3297
Hepatic iron quantification using a Free-breathing 3D Radial Dixon technique and validation with a 2D GRE biopsy calibration1Department of Diagnostic Imaging, St. Jude Children's Research Hospital, Memphis, TN, United States, 2Department of Biomedical Engineering, The University of Memphis, Memphis, TN, United States, 3Siemens Medical Solutions USA, Inc., Los Angeles, CA, United States, 4MR Application Development, Siemens Healthcare, Erlangen, Germany, 5University of New South Wales, Sydney, Australia, 6Department of Hematology, St. Jude Children's Research Hospital, Memphis, TN, United States
Synopsis
Radial acquisitions are less motion sensitive and a viable alternative in patients unable to breath-hold. This study investigates a free-breathing 3D Radial Dixon technique to assess HIC by validating with 3D Cartesian Dixon and biopsy-calibrated 2D GRE method. All three acquisitions showed excellent correlation with each other. The free-breathing 3D Radial Dixon produced sharper images whereas the 2D GRE and 3D VIBE Cartesian-based techniques exhibited motion artifacts and a slight underestimation in R2* values compared to 3D Radial VIBE likely due to motion artifacts.
Introduction
Hepatic iron content (HIC) is an important parameter that guides management of patients with iron overload. Currently, non-invasive HIC assessment is performed based on published R2*-MRI versus biopsy-HIC calibration curves.1,2,3 However, these curves were derived by acquiring 2D multi-echo gradient echo (GRE) images from a single central liver slice and calculating R2* by fitting a mono-exponential model, which may produce inaccurate results in patients with co-existing fat. Recently, 3D Dixon techniques and multi-spectral fat-water models have been investigated for providing whole liver coverage and for simultaneous quantification of R2* and fat-fraction (FF).4,5 However, these acquisition techniques are based on Cartesian sampling and require the patient to perform a breath-hold for ~21 seconds to avoid breathing artifacts. Alternatively, radial sampling is less motion sensitive and can produce excellent image quality even in patients that are unable to perform a breath-hold.4 The purpose of this study is to investigate the performance of a free-breathing 3D Radial Dixon technique and validate the HIC quantification with 3D Cartesian Dixon and published 2D GRE biopsy calibration methods.Methods
