOPAC respiration belt and pulse via a transducer on the index finger or thumb, both sampled at a frequency of 1000 Hz (PowerLab, ADInstruments).Data Analysis: In MATLAB, pulse and respiration peaks were extracted and used to create 12 low-order Fourier series RETROICOR regressors (4 cardiac, 4 respiratory, and 4 interaction) as described in Glover et al. (2000)3. The respiration belt trace was also used to create a slice-wise chest position regressor for each volume. For each breath-hold and resting-state dataset, two general linear models were created: raw data modeled with RETROICOR and raw data modeled with RETROICOR and chest position. Polynomial terms (up to third order) were also included in each model. A circular mask containing the spinal cord and surrounding CSF was applied to the results and a voxel-wise partial R2 value was calculated to describe the additional variance explained by the chest position regressor compared to RETROICOR alone.
Results
Fig1 shows the distribution of chest positions for each subject across the breath-hold and resting-state scans. RETROICOR uses these distributions to calculate the phase of respiratory Fourier series terms. Variations in distribution can be seen across subjects and between breath-hold and resting-state scans. Subj1 has the most similar resting-state and breath-hold distributions.Fig2 and Fig3 show maps of the partial R2 values for three slices of the spinal cord for the breath-hold and resting-state datasets, respectively. Subj1’s breath-hold and resting-state maps are the most similar, while the others display greater partial R2 values in the breath-hold condition, primarily located around the edges of the spinal cord.
Fig4 shows the distribution of partial R2 values for each subject and scan. Subj2 and Subj3 have an increase in mean and median partial R2 in the breath-hold condition compared to rest, while Subj1 has a slight increase in the rest condition. Subj2 and Subj3 also have more extreme variation in partial R2 values of breath-hold scans compared to rest scans and Subj1’s breath-hold scan.
Discussion and Conclusion
Our initial findings indicate absolute chest position may explain additional variance in raw spinal cord fMRI data collected during a breath-hold task compared to RETROICOR alone. However, there was considerable variation in this effect across subjects. This variation may be related to differences in breathing patterns across subjects (Fig1); subjects with a greater difference in breathing pattern in their breath-hold scan versus resting-state showed a greater overall partial R2 value of the added chest position regressor in the modeled breath-hold data. Because RETROICOR regressors depend on the chest position distribution created by the “regular” breathing pattern seen in resting-state scans, a greater deviation from this expected distribution reflects a greater deviation from RETROICOR assumptions and perhaps greater utility of an alternative regressor.Although we used a chest position regressor with RETROICOR to model the field effects of breathing motion, this regressor may also reflect bulk motion of the torso and cord. In fMRI processing pipelines, RETROICOR correction can be performed prior to a motion correction algorithm. The resultant preprocessed fMRI data are used in a subsequent general linear model that may include motion regressors in addition to other pertinent signal models (e.g., a task vector). It will be important to examine the interaction of our slice-wise chest position regressor with subsequent processing techniques and confirm its best implementation in this pipeline. Further understanding of the relationship between the raw respiratory belt data and different fMRI confounds is needed before making a recommendation for spinal cord fMRI preprocessing more generally. However, we have demonstrated that this denoising approach may be beneficial in spinal cord fMRI during atypical breathing patterns.
Acknowledgements
This research is supported by the Craig H. Neilsen Foundation (595499). N.A.R. was supported by National Institutes of Health award T32GM008152. This material is based upon work supported by the National Science Foundation Graduate Research Fellowship under Grant No. DGE-1324585.References
- Brooks JC, Beckmann CF, Miller KL, et al. Physiological noise modelling for spinal functional magnetic resonance imaging studies. Neuroimage. 2008;39(2):680-692.
- Brooks JC, Faull OK, Pattinson KT, et al. Physiological noise in brainstem FMRI. Front. Hum. Neuro. 2013;7:623.
- Glover GH, Tie-Qiang L, and Ress D. Image‐based method for retrospective correction of physiological motion effects in fMRI: RETROICOR. Mag. Reson. Med. 2000;44(1):162-167.
