3460
Multi-parameter model proposes a comprehensive imaging index for degenerative cervical myelopathy diagnosis: a preliminary study1Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 2Department of spine surgery, Beijing Jishuitan Hospital, Beijing, China, 3Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 4Electrical Engineering and Computer Sciences, University of California, Berkeley, Berkeley, CA, United States, 5Department of Radiology, Beijing Jishuitan Hospital, Beijing, China
Synopsis
DTI and MTR have been reported to be useful in aiding the diagnosis of DCM. Some of the DTI and MTR metrics are significantly correlated with mJOA and thus can assist clinical assessment. However, previous studies have tended to only focus on a limited number of metrics. We aim to propose a comprehensive imaging index that correlates well with mJOA. It is based on the analysis of multiple metrics in different ROIs. In this preliminary study, we examine the correlation between mJOA and metrics at the C2 level. The plan and framework of the follow-up study are also presented.
Introduction
Degenerative cervical myelopathy (DCM) is the usual cause of chronic spinal cord injury. Imaging modalities are involved in the diagnosis of this disease. Many previous studies have reported that some DTI and MT metrics are significantly correlated with the modified Japanese Orthopedic Association scale (mJOA) [1][2][3][4], the major clinical assessment for DCM patients. Although these studies have yielded fairly good results, there is still a need for further works. First, most of the studies tended to focus on a single metric. However, DCM is likely to affect the patients in disparate aspects, and thus multiple metrics change. Second, it is necessary to demonstrate the metric outcomes of different regions-of-interest (ROIs).This study aims to generate an image index that correlates well with mJOA. It is based on a multi-parameter model that considers different metrics from various ROIs. And it can be utilized to interpret or even predict the mJOA for a patient. As a preliminary study, this abstract investigates the correlation between mJOA and five metrics. All the metrics were extracted in eight different ROIs at the C2 level. Additionally, The plan and framework for our future work were covered in the discussion section.
Data Acquisition
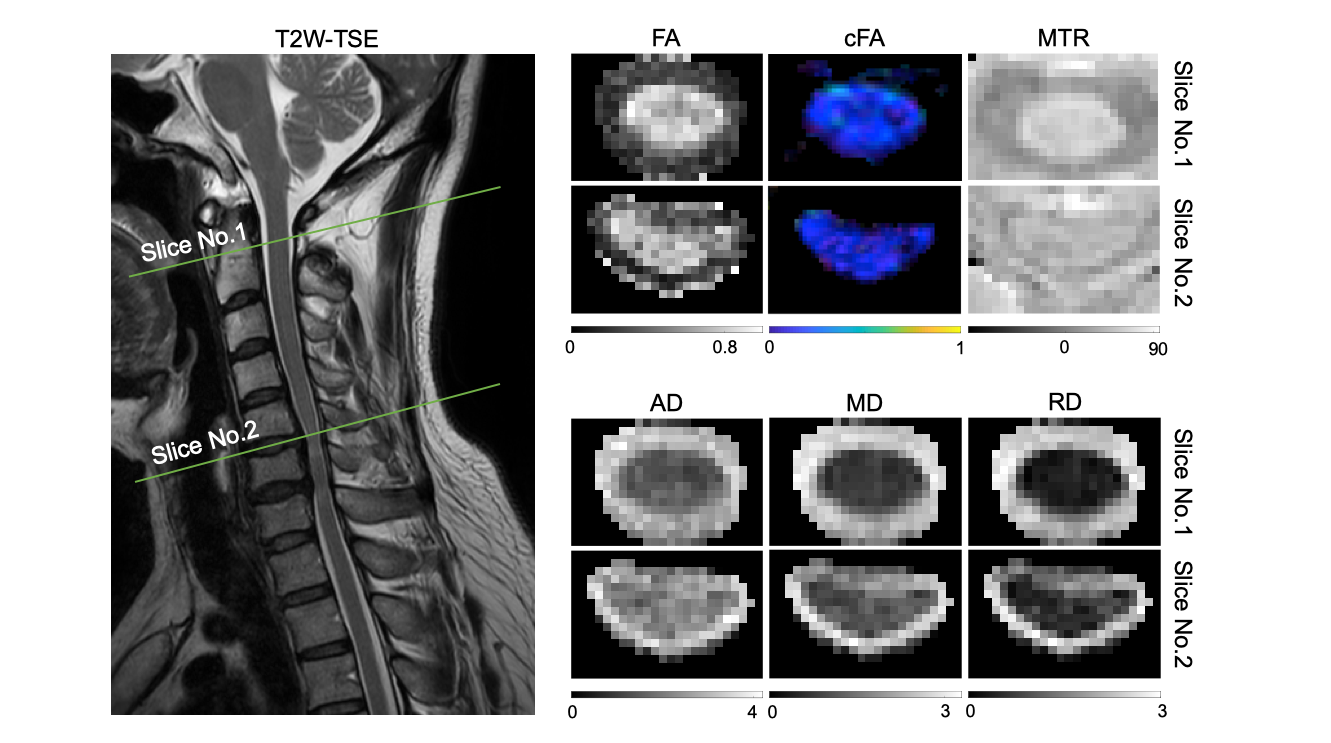
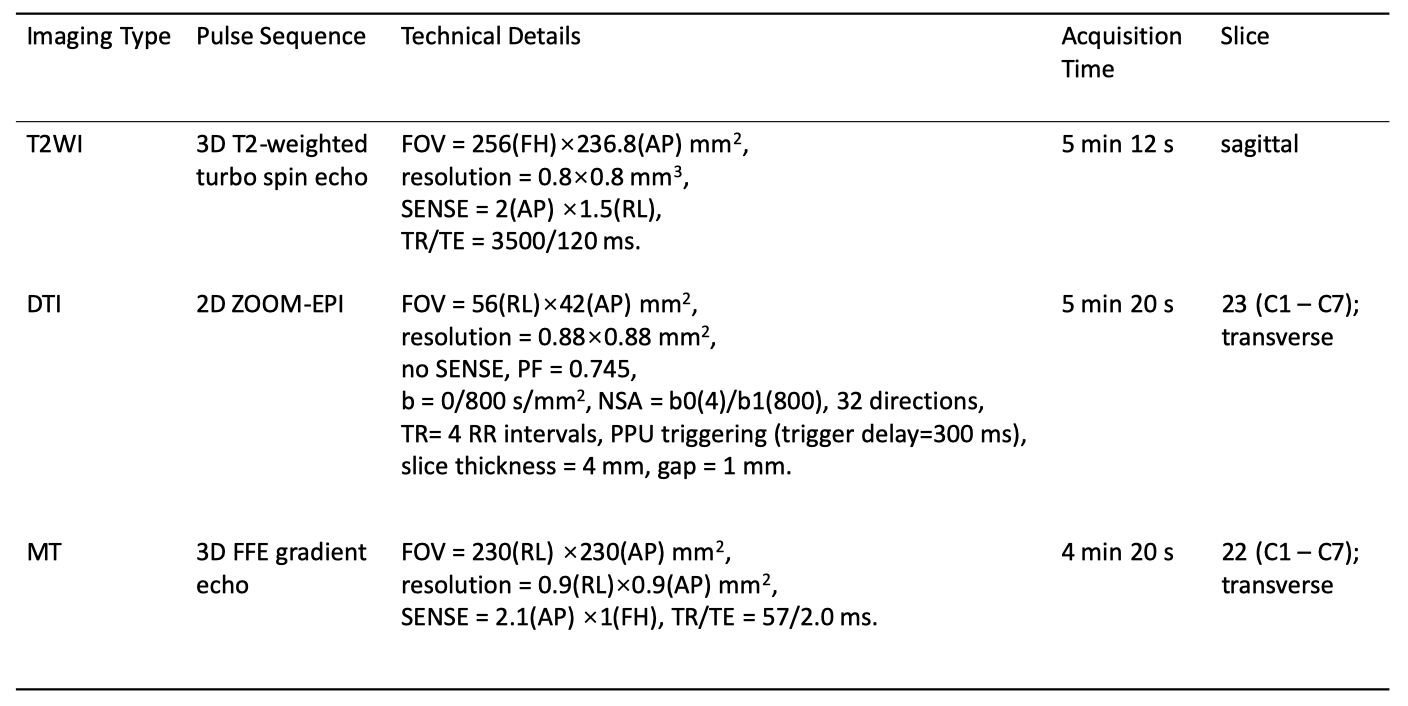
