3241
Feasibility of free-breathing 3D isotropic whole-lung zero echo time imaging1Radiology, The first affiliated hospital of Guangzhou Medical University, Guangzhou, China, 2The first affiliated hospital of Guangzhou Medical University, Guangzhou, China, 3MR Research, GE Healthcare, Beijing, China, 4GE Healthcare, Beijing, China
Synopsis
The study assessed the feasibility and image quality of free-breathing 3D isotropic whole-lung zero echo time (ZTE) imaging. The overall image quality of the lung in most healthy subjects was good to excellent. The visibility of pulmonary arteries (up to the 7th generation) was better than the bronchi (up to the 5th generation). The demonstration of fissures was poor. In addition, one volunteer with azygos fissure was discovered in our study, which encourage us promote ZTE as a routine lung examination tool. The whole lung ZTE with free-breathing is feasible and can serve as an alternative method of chest imaging.
Introduction and purpose
Lung MRI can offer a radiation-free diagnostic option in chest imaging, which is especially relevant to children and pregnant women, as well as subjects who need to undergo repeated examinations such as treatment response assessment of lung cancer or diffuse lung diseases1,2. The aim of this study was to assess the feasibility of three-dimensional isotropic high-resolution lung MRI using a free-breathing zero-echo time (ZTE) imaging technique at 3.0 T MRI scanner.Materials and Methods