MRI data was collected from 25 patients aged 5 to 25 years who underwent imaging at 1.5T scanner (MAGNETOM Avanto fit, Siemens Healthineers, Erlangen, Germany) using (a) 2D GRE (TR/TE/ΔTE 200/1.1/0.82ms, 20 echoes, α 35o, matrix 128x104, slice thickness 10mm), (b) 3D Cartesian Dixon Cartesian VIBE (TR/TE/ΔTE 11/0.93/0.96ms, 8 echoes, α 5o, 1.37 mm x 1.37 mm x 3.5mm), and (c) Radial Dixon VIBE (TR/TE/ΔTE 8.34/1.23/1.19ms, 6 echoes, α 5o, 1.52 mm x 1.52 mm x 5 mm). Quantitative R2* maps were calculated using a published 2D GRE method as the reference standard.3 Both R2* and FF maps were produced inline for 3D Cartesian VIBE and were processed offline for 3D Radial VIBE based on an adaptive multi-step fitting algorithm that is extended to account for magnitude noise.5 For each technique, mean R2* and FF values were calculated by drawing a large region-of-interest (ROI) and filtering out blood vessels in Matlab.6 The mean R2* values were converted into HIC values using a R2*-biopsy HIC calibration.3 R2*-HIC and FF values between each of the techniques were compared using linear regression and Bland-Altman analysis.Results & Discussion
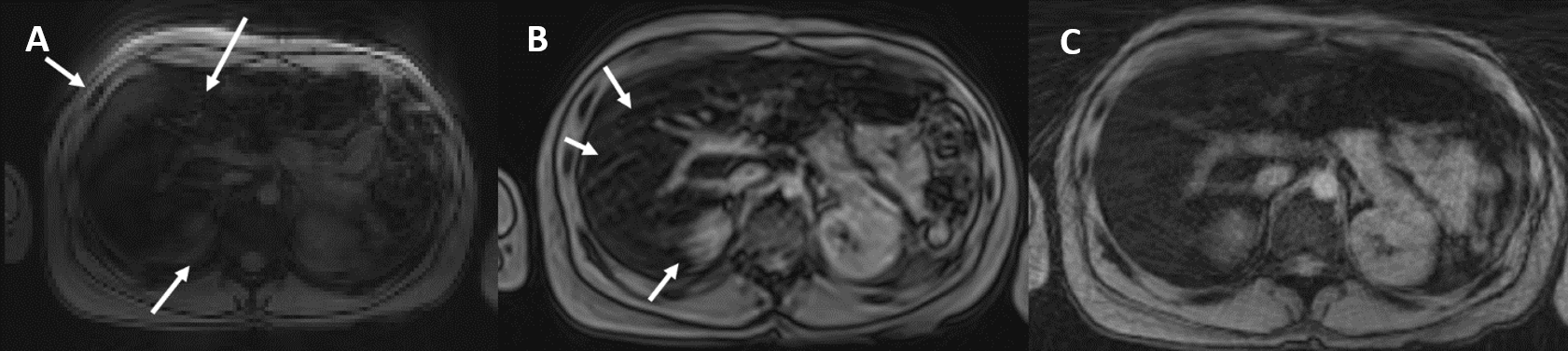
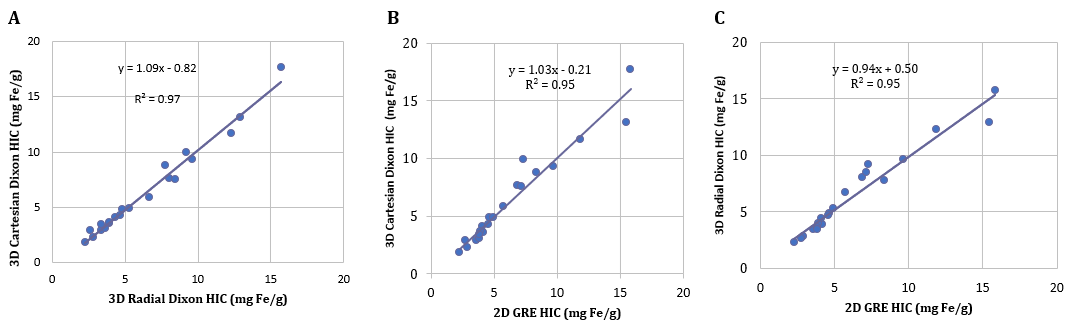
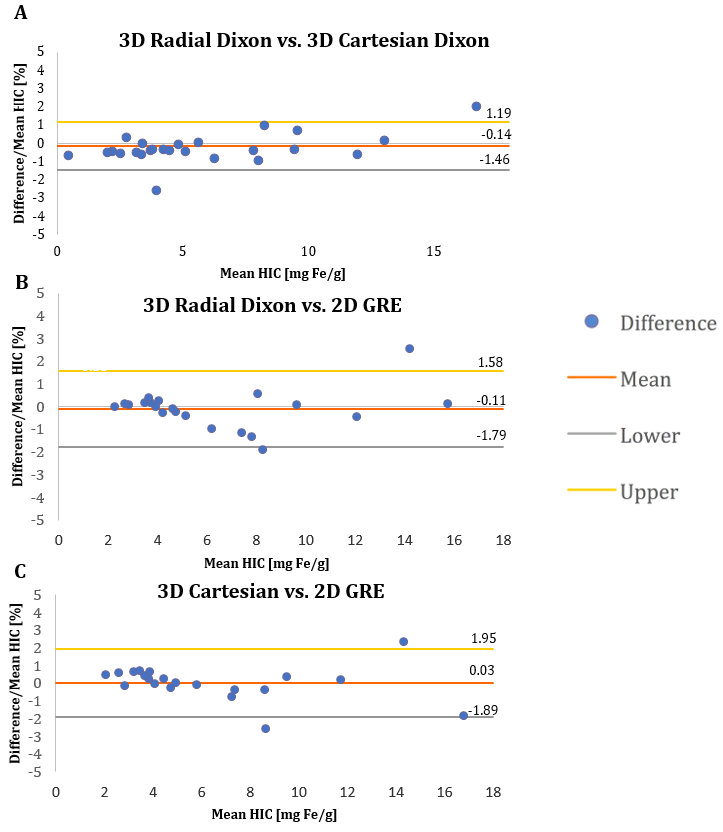
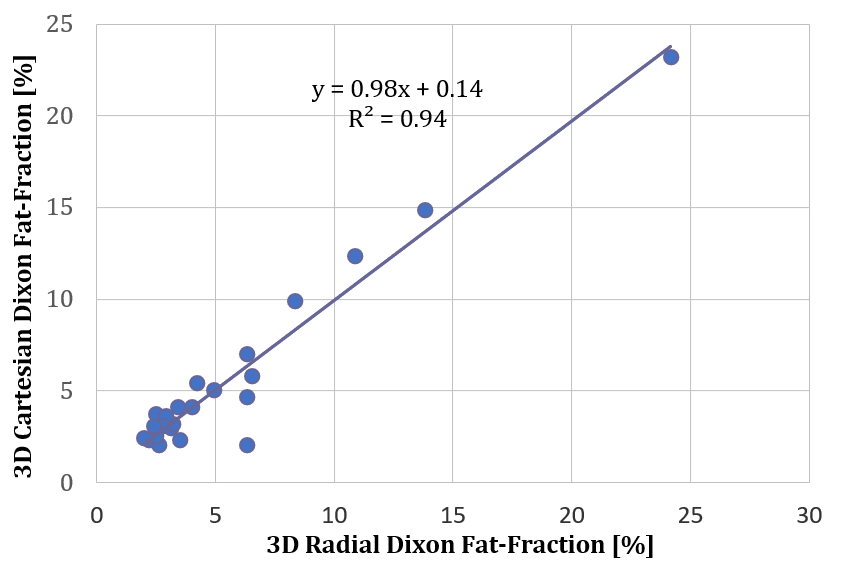
Of the 25 patients, 1 had fat-water swap and was excluded from further analysis. Of the 24, 3 patients had FF>10% and were excluded from R2* comparisons. Figure 1 shows magnitude images from all three acquisitions in a representative sedated patient unable to breath-hold. The images from the 2D GRE and 3D Cartesian Dixon showed motion artifacts (pointed out by white arrows), whereas 3D Radial was more robust to motion artifacts and produced a sharper image. As evident in Figs. 2 and 3, all three acquisitions showed excellent correlation between each other and mean biases close to zero. However, the R2* values for 2D GRE and 3D VIBE Cartesian-based techniques showed slight underestimation compared to R2* values of 3D Radial VIBE due to motion artifacts (Fig. 2). The FF values obtained with 3D Radial and Cartesian Dixon sequences also showed high correlation with slope close to unity (Fig. 4).Conclusion