Sixty-one patients and ten healthy volunteers were recruited with written consent. The study was approved by the Institutional Review Board. All patients were clinically accessed by mJOA. And each subject was scanned by a Philips 3T Ingenia CX scanner (Philips Healthcare, Best, The Netherlands) using a 16-channel spine coil. Table 1 shows the technical details of the applied sequences.Data Analysis
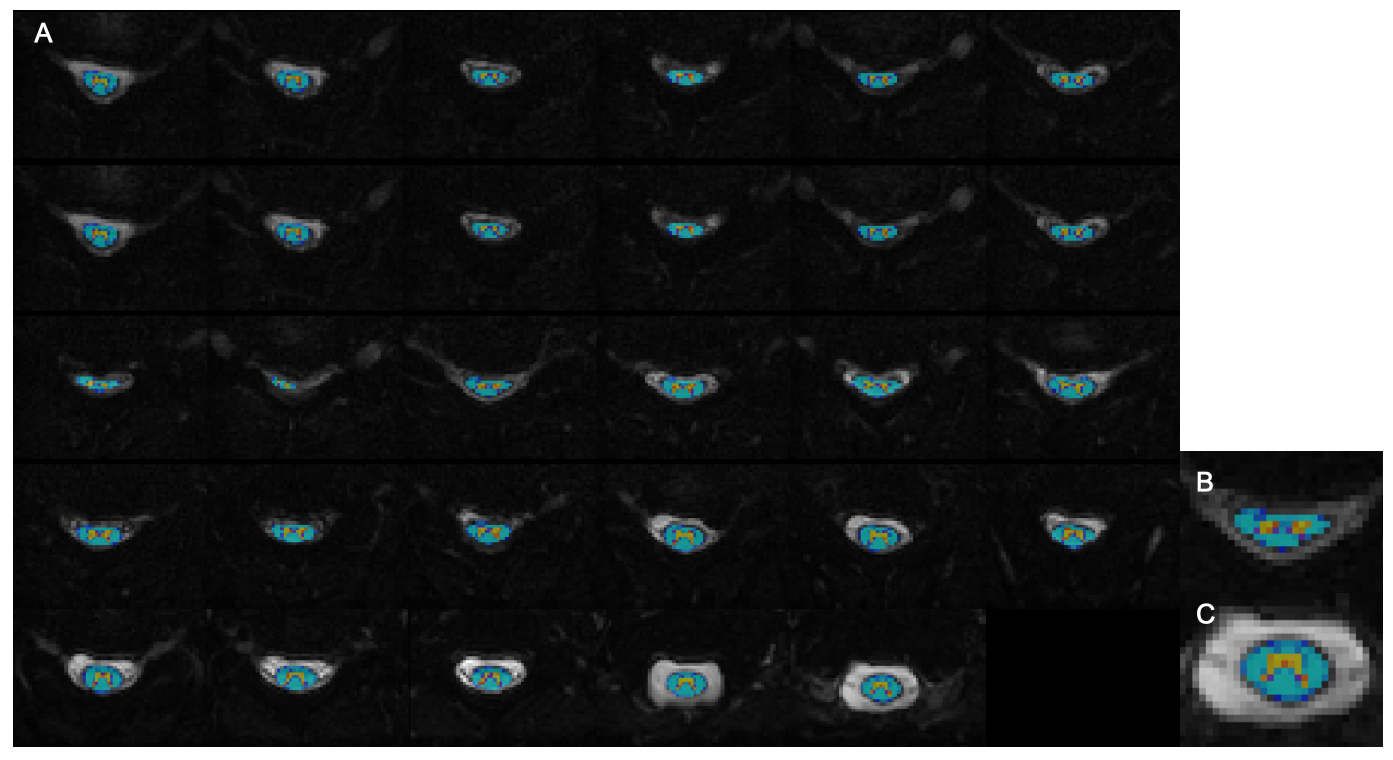
DTI and MT data were processed by the Spinal Cord Toolbox[5]. We did the motion correction first and then registered the PAM50 template[6] to the image. For every slice, we selected eight ROIs: the whole spinal cord, white matter, gray matter, dorsal columns, lateral funiculi, ventral funiculi, WM left spinal lemniscus, and WM right spinal lemniscus. Figure 1 shows the registration result of one patient.After that, the image metrics we chose were fractional anisotropy (FA), axial diffusivity (AD), radial diffusivity (RD), mean diffusivity (MD), and magnetic transfer rate (MTR). The metrics in each ROI were calculated automatically by the toolbox, and the results are shown in Figure 2.
Statistical analysis was performed using MATLAB (Mathworks), Version 2019b. Metrics in all ROIs of C2 level was correlated with mJOA by the Pearson correlation.