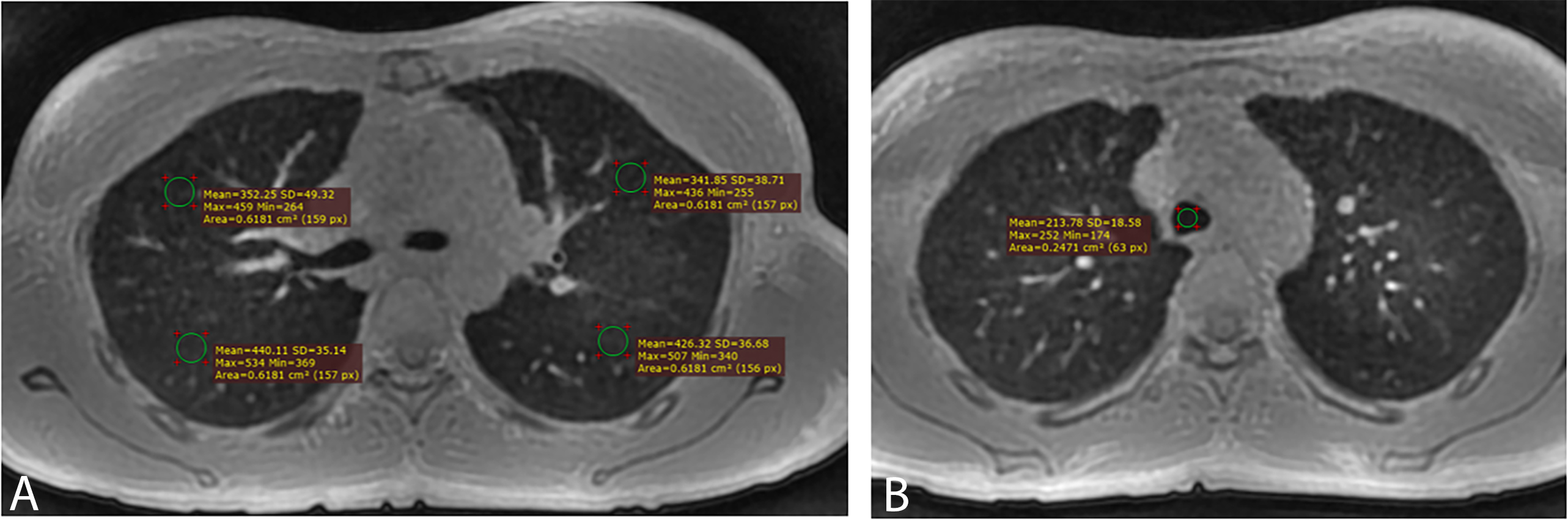
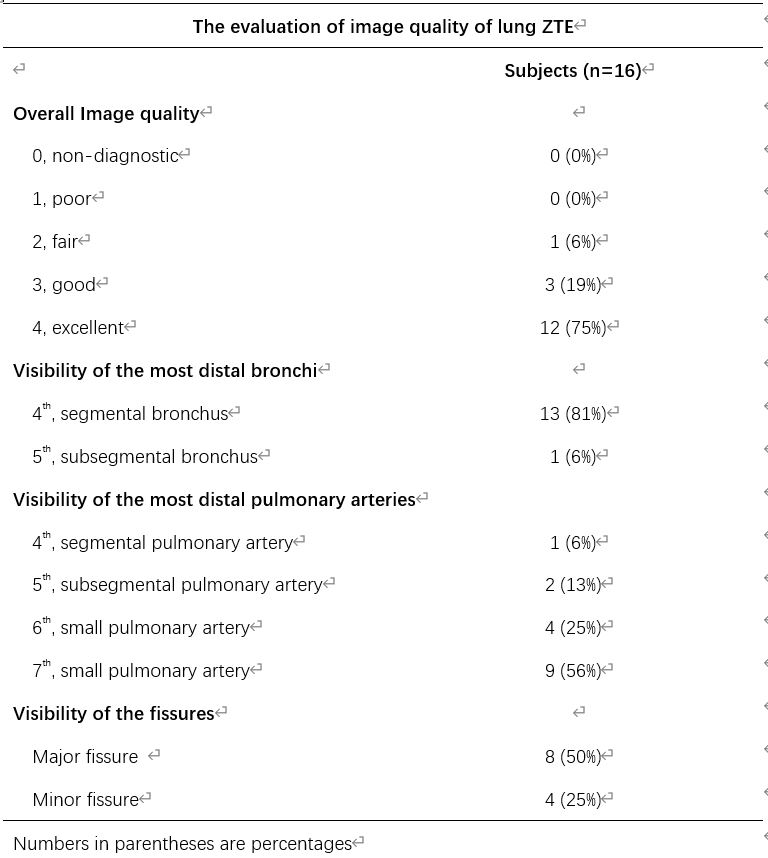
The study was approved by the local ethics committee. A total of sixteen healthy volunteers (8 males and 8 females, aged 24-26 years) were enrolled in this study and gave written informed consent. Half of the subjects underwent both axial and coronal ZTE scan, the other half underwent both axial and sagittal ZTE scan at a 3.0 T MRI scanner (Discovery MR750w, GE Healthcare, Waukesha, WI). The overall image quality (0, Non-diagnostic; 1, Poor; 2, Fair; 3, Good; 4, Excellent), the visible generation of the bronchi (trachea deemed as the 1st generation) and pulmonary arteries (pulmonary trunk deemed as the 1st generation), the visibility of the minor and major fissures, and the signal-to-noise ratio (SNR) of the lung parenchyma were evaluated by two independent chest radiologists3 (Fig. 1). The interobserver agreement for image quality and SNR were determined by the kappa coefficient and intraclass correlation coefficient (ICC), respectively. The difference of the image quality, SNR between axial scan and non-axial