3467
Quantitative Multimodal Magnetic Resonance Imaging for the Evaluation of Dysthyroid Optic Neuropathy1Radiology, The first affiliated hospital of Sun Yet-sen University, Guangzhou, China, 2MR Sicentific Marketing, Siemens Healthineers, Shanghai, China
Synopsis
Dysthyroid optic neuropathy (DON) is one of the most severe types of Graves orbitopathy (GO) and requires urgent treatment to prevent blindness. However, DON is frequently difficult to diagnose clinically in its early stages because of confounding signs and symptoms of congestive orbitopathy. In our study, we evaluate orbital condition of DON patients by using quantitative multimodal MRI, which include anatomical and functional indicators. We found that mMI (at 21 mm) combined with the mean T2 value of the optical nerve can use as an effective imaging indicator for detecting DON.
Backgrounds
Dysthyroid optic neuropathy (DON) is the main causes of blindness in Graves orbitopathy (GO) patients, which is difficult to diagnose in its early stage. Therefore, weevaluated the ability of quantitative multimodal magnetic resonance imaging(MRI) indicatorsto predict the presence of DON.Methods
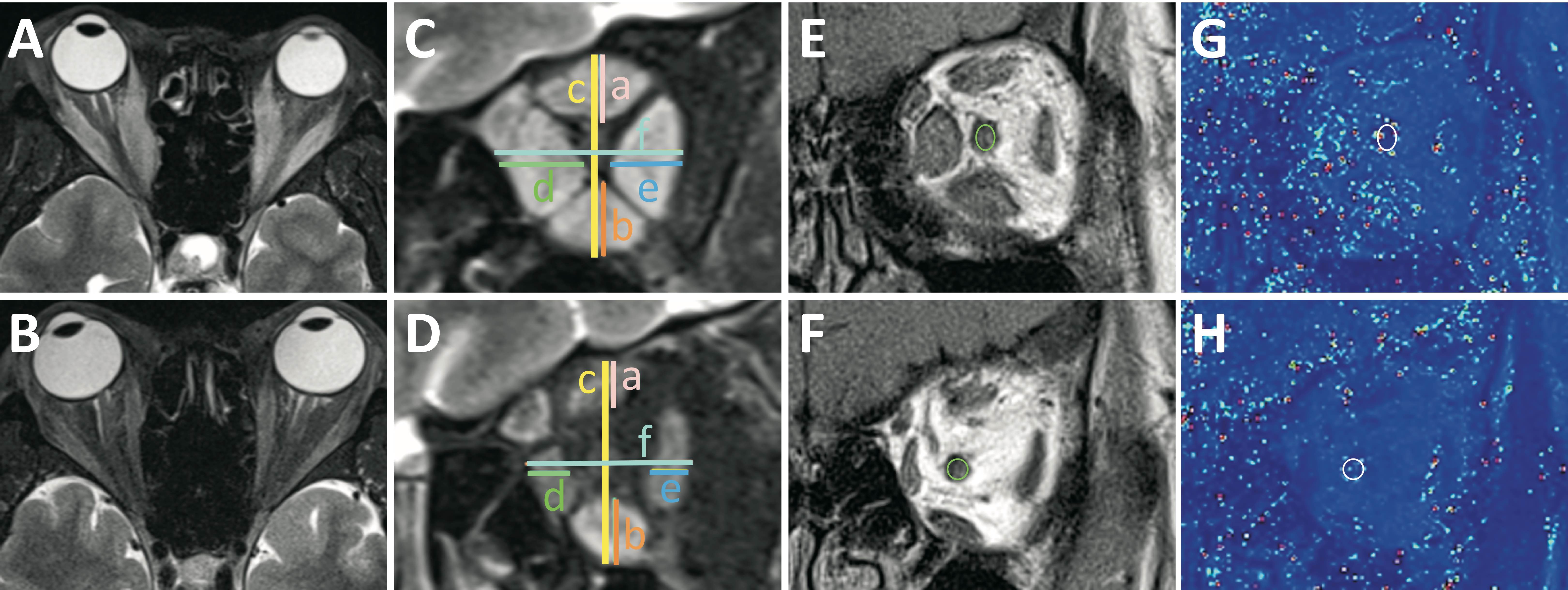
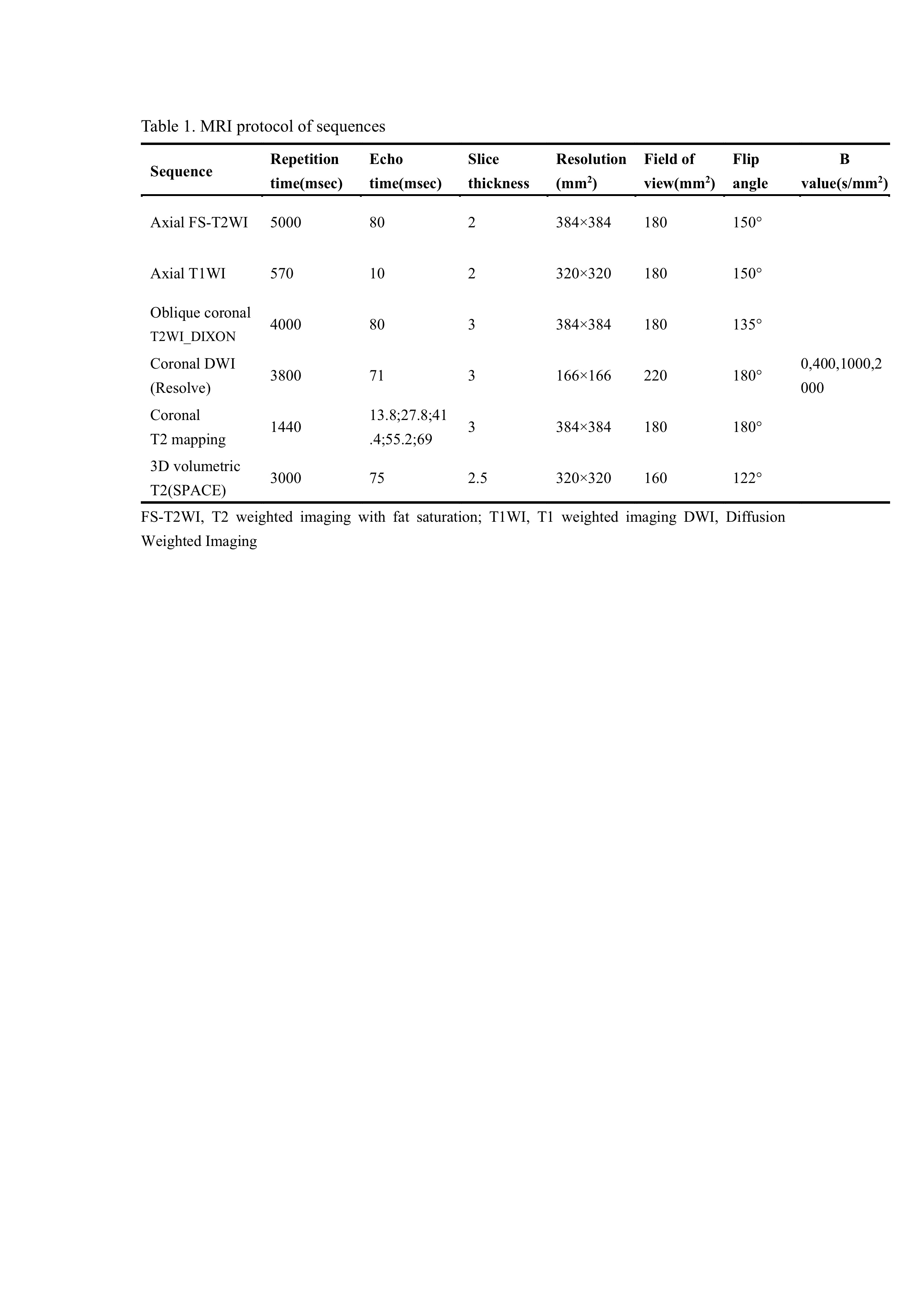
We retrospectively collected and analyzed the clinical features and MRI data of 59 GO patientswith and without DON. MRI was performed using a 3T unit (Siemens Magnetom Trio, Erlangen, Germany). The sequence parameters are shown in Table 1. MRI quantitative parameters, including modified muscle index (mMI), proptosis, volume of intraorbital fat, mean ADC value and T2 value of the optic nerve, were compared between patients with and without DON. Logistic regression analysis was performed to identify risk factors associated with the presence of DON. Receiver operating characteristic (ROC) curve analysis and decision curve analysis (DCA) were performed to evaluate the diagnostic efficiencyof theidentified indicators for DON.Results
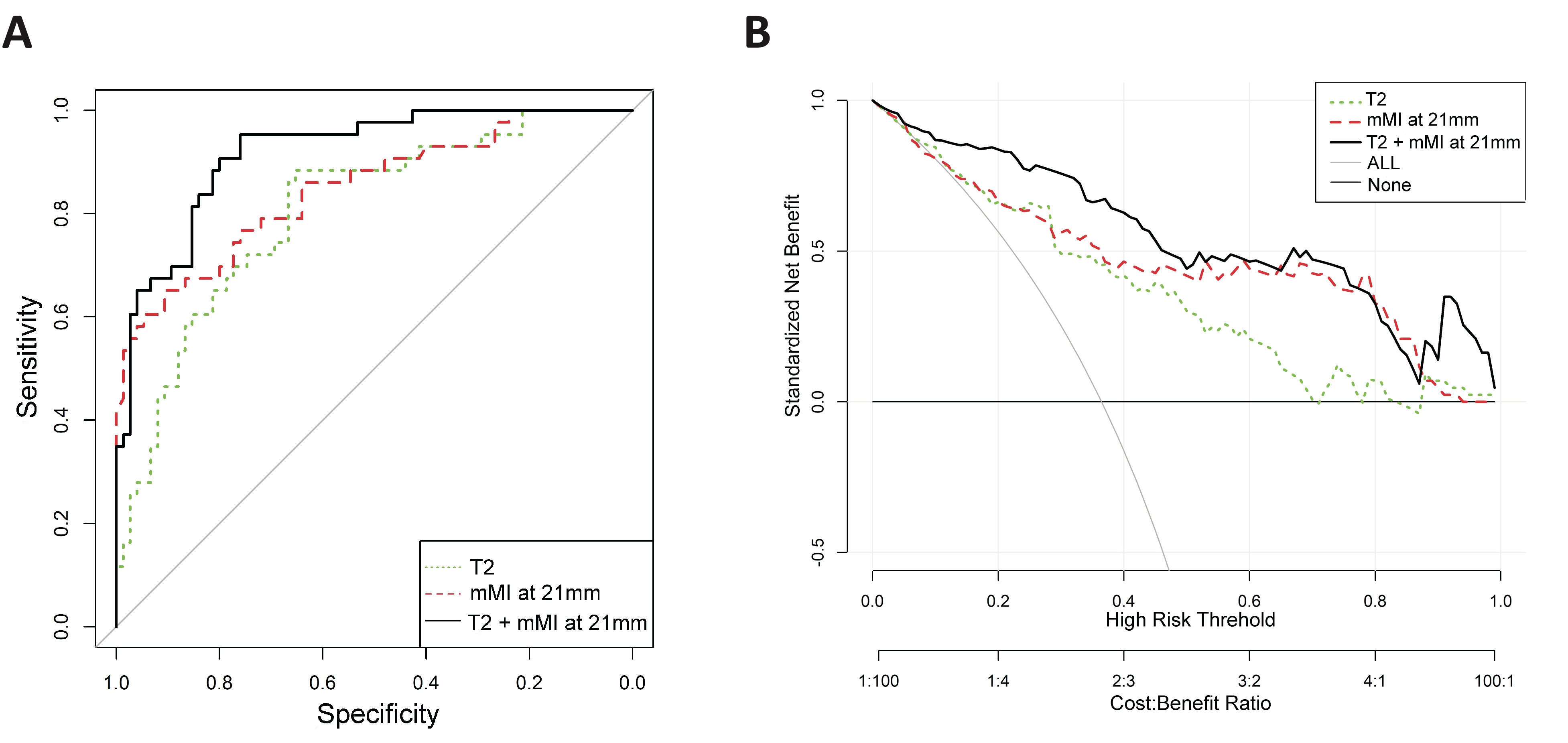
One hundred eight orbits (43 with and 75 without DON) were studied. The mMI and the mean T2 value of the optic nerve were significantly greater in orbits with DON than in those without DON (P <0.001).Multivariate regression analysis showed that mMIat 21 mmand mean T2 values of the optic nerve were independent predictors of DON. Greater mMI at 21mm (odds ratio [OR], 1.039; 95% confidence interval [CI]: 1.019, 1.058) and a higher mean T2 value of the optic nerve (OR, 1.035; 95% CI: 1.017, 1.054) were associated with a high risk of DON. A model combining mMI at 21 mm and mean T2 values for the optic nerve was an effective parameter for predicting DON in GO patients, with a sensitivity of 95.3% and a specificity of 76%.Moreover,DCA indicated that the model combining mMI at 21 mm and mean T2 value of the optic nerve was of great value in DON diagnosis.Discussion