Results and Discussion
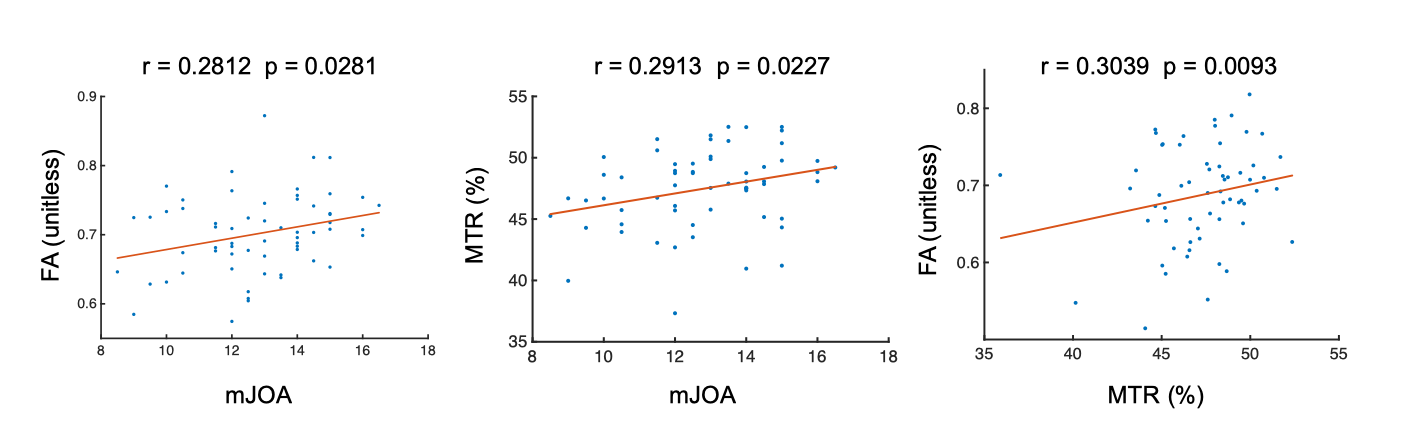
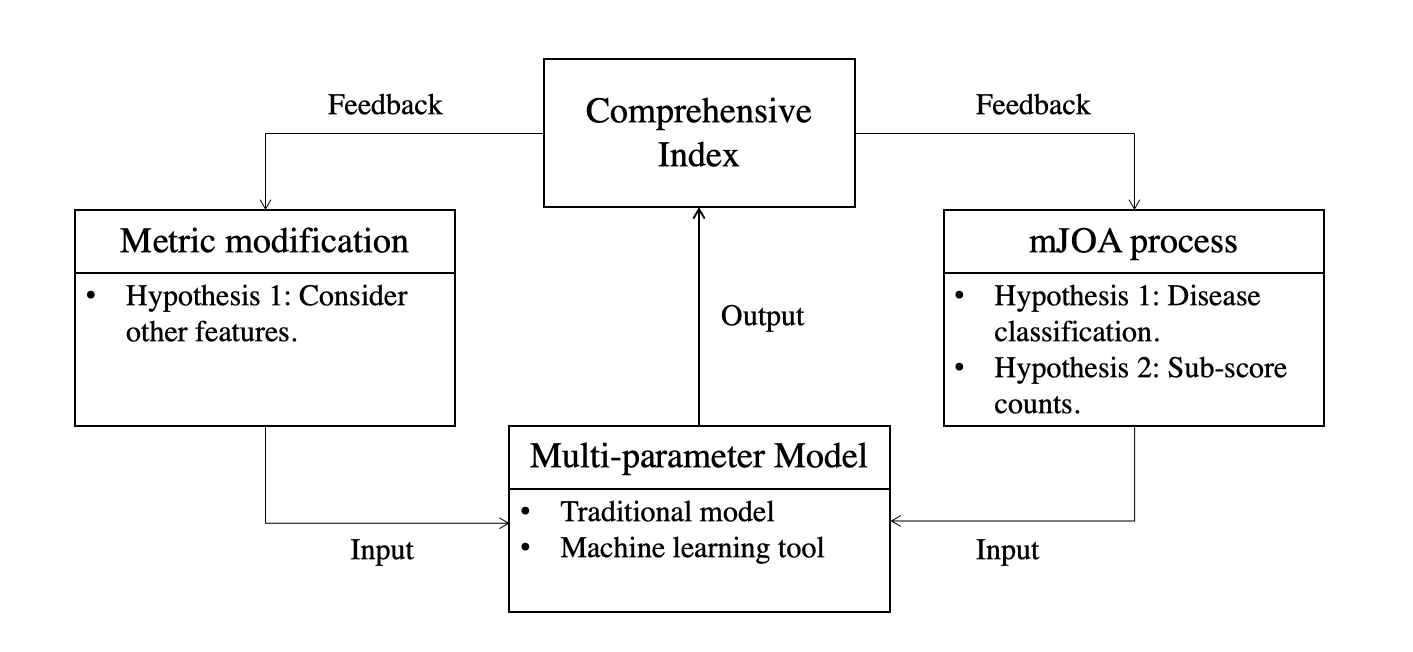
At the C2 level, only FA and MTR in the dorsal column (DC) were significantly correlated with mJOA, as shown in Figure 4. This result of FA is consistent with some studies.[7] But the correlation between the mJOA and MTR in DC has not been reported before. What's more, FA and MTR also have a significant correlation, as shown in Figure 4.This result only shows our work so far, and most of the study will be done in the future. The future research framework is shown in Figure 4. And we will verify 3 hypotheses first.
