3260
Neural Network for Autonomous Segmentation and Volumetric Assessment of Clot and Edema in Intracerebral Hemorrhages1Medical Physics, University of Wisconsin at Madison, Madison, WI, United States, 2Electrical Engineering, University of Wisconsin at Madison, Madison, WI, United States, 3Neurological Surgery, University of Wisconsin at Madison, Madison, WI, United States, 4Radiology, University of Wisconsin at Madison, Madison, WI, United States, 5Biomedical Engineering, University of Wisconsin at Madison, Madison, WI, United States
Synopsis
Previous work has shown that minimally-invasive reduction of hematoma volume in intracerebral hemorrhage to a threshold of 15mL is indicative of improved long term patient outcome. To attain this goal, image-guided minimally-invasive surgical techniques are applied to both lyse clot material and drain from the site of hemorrhage via a porous catheter. We propose a Convolutional Neural Network to identify and autonomously segment clot and peripheral edema in MR images of the brain for volumetric analysis, and image-guidance during evacuation. Quantitative measurements produced in this way can be used for superior clot visualization and direct measurement of remaining clot volume.
Introduction
Quantification of residual clot volume of intracerebral hemorrhages (ICH) after minimally-invasive treatment is perhaps the best indicator of treatment efficacy and improvement in patient independence. The international Phase III MISTIE Trial, which used CT-image guidance to position a catheter at the site of hemorrhage for periodic clot drainage and infusion of thrombolytic drugs (Fig. 1), failed to meet its clinical endpoint for all patients. However, a subset of patients with less than 15 ml of residual clot showed statistically significant reductions in morbidity and improved independence1. The Trial concluded that improved guidance was needed to help a wider set of neurosurgeons meet the residual goal without endangering rebleeds.We previously proposed that the superior contrast of T2-W MRI could be used to visualize and quantify the extent of clot evacuation remaining periodically during treatment. We developed a Convolutional Neural Network (CNN) to identify and segment regions of clot and edema2. After securing further ICH datasets from our institution, we further refined the network and can now present measurements of segmentation accuracy, clot volume, and edema volume using a sufficient number of independent test sets.
Methods
Data Processing:Developing MRI training sets from ICH patients is complicated by time-varying contrast after hemorrhagic onset, motion artifacts from cognitive impairment, and lack of uniform protocols. To avoid age-varying contrast as hemoglobin breaks down3, we utilized only images acquired within 4 days of patient admission. Due to varying patient protocols, we used only T2-W imaging, as this was most commonly acquired. From our institution’s records, a set of 18 de-identified axial T2-weighted MR scans with fat saturation, taken on GE Healthcare scanners, were selected for use in training and validating. Figure 2 outlines cases for exclusion that either lack sufficient image quality, or are not compatible with minimally-invasive surgical approaches. Clot and edema columns of each image were manually segmented4 by a radiologist-trained imaging scientist. Subject to these same constraints, 11 more cases (29 total) were acquired and segmented for testing. For more assurance of accuracy, testing cases were segmented by two individuals. Independently-performed segmentations were found to be in high agreement with each other for both clot (Rsquared = 0.992), and edema (Rsquared = 0.896).
Network Architecture:
Our proposed CNN followed a UNet-styled architecture5 with 5 sets of convolution-deconvolution layers to extract image features and generate binary masks for relevant regions (Fig. 3). Notably, the process utilizes two separate CNNs, one trained to identify edema, and for clot core. Each produces its own segmented region, then the two are combined into a single mask displaying both segmentations. Separate networks were used such that each could be optimized individually. The models were constructed using the Keras toolbox for Python6.
Training and Evaluation:
The image-manual segmentation pairs were sorted on a case-by-case basis into training and validation datasets. Data was split such that 16 cases were relegated to the training dataset, while the remaining 2 formed the validation set. The loss function was defined to maximize the Dice Coefficient (DC) of each machine segmentation compared to the provided manual ones. Each CNN was trained over 100 epochs. Trained models were applied to the yet-unused testing dataset for evaluation.
