3476
Application of 3D-FFE Based on Compressed Sensing for Lumbosacral Plexus Imaging: A Preliminary Study1Department of Medical Imaging, The Third Affiliated Hospital of Southern Medical University, Guangzhou, China, 2China International Center, Philips Healthcare, Guangzhou, China
Synopsis
The anatomy of lumbosacral plexus (LSP) is complex, patients with trauma, neoplasms, or infection may experience motor weakness, sensory loss, and/or debilitating pain. Accurate and fast MRN scanning is an invaluable tool for evaluation of LSP diseases. In this study, the feasibility and performance of compressed sensing (CS) in scanning LSP was investigated and compared with conventional 3D-FFE with principles of the selective excitation technique. The results show that 3D-FFE with CS could reduce scan time obviously, influence image quality mildly, and meet clinical diagnosis.
Purpose and Introduction
The MRN examination of the lumbosacral plexus (LSP) could clearly show the lesion location and morphology compared with the electrophysiological and physical examination1. However, patients with LSP diseases usually have lumbosacral neuralgia and cannot stay still for a long time, which results in motion artifacts and affects image quality. Relatively long MRN scanning time limits its clinical application. With the advent of compressed sensing (CS) technology, shortening the MR scan time is feasible2. The purpose of this study was to evaluate the feasibility and performance of 3D-FFE (Three-Dimensional Fast Field Echo) with principles of the selective excitation technique (Proset) MR imaging with compressed sensing for lumbosacral plexus imaging.Methods
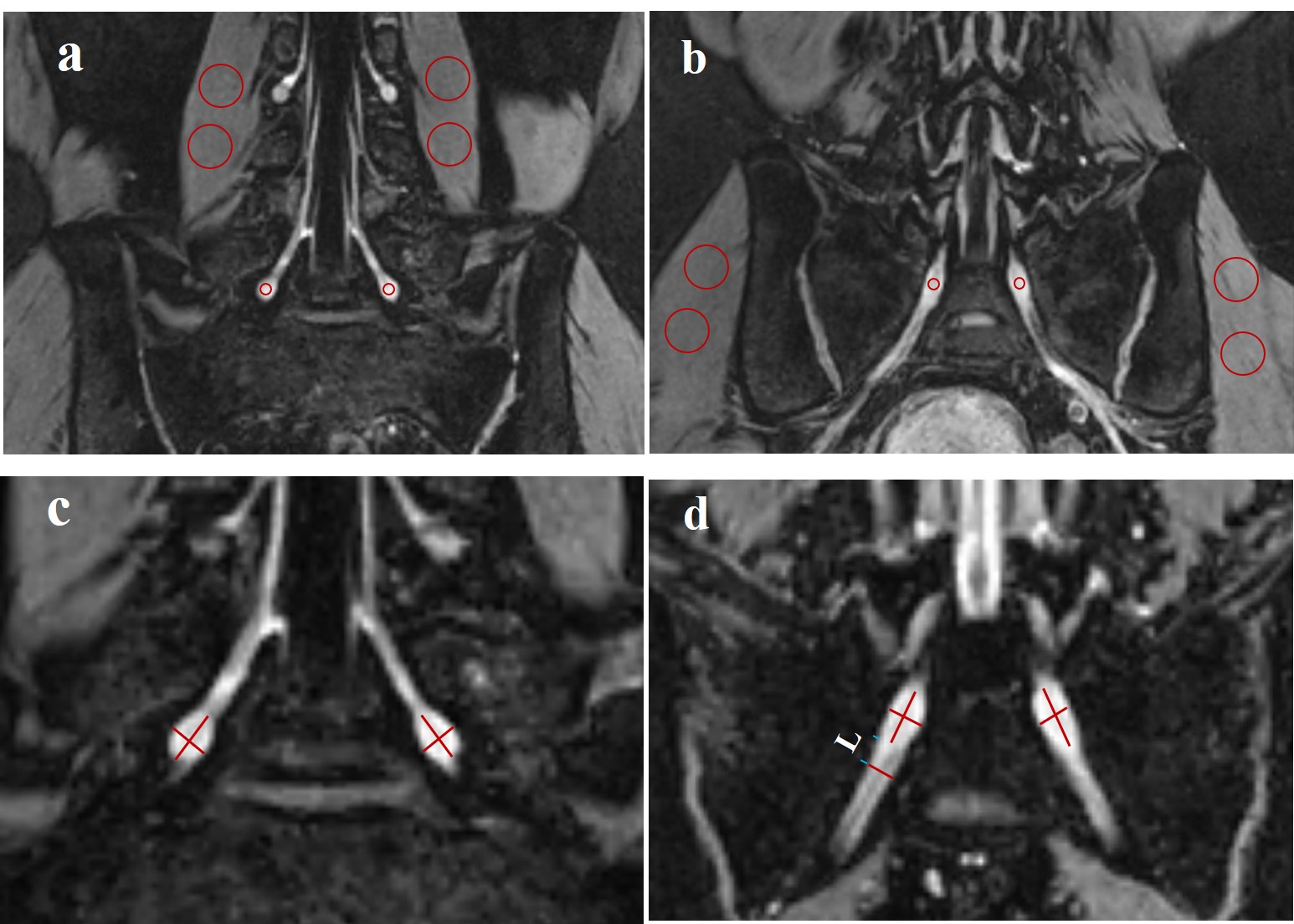
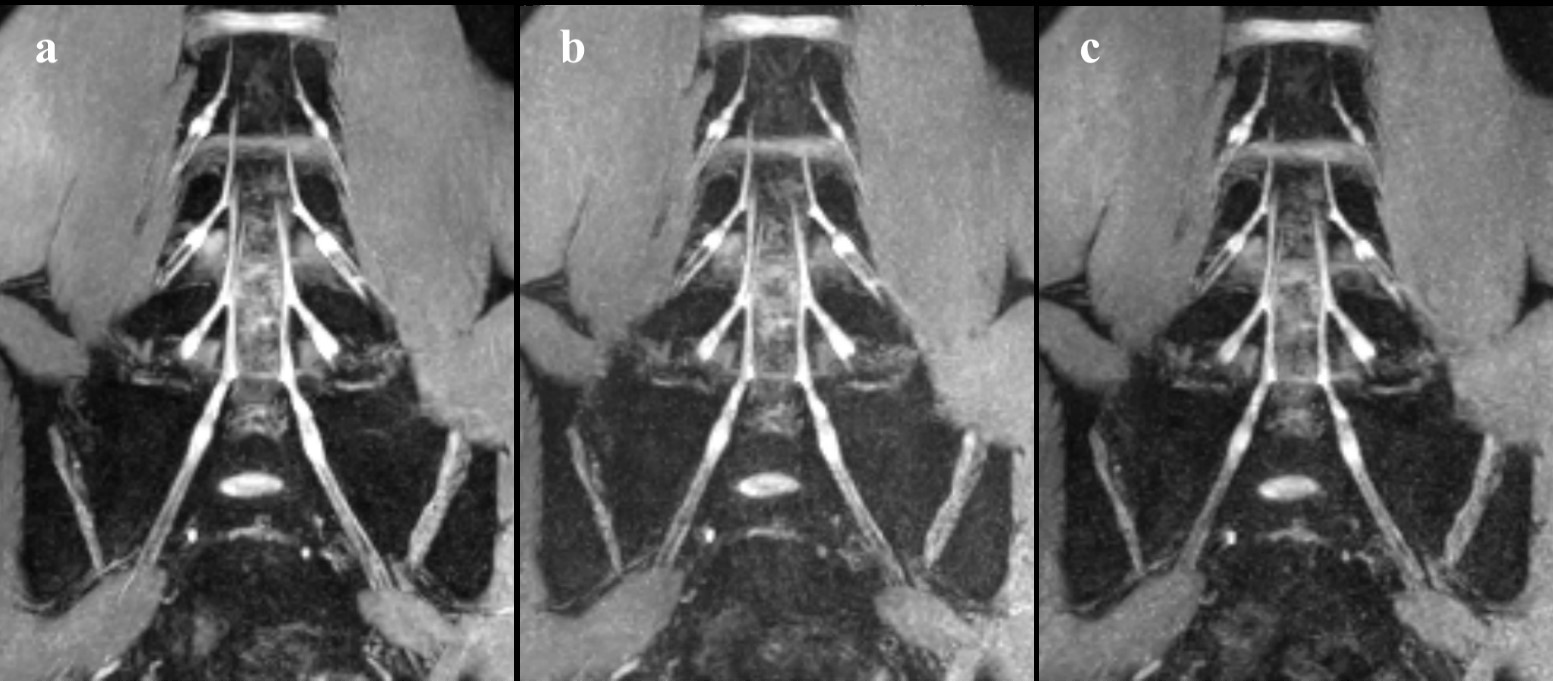
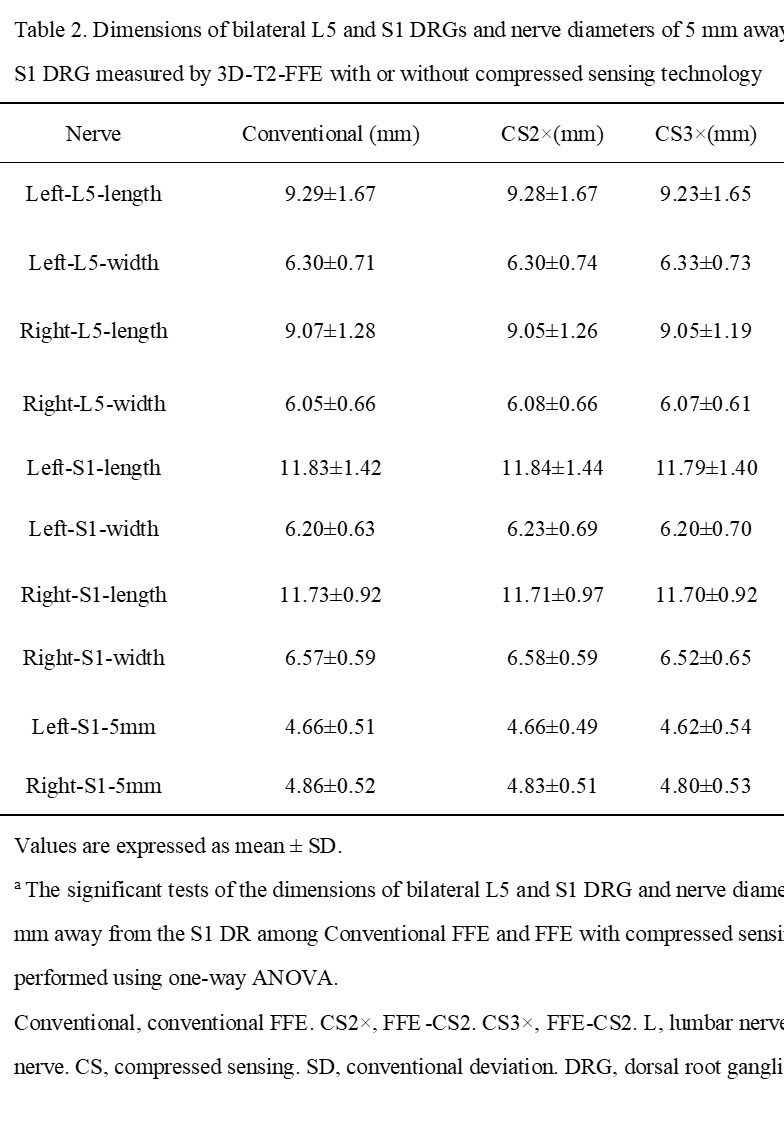