- Amazeen PG, Amazeen EL, and Beek PJ. Coupling of breathing and movement during manual wheelchair propulsion. J. Exp. Psych: Hum. Perc. Perf. 2001;27(5):1243-1259.
Figures
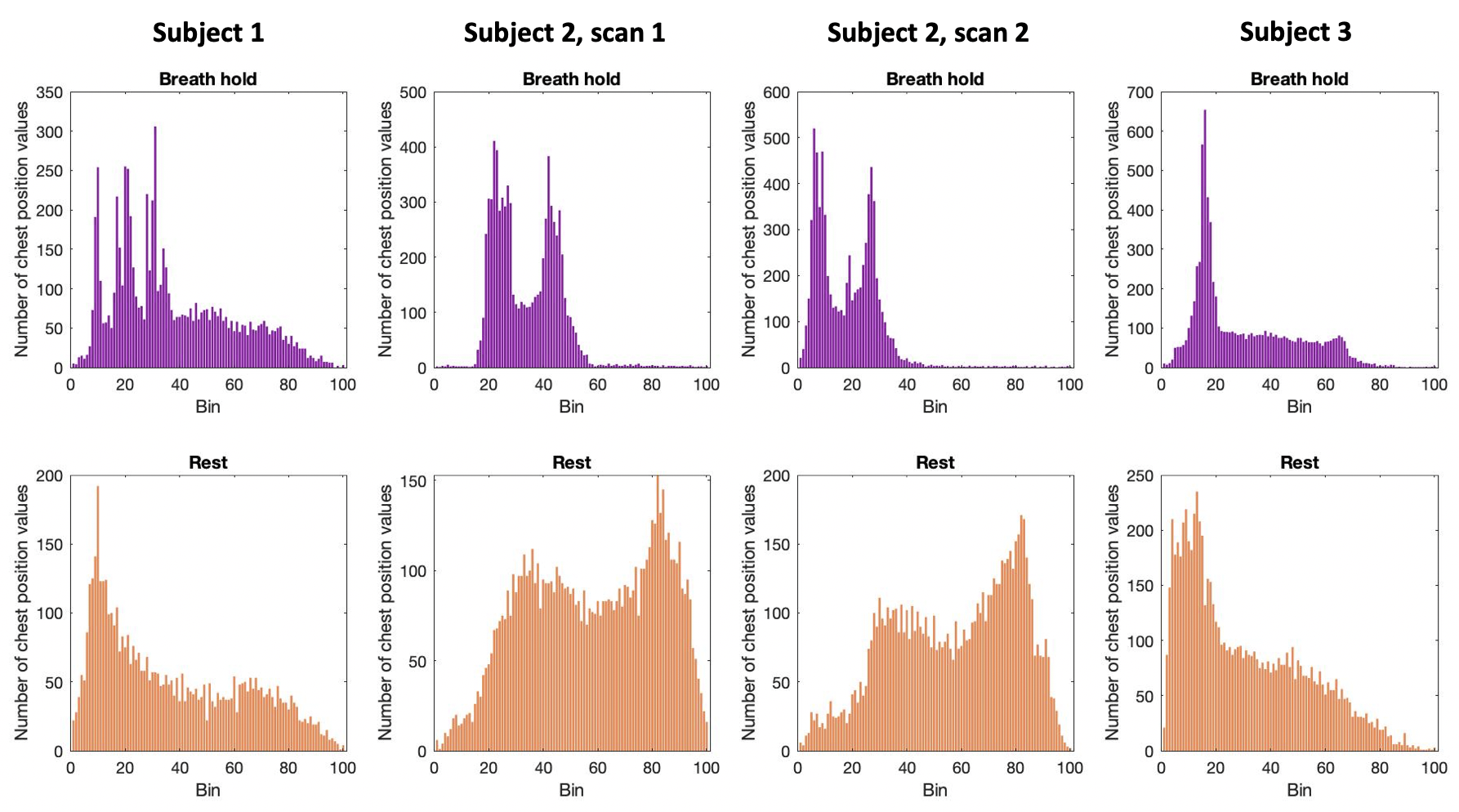
Figure 1. Respiratory cycle histogram created from respiration belt trace of chest position, plotted for each scan. Histograms created from chest position data during breath-hold task scans (top row) and resting-state scans (bottom row). In breath-hold scans, extra peaks at lower bins are due to prolonged low chest position during end-expiratory breath holds. Long tails at higher bins are due to large inhalations during recovery breaths post-breath hold.