The excellent agreement between the 3D Radial Dixon technique and the 3D Cartesian Dixon and 2D GRE techniques demonstrates that the 3D Radial Dixon method can accurately estimate HIC for guiding iron chelation therapy. The free-breathing 3D Radial Dixon will be a viable alternative in patients unable to breath-hold by providing sharper images with less motion artifacts compared to Cartesian-based techniques.Acknowledgements
No acknowledgement found.References
1. Wood JC, Enriquez C, Ghugre N, et al. MRI R2 and R2* mapping accurately estimates hepatic iron concentration in transfusion-dependent thalassemia and sickle cell disease patients. Blood. 2005;106(4):1460-1465.
2. Henninger B, Zoller H, Rauch S, et al. R2* relaxometry for the quantification of hepatic iron overload: biopsy-based calibration and comparison with the literature. RoFo : Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin 2015;187(6):472-479.
3. Hankins JS, McCarville MB, Loeffler RB, et al. R2* magnetic resonance imaging of the liver in patients with iron overload. Blood. 2009;113(20):4853-4855.
4. Tipirneni-Sajja A, Krafft AJ, McCarville MB, et al. Radial Ultrashort TE Imaging Removes the Need for Breath-Holding in Hepatic Iron Overload Quantification by R2* MRI. AJR Am J Roentgenol. 2017;209(1):187-194.
5. Jhaveri KS, Kannengiesser SAR, Ward R, Kuo K, Sussman MS. Prospective Evaluation of an R2* Method for Assessing Liver Iron Concentration (LIC) Against FerriScan: Derivation of the Calibration Curve and Characterization of the Nature and Source of Uncertainty in the Relationship. J Magn Reson Imaging. 2019;49(5):1467-1474.
6. McCarville MB, Hillenbrand CM, Loeffler RB, et al. Comparison of whole liver and small region-of-interest measurements of MRI liver R2* in children with iron overload. Pediatr Radiol. 2010;40(8):1360-1367.
Figures