scans were compared as well. Statistical analyses were performed using MedCalc 19.5.6 (MedCalc Software Ltd, Belgium) or SPSS 22.0 (SPSS Inc. , Chicago, IL). A p value of < 0.05 was regarded as statistically significant.Results
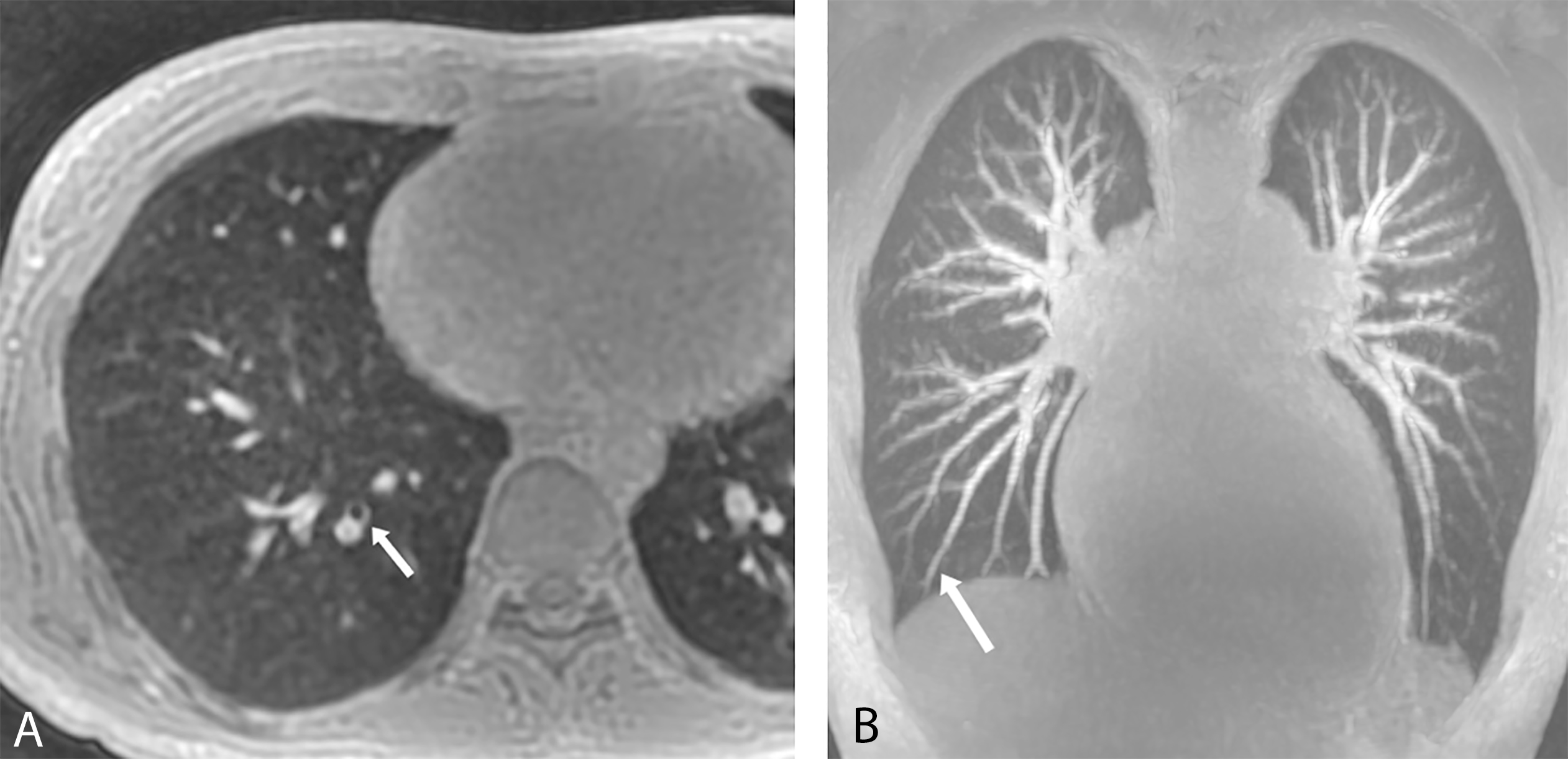
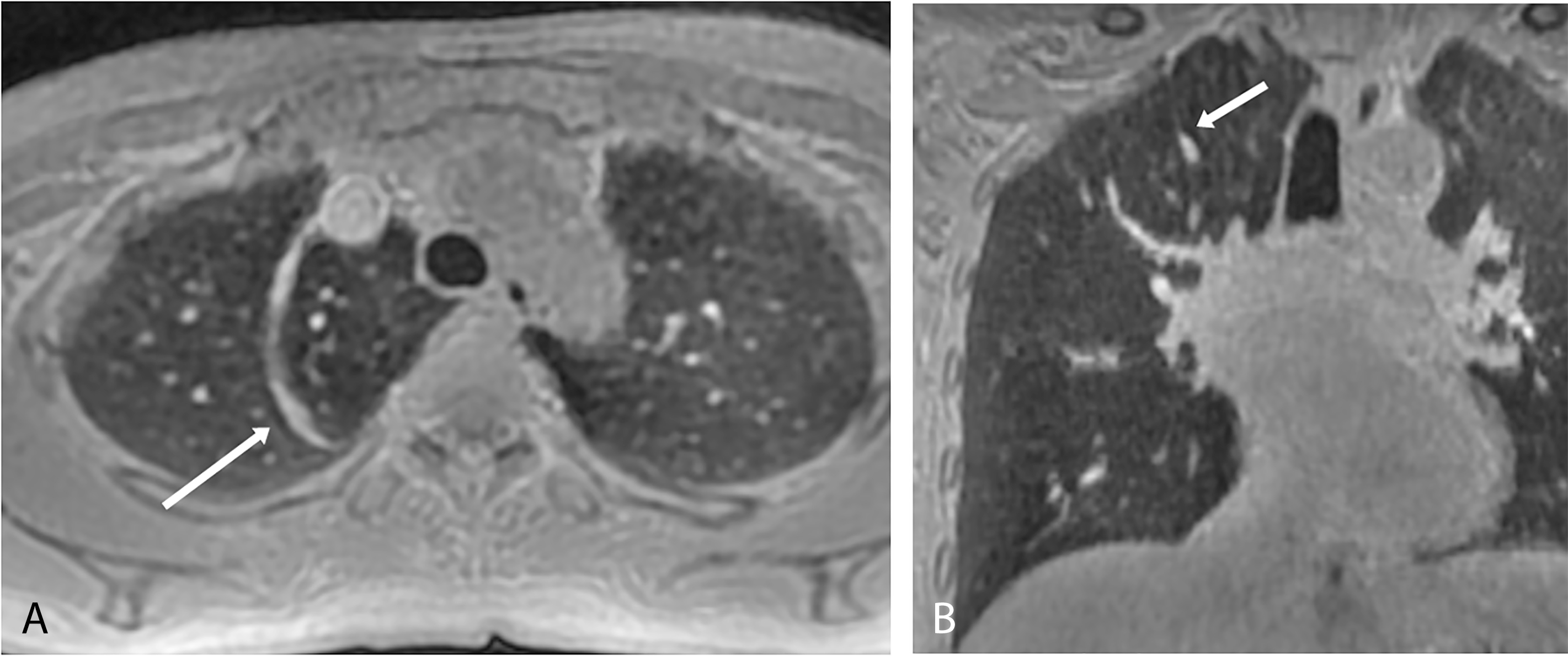
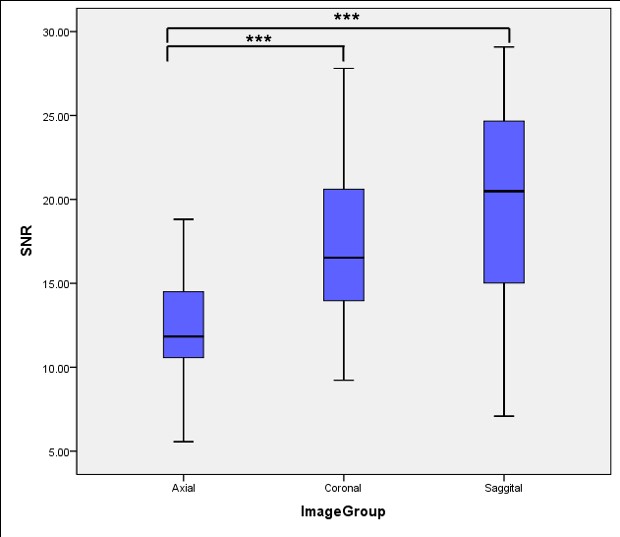
Fifteen cases (94%) showed good to excellent overall image quality. The bronchi were visible to the fourth generation in 13 case (81%) and in one case up to the fifth generation. The pulmonary arteries were visible to the sixth or seventh generation in 13 cases (81%) (Fig. 2 and Table 1). Minor and major fissures can be partial visualized in 25% (4/16) and 50% (8/16) of all subjects, respectively. An azygos fissure was found in one subject (Fig. 3). Good interobserver agreement for both image quality and SNR was found (0.706, 0.686, respectively). There was no difference of image quality between axial scan and coronal or sagittal scan (p=0.084, 0.317, respectively). The SNR of the lung on both coronal (17.60 ±4.88) and sagittal scan (19.56 ± 6.65) was higher than axial scan (12.16 ± 3.30) (p=0.000), while no difference between coronal and sagittal scan was found (p=0.719) (Fig.4). Mean scan time was 452 s (383–511 s) for axial scan, 372 s (453–508 s) for coronal scan, and 366 s (314 - 454) for sagittal scan.Discussion and conclusion
The overall image quality of whole lung ZTE was good to excellent. Bronchi and pulmonary vessels can be well visualized in most cases, while fissures showed poor demonstration. Coronal or sagittal scan can provide identical image quality, higher SNR and less scan time than axial scan. In addition, ZTE has great potential in revealing rare abnormalities as one volunteer with azygos fissure. In conclusion, 3D isotropic high-resolution lung MRI based on free-breathing ZTE technique is feasible and sufficient to serve as an alternative option for chest imaging with diagnostic image quality and spatial resolution.Acknowledgements
No acknowledgement found.References
1. Biederer J, Mirsadraee S, Beer M, et al. MRI of the lung (3/3)-current applications and future perspectives. Insights Imaging. 2012;3(4):373-86
2. Sodhi KS, Sharma M, Lee EY, et al. Diagnostic Utility of 3T Lung MRI in Children with Interstitial Lung Disease: A Prospective Pilot Study. Acad Radiol. 2018;25(3):380-386.
3.Bae K, Jeon KN, Hwang MJ, et al. Comparison of lung imaging using three-dimensional ultrashort echo time and zero echo time sequences: preliminary study. Eur Radiol. 2019;29(5):2253-2262.
Figures