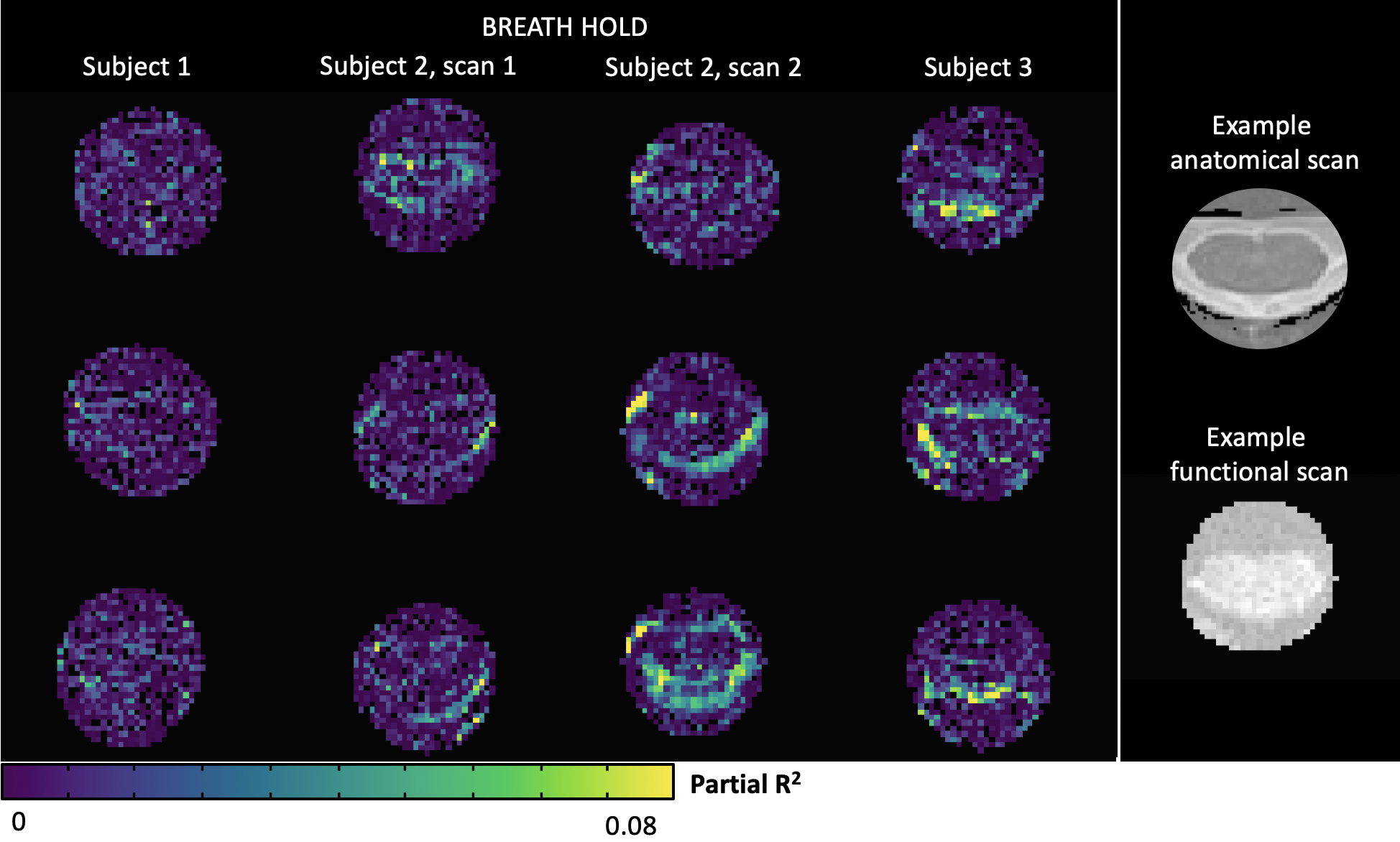
Figure 2. Maps of partial R2 values from adding a chest position regressor compared to RETROICOR alone during breath-hold scans. Three cervical spinal cord transverse slices are shown at approximately the same levels for each subject. Example anatomical and functional scans of the spinal cord are shown in the rightmost column for context.
