3662
Methodological considerations on segmenting MRI data of rhabdomyosarcoma1Image Science Institute, UMC Utrecht, Utrecht, Netherlands, 2Princess Máxima Center for Pediatric Oncology, Utrecht, Netherlands, 3Department of Radiology, Academic Medical Centre Amsterdam, Amsterdam, Netherlands
Synopsis
Rhabdomyosarcoma is a rare form of cancer that is particularly prevalent in children. There is a pressing need for new imaging biomarkers for monitoring treatment response, such diffusion. No standards currently exist to annotate rhabdomyosarcoma on MRI and measure the diffusion.
This work analyses segmentation strategies in recent literature on saromas and compares them on a toy example. It shows that there is a large inconsistency in the application of segmentation strategies and that the different methods for segmenting the tumor can yield high variation in measured diffusion.
Introduction
Rhabdomyosarcoma is a rare form of cancer that is particularly prevalent in children. Treatment monitoring of rhabdomyosarcoma is currently done by looking at changes in the size of the tumor before and after treatment measured by either the longest diameter of the tumor or the tumor volume 1. Recent studies have shown that such assessments have only moderate interobserver agreement 2 and furthermore can be inaccurate predictors of long term survivability 3,4. Without radiological measures, there is a pressing need for new imaging biomarkers for monitoring treatment response.One promising candidate is the apparent diffusion coefficient (ADC) of the tumor, as a decrease in ADC can indicate a lowered cellularity within the tumor and corresponding effective treatment 5. No standards currently exist to annotate rhabdomyosarcoma on MRI and derive ADC values, limiting the comparability of studies into the effect of ADC as a biomarker 6. This work examines the current practices of segmenting sarcomas as described in literature and tests the extent of variability caused in the measurement of ADC by different segmentation strategies.
Literature survey
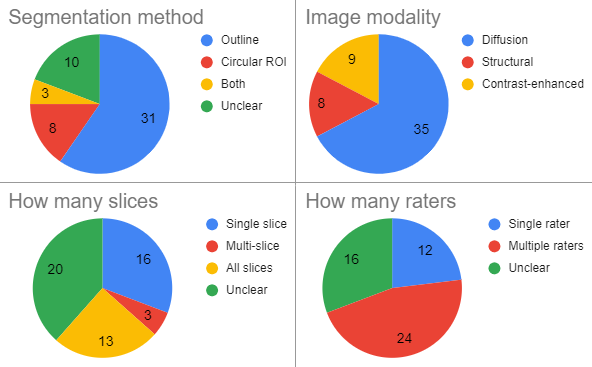
We surveyed 52 recent papers which performed manual segmentation of sarcomas. For each paper, the following aspects of the segmentation strategy were tallied:- Segmentation method:
- outline
- circular region of interest (ROI)
- both
- unclear
