3661
Assessment the Preponderant Diagnostic Performances of Oligometastatic Prostate Cancer Using Diffusion Kurtosis Imaging1The First Affiliated Hospital of Dalian Medical University, Dalian, China
Synopsis
It remains a challenge to diagnose the oligometastatic prostate cancer (PCa) due to the ambiguous definition of oligometastatic PCa. Previous studies had shown that diffusion kurtosis imaging (DKI) is a non-gaussian diffusion weighted imaging (DWI) method that yields more accurate results on the microstructural complexity of prostate cancer tissue structure. This study indicated that performances of DKI cannot differentiate between oligometastatic and widely metastatic PCa, however it has the potential to assess tumor load and aggressiveness in metastatic PCa.
Introduction
The term “Oligometastases” was first proposed in 1995 by Hellman and Weichselbaum [1]. Oligomeric prostate cancer (PCa) indicates the intermediate state between local and advanced metastatic disease. In previous studies, the definition of oligometastatic PCa depended on the number of bone metastatic lesions (usually 3 to 5) [2]. Although the definition of oligometastatic PCa is not clear, studies have suggested that treatment of the primary tumor might provide a survival benefit to oligometastatic PCa patients [3-4]. Diffusion kurtosis imaging (DKI) is a non-gaussian diffusion weighted imaging (DWI) method that yields more accurate results on the microstructural complexity of prostate cancer tissue structure [5].Purpose
To evaluate the diagnostic performances of DKI in assessing oligometastatic PCa.Methods
All PCa patients from Jan. 2018 to Dec. 2019, who underwent 3.0T MR scanning with DKI sequence were enrolled in this study. Patients with 1) treatment by chemotherapy, radiation therapy, endocrine therapy; 2) low image quality were excluded. Finally, 54 PCa patients were included in this study. Age ranged from 60 to 87 years, mean age 74±7.4 years. A 3.0T MR scanner (Signa HDxt, General Electric) and an 8-channel phased-array surface coil were used. DKI was performed using an axial single shot spin echo echo-planar imaging (SE-EPI) sequence (repetition time 2500 ms, echo time 80 ms, field of view 35×35cm cm2, number of excitations 2, slice thickness 7.0 mm, slice spacing 1.0 mm, b–values 1000,2000s/mm2, apply a diffusion gradient in 30 orthogonal directions, scan duration 2 minutes 58 seconds). Functool software was used to calculate statistics of the regions of interest (ROIs) of mean kurtosis (MK), axial kurtosis (Ka), radial kurtosis (Kr), fractional anisotropy of kurtosis (FAk), mean diffusivity (MD), axial diffusivity (Da), radial diffusivity (Dr) and fractional anisotropy (FA) (Figure 1). The region of interest (ROI) was placed on the largest slice of the tumor, and contained the whole tumor as much as possible. According to the number of bone metastatic lesions, the PCa patients were individed to three group: localized lesions group (no bone metastatic lesion), oligometastatic group (the number of bone metastatic lesions less than but equal to three) and widely metastatic group ( the number of bone metastatic lesions more than three). The intraclass correlation coefficient (ICC) was used to test the consistency of the two observers. The differences among groups were analyzed by Kruskal-Wallis test or One-way ANOVA test. Spearman’s bivariate correlation analysis was performed to assess the correlation between DKI parameters and prostate specific antigen (PSA).Results