Hypothesis 1: Many other metrics are well correlated with mJOA.
In our following work, we will continue to increase the number of metrics we survey. Other metrics include the cross-sectional area (CSA), age, etc. Some of these features have been proven to affect DTI and MT metrics[8], so it is probably feasible to find out their correlation with the mJOA.
Hypothesis 2: A specific disease leads to a specific metric change in some ROIs.
There are 3 disorders in our study: cervical disc herniation (CDH), cervical spondylotic myelopathy (CSM), and ossification of the posterior longitudinal ligament (OPLL). It is a simple assumption that a disease has a special influence on patients. The metrics in specific ROIs will thus change. We will classify patients according to the type of their disease. Each category will be considered separately to find out whether there is a relationship between the disease classification and metric variation.
Hypothesis 3: The sub-scores of mJOA have value for the correlation study.
The overall mJOA is the sum of seven sub-scores. A sub-score represents the clinical evaluation for a sensory or motor function of the patient. Likewise, each of these functions is associated with a unique ROI of the spinal cord. Hence, the mJOA sub-score may correspond to a particular ROI.
After the completion of the above work, we will finally try to build a model, using image metrics to fit mJOA. Traditional models like linear regression will be applied. Also, we will use other machine learning methods, as a previous study has proven the effectiveness of artificial intelligence in this field.[9]
In short, further study will consider more parameters and will be much more detailed and thorough. The ultimate goal of our study is to generate a comprehensive index that can interpret and predict mJOA. We hope this index can assist clinical diagnosis for DCM patients.
Acknowledgements
No acknowledgement found.References
[1] Wen CY, Cui JL, Liu HS, Mak KC, Cheung WY, Luk KD, Hu Y. Is diffusion anisotropy a biomarker for disease severity and surgical prognosis of cervical spondylotic myelopathy?. Radiology. 2014 Jan;270(1):197-204.
[2] Ellingson BM, Salamon N, Grinstead JW, Holly LT. Diffusion tensor imaging predicts functional impairment in mild-to-moderate cervical spondylotic myelopathy. The Spine Journal. 2014 Nov 1;14(11):2589-97.
[3] Cloney MB, Smith ZA, Weber KA. Quantitative magnetization transfer MRI measurements of the anterior spinal cord region are associated with clinical outcomes in cervical spondylotic myelopathy. Spine. 2018 May 15;43(10):675.
[4] Han X, Ma X, Li D, Wang J, Jiang W, Cheng X, Li G, Guo H, Tian W. The Evaluation and Prediction of Laminoplasty Surgery Outcome in Patients with Degenerative Cervical Myelopathy Using Diffusion Tensor MRI. American Journal of Neuroradiology. 2020 Sep 1;41(9):1745-53.
[5] De Leener B, Lévy S, Dupont SM, Fonov VS, Stikov N, Collins DL, Callot V, Cohen-Adad J. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage. 2017 Jan 15;145:24-43.
[6] De Leener B, Fonov VS, Collins DL, Callot V, Stikov N, Cohen-Adad J. PAM50: Unbiased multimodal template of the brainstem and spinal cord aligned with the ICBM152 space. Neuroimage. 2018 Jan 15;165:170-9.
[7] Martin AR, De Leener B, Cohen-Adad J, Aleksanderek I, Cadotte DW, Kalsi-Ryan S, Tetreault L, Crawley A, Ginsberg HJ, Fehlings MG. 163; Microstructural MRI Quantifies Tract-Specific Injury and Correlates With Global Disability and Focal Neurological Deficits in Degenerative Cervical Myelopathy. Neurosurgery. 2016 Aug 1;63:165.
[8] Taso M, Girard OM, Duhamel G, Le Troter A, Feiweier T, Guye M, Ranjeva JP, Callot V. Tract‐specific and age‐related variations of the spinal cord microstructure: a multi‐parametric MRI study using diffusion tensor imaging (DTI) and inhomogeneous magnetization transfer (ihMT). NMR in Biomedicine. 2016 Jun;29(6):817-32.
[9] Jin R, Luk KD, Cheung JP, Hu Y. Prognosis of cervical myelopathy based on diffusion tensor imaging with artificial intelligence methods. NMR in Biomedicine. 2019 Aug;32(8):e4114.
Figures