- How many raters:
- single rater
- multiple raters
- unclear
- Segmentation volume:
- single slice
- multi-slice
- all slices
- unclear
- Image modality
- diffusion weighted image (DWI)
- structural image (T1/T2)
- contrast-enhanced image
- Segmentation target:
- only active tumor
- whole tumor
- no necrosis
- no cyst
- no hemorrhage
- unclear
Comparison of strategies
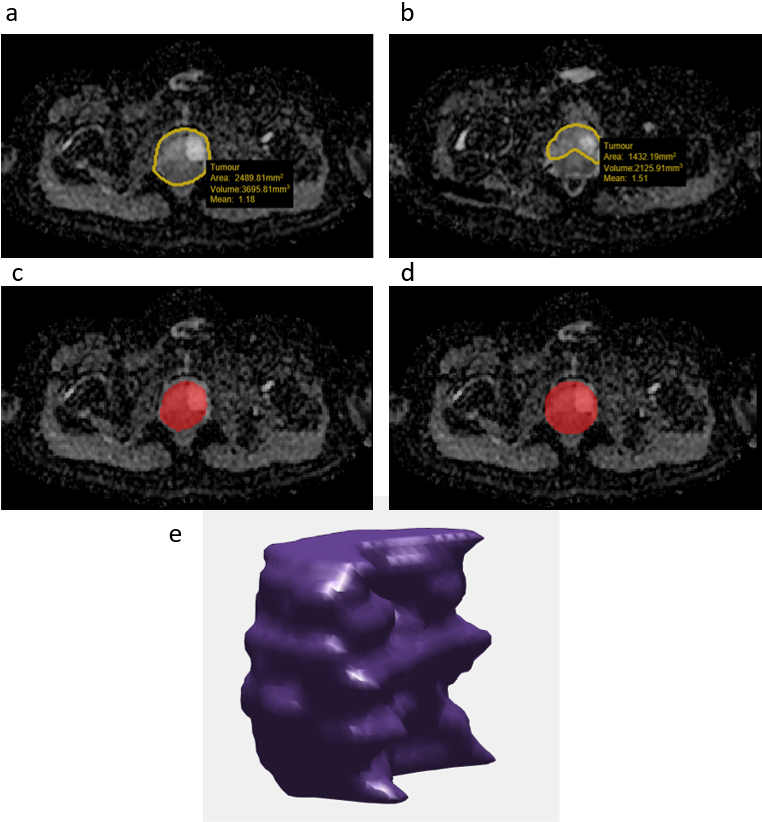
In order to illustrate effects of different segmentation strategies, four methods were applied to an ADC map of pediatric rhabdomyosarcoma. These methods are:- 2D outline of the whole tumor performed by two experienced radiologists on what they perceived as the largest slice ('outline')
- 2D outline of the whole tumor minus the edge, achieved by eroding the 'outline' method segmentations with a 5x5 kernel ('eroded')
- circular ROI placed by a trained researcher on the same slice as the first outline segmentation in such a way to cover as much area without exceeding past the tumor boundaries ('circular')
- outline of the whole tumor in 3D delineated by a trained researcher on each slice ('3D').
Results
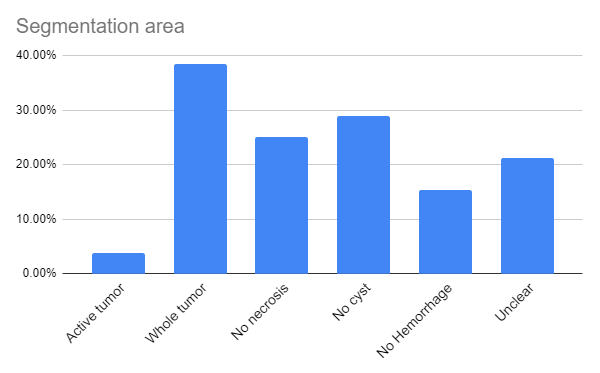
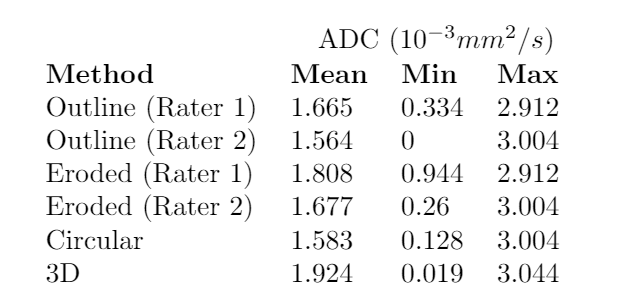
Figure 1 shows the tallies of the segmentation methods, how many raters, segmentation volumes, and image modalities that were used in the surveyed papers. Many aspects of the segmentation strategy were found to be reported with insufficient detail to allow for reproduction of the steps. Furthermore, 9 papers which had initially been selected for the survey reported no details about the segmentation method and had to be left out. Figure 2 shows what area the surveyed papers selected for segmentation. A high variability can be seen between the various strategies in choosing whether or not to exclude certain areas of the tumor.Figure 3 shows the segmentations that were obtained via the different segmentation strategies. There is clear variation between the areas that the radiologists delineated, as well as a difference in the slice which they deemed to have the largest tumor area.The ADC is greatly impacted by the segmentation details. As table 1 demonstrates, both the minimum and the mean ADC vary largely when going from a 2D outline to a 3D outline or when excluding the edge of the tumor. The mean ADC varies by up to 23%.