Dysthyroid optic neuropathy (DON) is one of the most severe types of Graves orbitopathy (GO) and requires urgent treatment to prevent blindness. However, DON is frequently difficult to diagnose clinically in its early stages because of confounding signs and symptoms of congestive orbitopathy. In our study, we evaluate orbital condition of DON patients by using quantitative multimodal MRI, which include anatomical and functional indicators. we found that mMI and the mean T2 value of the optic nerve were significantly greater in orbits with DON than in those without DON. We innovatively used MRI to evaluate muscle index, which is the sensitivity of the soft tissue image contrast to tissue composition and can be a reflection of physiology and pathophysiology. In addition, increase of T2 value is a novel indicator of DON, which represents microscopic changes ofedema in the optic nerve. Finally, by conjointly analyzing anatomical and functional indicators, we found that mMI (at 21 mm) combined with the mean T2 value of the optical nerve can use as an effective imaging indicator for detecting DON.Conclusion
A quantitative multimodalMRI indicator combining mMI at 21 mm and the mean T2 value of the optical nerve can be an effective diagnostic method for detecting DON.Acknowledgements
No acknowledgement found.References
1. Blandford AD, Zhang D, Chundury RV, Perry JD 2017 Dysthyroid optic neuropathy: update on pathogenesis, diagnosis, and management. Expert Rev Ophthalmol 12:111-121.
2. Preeti Thyparampil MMTY, MD 2016 Compressive Optic Neuropathy in Thyroid Eye Disease. International Ophthalmolgy Clinics 56:51-67.
3. Saeed P, Tavakoli Rad S, Bisschop P 2018 Dysthyroid Optic Neuropathy. Ophthalmic Plast Reconstr Surg 34:S60-S67.
Figures