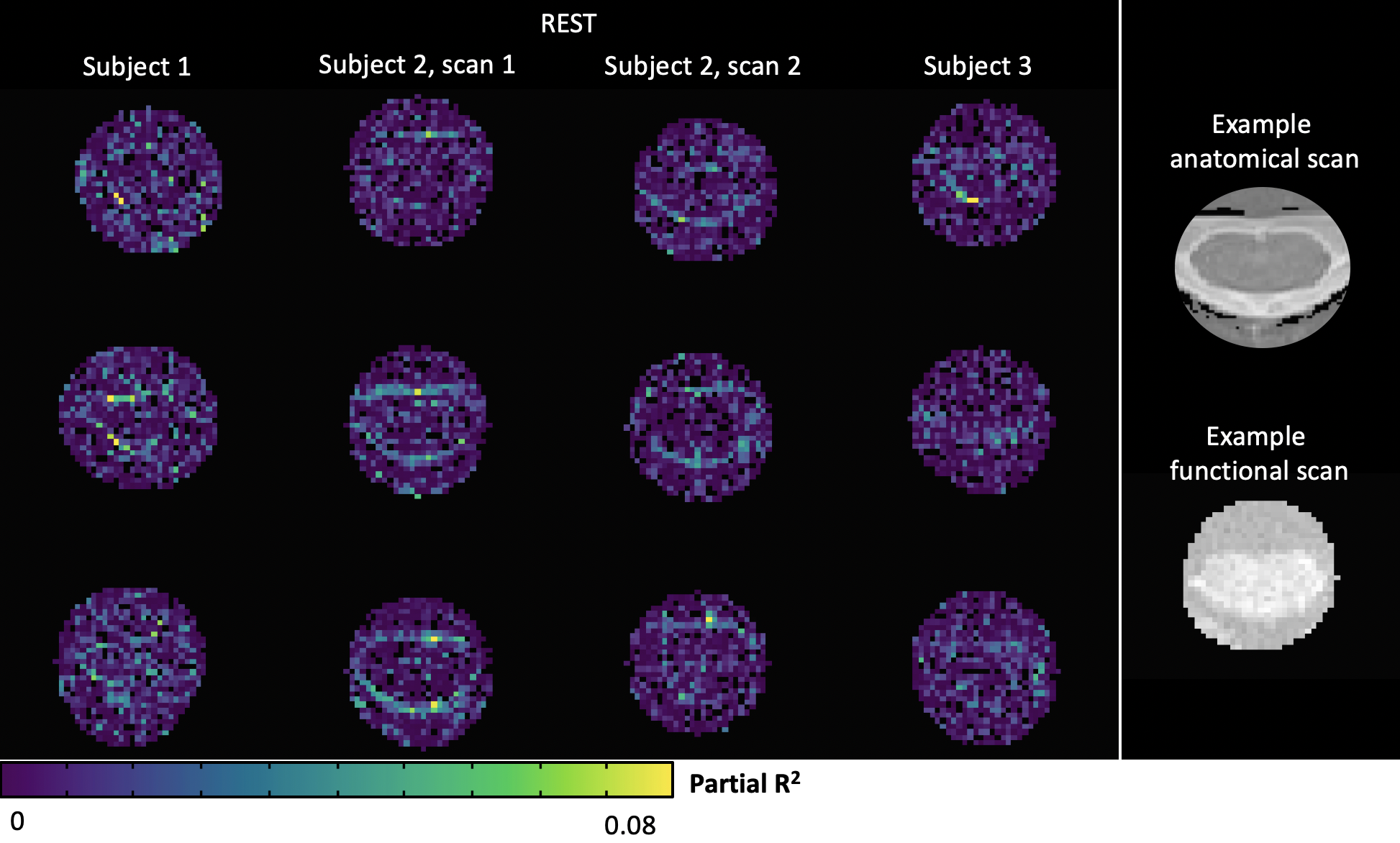
Figure 3. Maps of partial R2 values from adding a chest position regressor compared to RETROICOR alone during resting-state scans. Three cervical spinal cord transverse slices are shown at approximately the same levels for each subject. Example anatomical and functional scans of the spinal cord are shown in the rightmost column for context.