Results
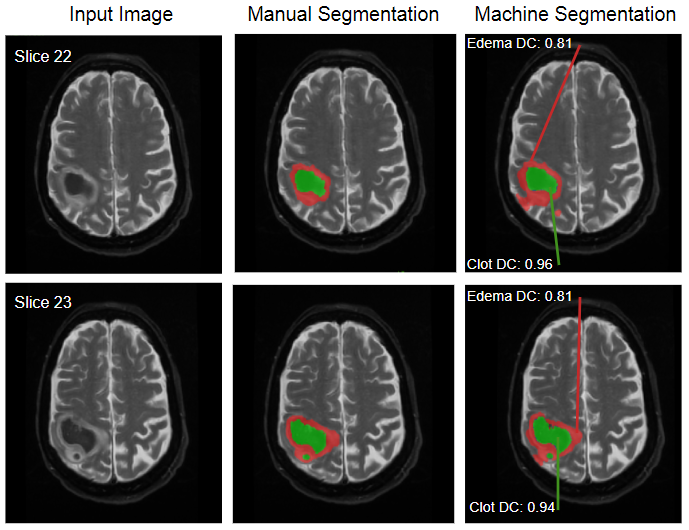
From the 11 testing cases, the model produced segmentations with average DCs of 0.735±0.138 on clot and 0.612±0.150 on edema. Figure 4 shows a machine-produced segmentation next to the manual segmentation, showing high agreement with both defined regions. Due to the dual-model structure of segmentation, some pixels were attributed to both clot and edema. These uncertain pixels make up less than 1% of total segmented volume (0.18%). The model tended to undersegment clot volumes, with a mean difference of -2.615 mL relative to manual segmentations’ volumes.Discussion
This model’s performance on the supplied dataset is promising for surgically relevant cases. Cases wherein the clot was exceedingly small or diffuse were excluded due to being ill-suited to surgical evacuation, as shown in Fig. 2. The same reasoning was applied to exclude intraventricular cases, where the bleeding breaches the ventricle and mixes with cerebrospinal fluid (CSF). While training was biased to younger clots, this aligns with the time window for which surgical evacuation is viable. Generally, clot segmentation was more accurate than edema, as a result of having more consistent image features.In practice, this model could be used to rapidly supply autonomous segmentations to neurosurgeons, neurologists, and neuroradiologists for clot visualization and assessments of residual hemorrhage volume (Fig. 5) periodically during clot evacuation procedures. This information would be valuable in assessing which portions of the residual clot can safely be treated further, while providing a running metric of the clot volume as evacuation progresses. Furthermore, the model’s ability to distinguish segmentation of peripheral edema from clot may serve to further specify exact boundaries of the clot, reducing risk of agitating hematoma boundaries and triggering a rebleed.
Conclusion
The segmentations produced by this CCN pipeline produced fast autonomous segmentations showing high agreement with manual segmentations of the same cases. This allows for convenient 3D-visualization and volume calculation of the clots and peripheral edema. This software could provide interventionalists with real-time imaging and quantification of intracerebral hemorrhages needed to guide minimally-invasive surgical evacuations.Acknowledgements
We acknowledge GE Healthcare and the University of Wisconsin - Madison ML4MI Program for research support.References
[1] Hanley DF, Thompson RE, Rosenblum M, Yenokyan G, Lane K, McBee N, Mayo SW, Bistran-HallAJ, Gandhi D, Mould WA, Ullman N, Ali H, Carhuapoma JR, Kase CS, Lees KR, Dawson J, Wilson A, Betz JF,Sugar EA, Hao Y, Avadhani R, Caron JL, Harrigan MR, Carlson AP, Bulters D, LeDoux D, Huang J, Cobb C,Gupta G, Kitagawa R, Chicoine MR, Patel H, Dodd R, Camarata PJ, Wolfe S, Stadnik A, Money PL, MitchellP, Sarabia R, Harnof S, Barzo P, Unterberg A, Teitelbaum JS, Wang W, Anderson CS, Mendelow AD,Gregson B, Janis S, Vespa P, Ziai W, Zuccarello M, Awad IA, Investigators MI. Efficacy and safety ofminimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): arandomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet. 2019. Epub 2019/02/12. doi:10.1016/S0140-6736(19)30195-3. PubMed PMID: 30739747.Melander A, Olsson J, Lindberg G, Ciaria MV, Ariano M,Strom R, Gibney J, Weiss U, Turner B, O'Gorman P, Watts G, Powrie J, Crook M, Shaw K, Cummings M.35th Annual Meeting of the European Association for the Study of Diabetes : Brussels, Belgium, 28September-2 October 1999. Diabetologia. 1999;42(Suppl 1):A1-A330. Epub 1999/08/01. doi:10.1007/BF03375458. PubMed PMID: 27770183.
[2] Lilieholm T, McMillan A, Liu F, Moskwa R, Ahmed A, Block WF, Tool for Image-guided Intracerebral Hemorrhage Evacuation: Automatic Segmentation of Clot, Edema, and Normal Brain Tissue, Proc. of International Society of Magnetic Resonance in Medicine, 2020.
[3] Voss, Yves L. “Timeline Diagram of MRI and CT Characteristics of Intracerebral Hemorrhage: Radiology Case.” Radiopaedia Blog RSS, Radiopaedia, radiopaedia.org/cases/timeline-diagram-of-mri-and-ct-characteristics-of-intracerebral-haemorrhage?lang=us.
[4] Paul A. Yushkevich, Joseph Piven, Heather Cody Hazlett, Rachel Gimpel Smith, Sean Ho, James C. Gee, and Guido Gerig. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006 Jul 1; 31(3):1116-28. doi:10.1016/j.neuroimage.2006.01.015
[5] Ronneberger O, Fischer P, and Brox T, “U-net: Convolutional networks for biomedical image segmentation.” International Conference on Medical image computing and computer-assisted intervention, 234–241 (2015).
[6] Chollet, F., & others. (2015). Keras. GitHub. Retrieved from https://github.com/fchollet/keras
[7] LeNail, (2019). NN-SVG: Publication-Ready Neural Network Architecture Schematics.Journal of Open Source Software, 4(33), 747
Figures