Inter-observer repeatability agreement was excellent in the orbital mass for all the DKI parameters (ICC = 99.4%, 99.5% ,99.4%,99.5%,98%,99.3%,99.6%and 98.7% for FA, MD , Da , Dr , FAk , MK , Ka and Kr, respectively). There were significant differences in MD , Dr , MK and Ka among the groups(P=0.002,P=0.001 , P=0.012 and P=0.006 ,Table 1). And MD and Dr values of the localized lesions group were significantly higher than those of the widely metastatic group (1.05 (IQR, 0.87-1.2) vs 0.787 (IQR, 0.605-0.823), P=0.001 and 0.938 (IQR, 0.777-1.04) vs 0.647 (IQR, 0.534-0.73), P=0.001). MK and Ka value of the localized lesions group was significantly lower than that of the widely metastatic group (0.942±0.184 vs 1.200±0.324, P=0.012 and 1.051±0.259 vs 1.408±0.385, P=0.006). There were no significantly different between oligometastatic and widely metastatic group (P<0.05) . Correlations between DKI parameters and PSA are shown in Table2. MD ,Da and Dr showed a significant negative correlation with PSA. MK , Kr and Ka showed a significant positive correlation with PSA. No statistically significant correlation was shown between PSA and FAk or FA.Discussion
The MK value represents the average value of diffusion kurtosis in all spatial directions, and the Ka value represents the average kurtosis value in the long axis direction of diffusion tensor, both of which are proportional to the complexity of the tissue.MD reflects the overall diffusion level and diffusion resistance of molecules , and Da represents the diffusion coefficient of water molecules in the main diffusion direction [6], which are proportional to the degree of motion of water molecules . Probably because metastasis is closely related to primary tumor load and invasion. The tumor with widely metastatic, the proliferation of cancer cells was active, the number of stromal cells increased, and the structure of microenvironment was disordered, which is why MK and Ka value of widely metastasis group increased. However, the decrease of extracellular space and the increase of interstitial fluid pressure caused the dispersion movement of water molecules to be limited, which is why MD and Da of widely metastasis group was decreased. Meanwhile, MD ,Da, Dr, MK , Kr and Ka have significant correlation with PSA, indicating that they are closely related to tumor load.Conclusion
The performances of DKI cannot differentiate between diagnostic oligometastatic and widely metastatic PCa, but it has the potential to assess tumor load and aggressiveness in metastatic PCa.Acknowledgements
No acknowledgement found.References
[1] Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol. 1995 Jan;13(1):8-10. doi: 10.1200/JCO.1995.13.1.8. PMID: 7799047.
[2] Rii J, Sakamoto S, Yamada Y, Takeshita N, Yamamoto S, Sazuka T, Imamura Y, Nakamura K, Komiya A, Komaru A, Fukasawa S, Nakatsu H, Akakura K, Ichikawa T. Prognostic factors influencing overall survival in de novo oligometastatic prostate cancer patients. Prostate. 2020 Aug;80(11):850-858. doi: 10.1002/pros.24016. Epub 2020 Jun 5. PMID: 32501559.
[3] Rusthoven CG, Carlson JA, Waxweiler TV, Raben D, Dewitt PE, Crawford ED, Maroni PD, Kavanagh BD. The impact of definitive local therapy for lymph node-positive prostate cancer: a population-based study. Int J Radiat Oncol Biol Phys. 2014 Apr 1;88(5):1064-73. doi: 10.1016/j.ijrobp.2014.01.008. PMID: 24661660.
[4] Lin CC, Gray PJ, Jemal A, Efstathiou JA. Androgen deprivation with or without radiation therapy for clinically node-positive prostate cancer. J Natl Cancer Inst. 2015 May 9;107(7):djv119. doi: 10.1093/jnci/djv119. PMID: 25957435.
[5] Yin J, Sun H, Wang Z, Ni H, Shen W, Sun PZ. Diffusion Kurtosis Imaging of Acute Infarction: Comparison with Routine Diffusion and Follow-up MR Imaging. Radiology. 2018 May;287(2):651-657. doi: 10.1148/radiol.2017170553. Epub 2018 Mar 20. PMID: 29558293; PMCID: PMC5929367.
[6] Hectors SJ, Semaan S, Song C, Lewis S, Haines GK, Tewari A, Rastinehad AR, Taouli B. Advanced Diffusion-weighted Imaging Modeling for Prostate Cancer Characterization: Correlation with Quantitative Histopathologic Tumor Tissue Composition-A Hypothesis-generating Study. Radiology. 2018 Mar;286(3):918-928. doi: 10.1148/radiol.2017170904. Epub 2017 Nov 8. PMID: 29117481.