Twenty-four volunteers without lower back pain (26 ± 3.19 y old; 12men, 12women) underwent three types of 3D-FFE with Proset scans: one conventional FFE (number of signals averaged, NSA=2) and two CS 3D-FFE with acceleration factor=2, 3, and NSA=2, 3, respectively. All scans were acquired with otherwise equivalent imaging parameters on a 3.0T scanner (Ingenia, Philips Healthcare, Best, Netherlands). Subjective image quality was evaluated using a four-grade scoring system by two medical radiologists. A score greater than 2 indicates that the image could meet the clinical diagnosis. Signal intensity and morphological measurement were analyzed at the dorsal root ganglia (DRGs) of bilateral 5th lumbar and 1st sacrum. Regional image quality was evaluated using signal-to-noise ratios (SNRs) and contrast-to-noise ratios (CNRs).Results
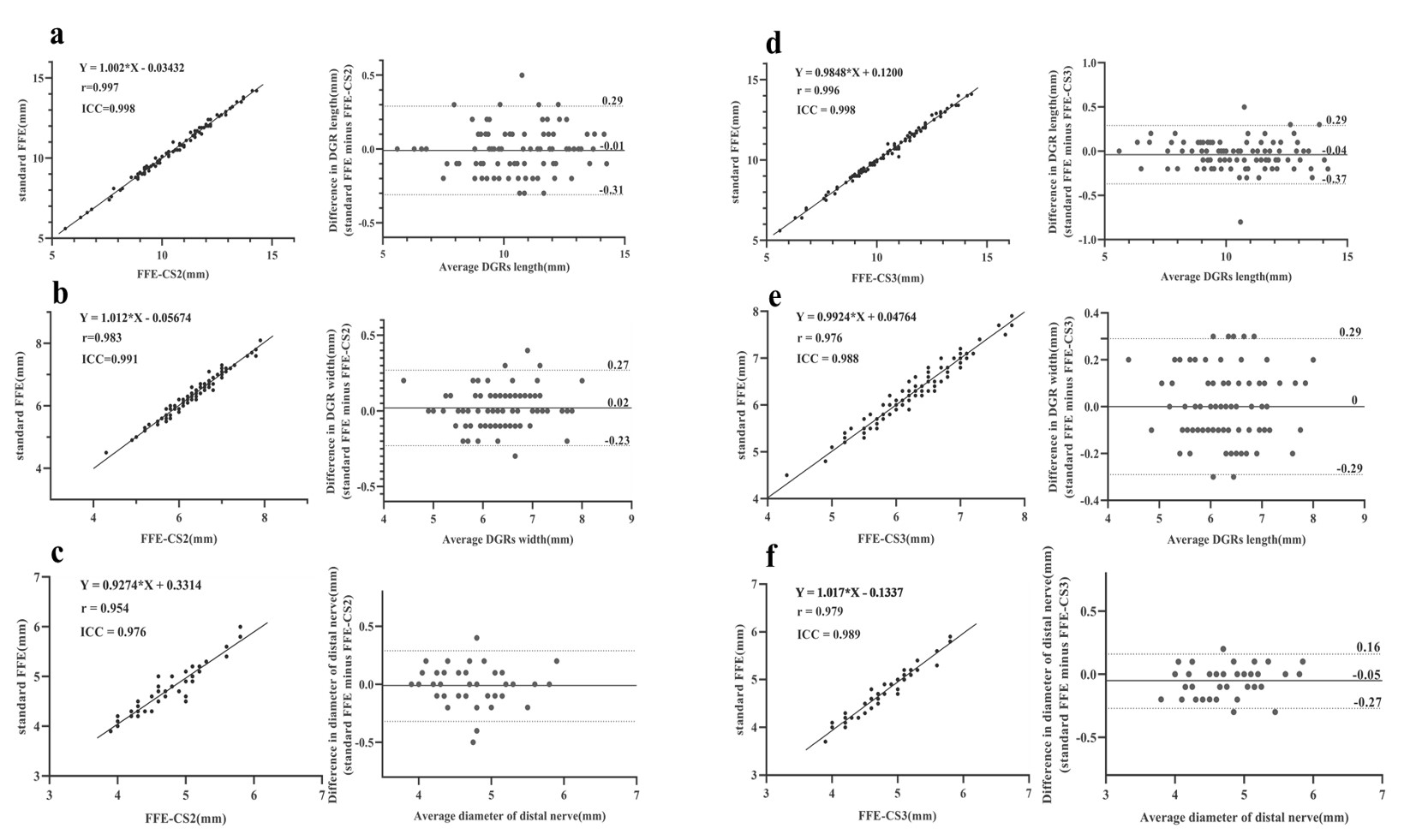
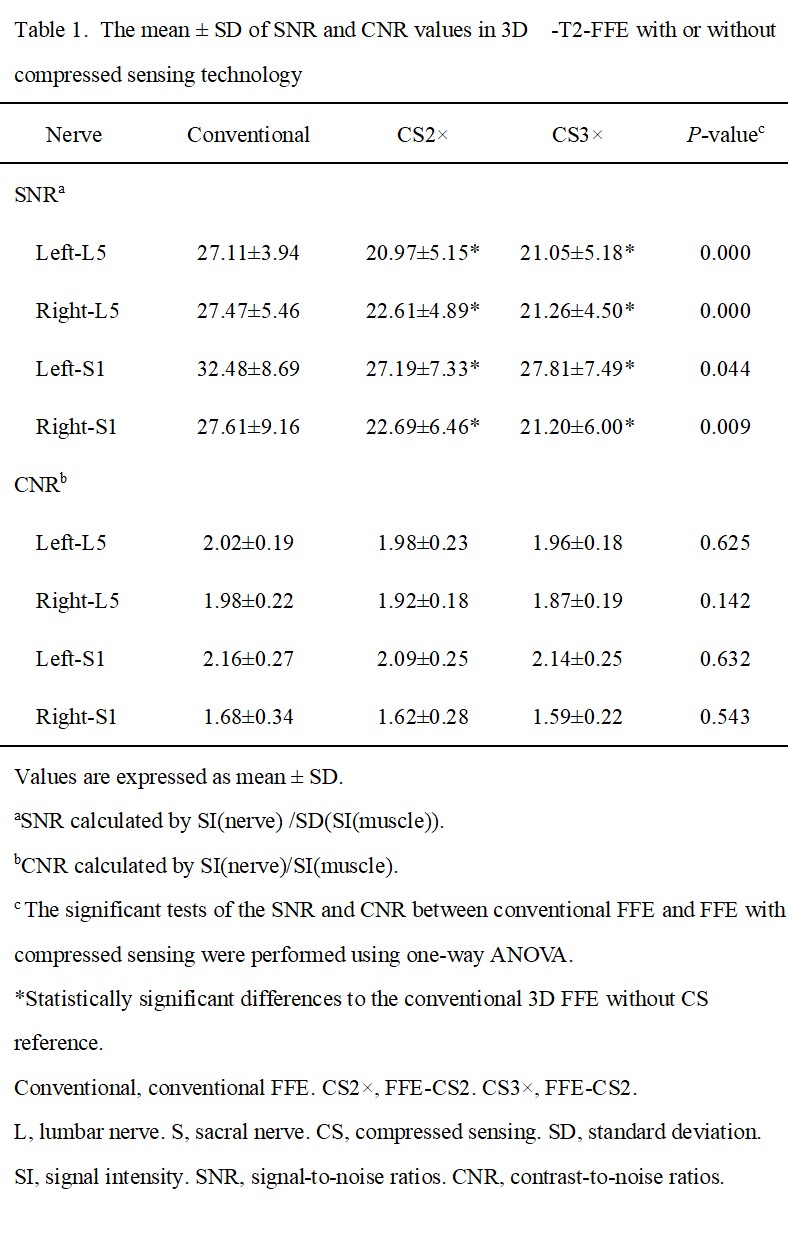