Discussion
Figure 1 shows that there is large variation in each aspect of the segmentation strategy of the papers that were surveyed. The results also demonstrate a lack of reporting of crucial details which can impair reproduction.It is furthermore shown that the area of segmentation is often restricted to avoid disturbance from the effects of necrosis, hemorrhaging, or the forming of cystic compartments. As these are different studies, no consensus of what areas to include and exclude can be found from this sample. It is important to remark, however, that many of the papers do not support the influence of excluding these regions with any evidence.
Due to its rarity, research on rhabdomyosarcoma often has to be a multi-center approach. The heterogeneity due to image acquisition being different in each center paired with the inherent variability in the data from the many possible tumor locations can make research very cumbersome. Removing a source of variability by defining a robust standard for segmentation can therefore be an important step in streamlining future work.
A standard for segmentation can be obtained by extending the work shown here and demonstrating the extent to which the chosen strategies impact the measured values when using segmentation to determine functional imaging characteristics, such as mean ADC of a tumor.
Conclusion
Our survey demonstrates that not much consensus currently exists on the segmentation of sarcomas. Additionally, recent literature does not always contain key information on how segmentations are obtained. Very little is still known about the effects that segmentation strategies have on measurement outcome. We have shown that variation of strategy can lead to a change in ADC of up to 23%. Further research is therefore needed to create a more robust standard.Acknowledgements
No acknowledgement found.References
1 Ferrari, A., Miceli, R., Meazza, C., Casanova, M., Favini, F., Morosi, C., ... & Terenziani, M. (2010). Comparison of the prognostic value of assessing tumor diameter versus tumor volume at diagnosis or in response to initial chemotherapy in rhabdomyosarcoma. Journal of clinical oncology, 28(8), 1322-1328.
2 Schoot, R. A., McHugh, K., van Rijn, R. R., Kremer, L. C., Chisholm, J. C., Caron, H. N., & Merks, J. H. (2013). Response assessment in pediatric rhabdomyosarcoma: can response evaluation criteria in solid tumors replace three-dimensional volume assessments?. Radiology, 269(3), 870-878.
3 Rosenberg, A. R., Anderson, J. R., Lyden, E., Rodeberg, D. A., Wolden, S. L., Kao, S. C., ... & Hawkins, D. S. (2014). Early response as assessed by anatomic imaging does not predict failure-free survival among patients with Group III rhabdomyosarcoma: A report from the Children’s Oncology Group. European Journal of Cancer, 50(4), 816-823.
4 Vaarwerk, B., van der Lee, J. H., Breunis, W. B., Orbach, D., Chisholm, J. C., Cozic, N., ... & Glosli, H. (2018). Prognostic relevance of early radiologic response to induction chemotherapy in pediatric rhabdomyosarcoma: a report from the International Society of Pediatric Oncology Malignant Mesenchymal Tumor 95 study. Cancer, 124(5), 1016-1024.
5 Robba, T., Chianca, V., Albano, D., Clementi, V., Piana, R., Linari, A., ... & Borrè, A. (2017). Diffusion-weighted imaging for the cellularity assessment and matrix characterization of soft tissue tumour. La radiologia medica, 122(11), 871-879.
6 Norman, G., Fayter, D., Lewis-Light, K., McHugh, K., Levine, D., & Phillips, B. (2015). Mind the gap: extent of use of diffusion-weighted MRI in children with rhabdomyosarcoma. Pediatric radiology, 45(5), 778-781.
Figures