Figures
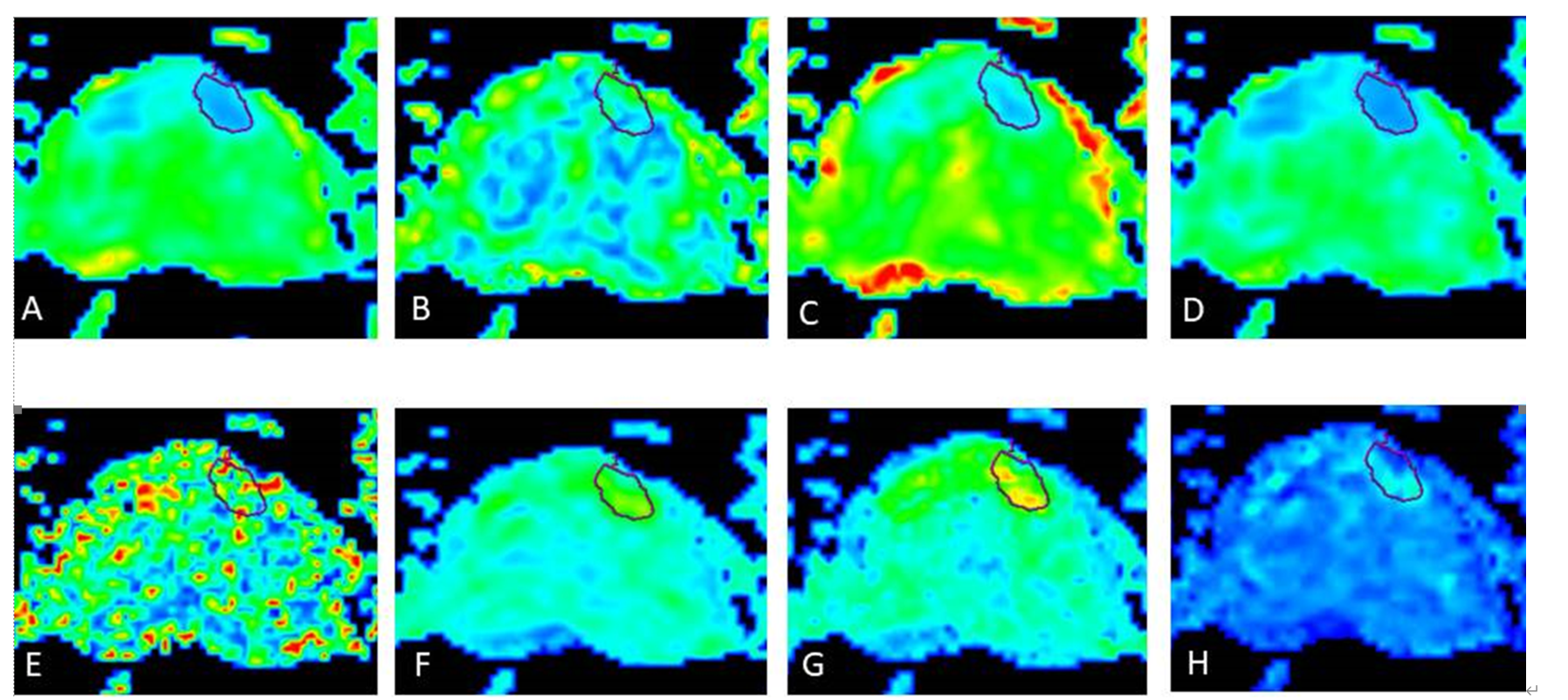
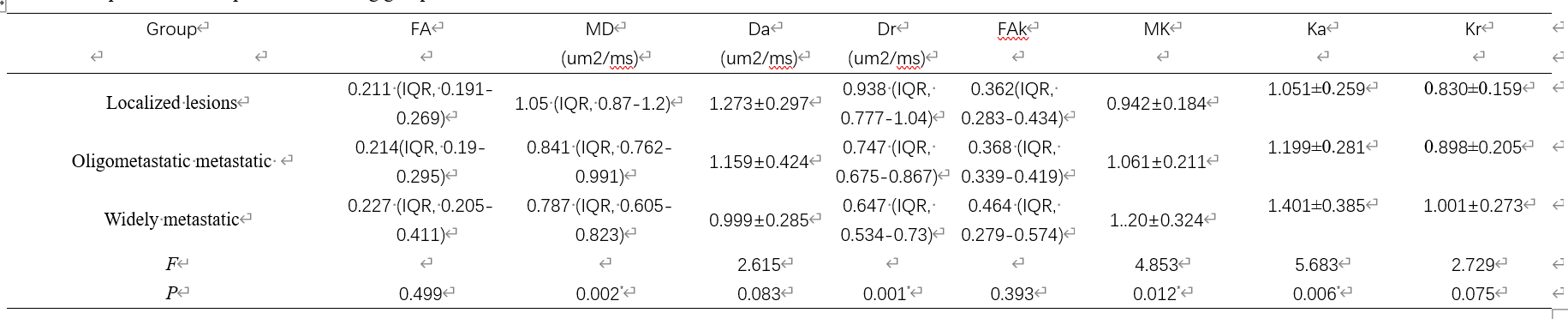
Table 1 Comparison of DKI parameters among groups
* P value is statistically significant. Da ,axial diffusivity , Dr ,radial diffusivity , FA, fractional anisotropy , FAk ,fractional anisotropy of kurtosis , Ka ,axial kurtosis , Kr, radial kurtosis , MD, mean diffusivity , MK, mean kurtosis

Table 2 Results of correlation analysis of DKI parameters and PSA
* P value is statistically significant.