Scan times for the conventional FFE, FFE-CS2 and FFE-CS3 were 3:31 min, 2:01 min, and 2:00 min, respectively. Compared with conventional FFE, the scanning time of 3D CS-FFE sequence was reduced by 93-94 seconds, or about 43.5-43.9%. The two radiologists showed substantial consistency in their subjective ratings of images quality (all, κ˃0.6). The nerve discrimination and overall imaging quality scores of the three groups were 2.83±0.38, 2.75±0.44 and 2.62±0.49, respectively, and there was no significant difference among the three groups(P=0.257). Besides, radiologists subjectively assess the image quality of all three scan sequences were above 2 points. The conventional FFE sequence showed the highest bilateral L5 and S1 DRGs SNR than both two CS 3D-FFE sequences with different accelerating factors (all, P<0.05). CNR(DRGs/muscle) and morphological measurements showed no significant difference among conventional FFE and two FFE sequences with CS protocol.Conclusion
Compressed sensing technology can greatly improve scanning speed at the small expense of a small SNR with unchanged CNR, morphological measurements and subjective images evaluation score on lumbosacral plexus MR imaging. Also, we found that the increase of CS accelerating factor and NSA at the same time had no significant effect on the image quality of FFE imaging in our study.Acknowledgements
Corresponding authors: Xiaodong Zhang
Funding: The National Natural Science Foundation of China (81801653), Science and Technology Planning Project of Guangdong Province (2017B090912006) .
References
1. Neufeld EA, Shen PY, Nidecker AE, Runner G, Bateni C, Tse G et al. MR Imaging of the Lumbosacral Plexus: A Review of Techniques and Pathologies. Journal of neuroimaging: official journal of the American Society of Neuroimaging 2015; 25(5): 691-703.
2. Iuga AI, Abdullayev N, Weiss K, Haneder S, Bruggemann-Bratke L, Maintz D et al. Accelerated MRI of the knee. Quality and efficiency of compressed sensing. European journal of radiology 2020; 132: 109273.
Figures