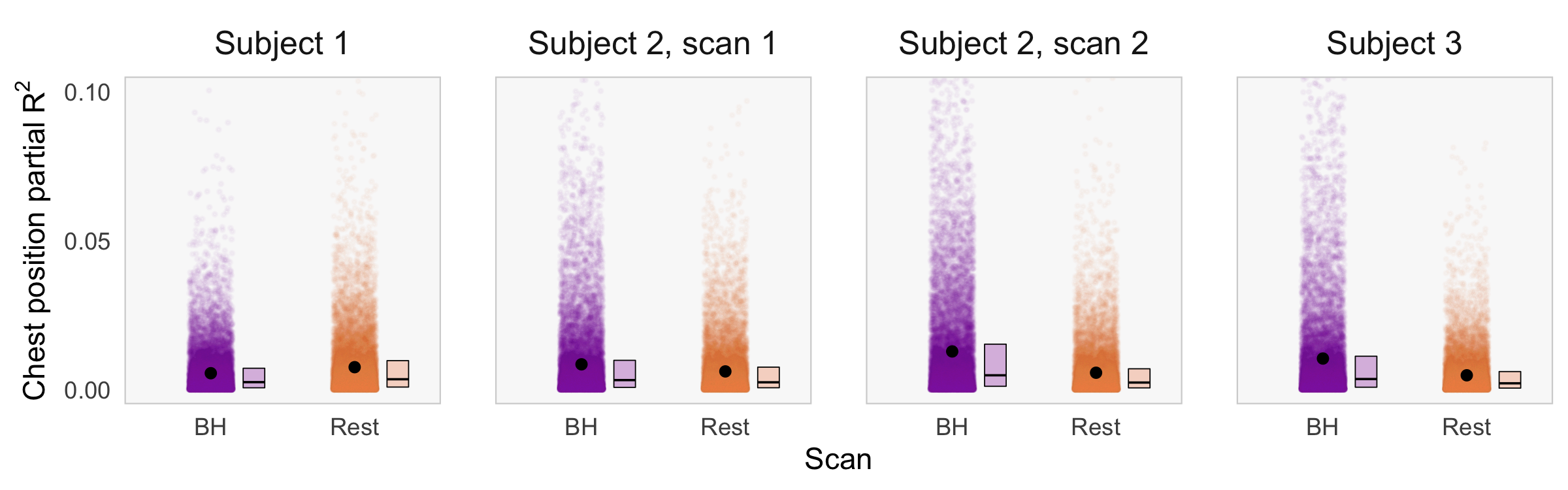
Figure 4. Distribution of partial R2 values for added chest position regressor in each breath-hold (BH) and rest scan. Mean adjusted R2 for RETROICOR-only models ranged from 0.18 to 0.25 and for chest position models from 0.18 to 0.26. Each partial R2 value represents the percent of unexplained variance in the RETROICOR-only model that is explained by addition of a chest position regressor. Each black dot represents the mean partial R2 value for the scan. Spatial distribution of this variation is seen in Fig2 and Fig3.