3221
Same-session Repeatability of Hyperpolarized 129Xe MRI Gas Uptake Measures in Healthy Subjects and Subjects with COPD
William J Garrison1, G Wilson Miller1,2, Kun Qing2, Y Michael Shim3, Jaime F Mata2, Mu He3, Talissa A Altes4, Joanne M Cassani4, Sarah E Struchen2, Roselove N Nunoo-Asare2, Nicholas J Tustison2, Alan M Ropp2, and John P Mugler III1,2
1Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2Radiology and Medical Imaging, University of Virginia, Charlottesville, VA, United States, 3Medicine, University of Virginia, Charlottesville, VA, United States, 4Radiology, University of Missouri, Columbia, MO, United States
1Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2Radiology and Medical Imaging, University of Virginia, Charlottesville, VA, United States, 3Medicine, University of Virginia, Charlottesville, VA, United States, 4Radiology, University of Missouri, Columbia, MO, United States
Synopsis
Same-session repeatability of quantitative measures of gas uptake derived from MRI of inhaled hyperpolarized 129Xe was assessed in healthy and COPD subjects, as well as the impact of scan-to-scan lung volume differences on measured gas uptake. Strong tissue-to-gas and RBC-to-tissue repeatability was found in same-day dissolved-phase 129Xe MRI scans performed at one-third of forced vital capacity, and regressing out scan-to-scan lung volume changes improved repeatability further. COPD subjects displayed similar or better repeatability when compared with healthy subjects.
Introduction
MRI of inhaled hyperpolarized 129Xe can be used to derive quantitative measures of gas uptake, and demonstrates high sensitivity to changes in lung function associated with diseases such as COPD.1-3 Given increasing interest in using this technique to aid clinical characterization of pulmonary diseases, it is important to characterize measurement repeatability in order to establish a threshold beyond which between-subject differences can reasonably be claimed to occur as a result of true physiological differences, rather than as a result of noise and/or error inherent in the measurement.To date, repeatability of RBC-to-gas, tissue-to-gas, and RBC-to-tissue derived from 129Xe MR imaging has been characterized in healthy subjects and subjects with COPD scanned on separate days,4,5 and repeatability of spectroscopic measurements of the RBC-to-tissue ratio has been characterized in healthy subjects and subjects with IPF scanned in the same session and in separate sessions.6,7 Here we assess repeatability of RBC-to-gas, tissue-to-gas, and RBC-to-tissue in healthy subjects and subjects with COPD in the same session, which should set a lower bound for measurement repeatability compared to, for example, measurements performed on different days. We further assess the impact of adjusting gas uptake measures based on scan-to-scan lung volume differences.4,8
Methods
For this study, 32 subjects were scanned between March 2014 and December 2015, with four subjects excluded from analysis due to technical failure. A total of 28 subjects were included in the final analysis, including 17 healthy subjects (age 46-79, %-pred-FEV1 106%±15%, FEV1/FVC 0.77±0.03) and 11 subjects with COPD (GOLD stages 1-3, age 57-80, %-pred-FEV1 63%±23%, FEV1/FVC 0.55±0.13). MR studies were performed using a 1.5T scanner (Siemens Avanto), with a flexible 129Xe chest RF coil (Clinical MR Solutions). Enriched xenon gas (87% 129Xe) was polarized using a prototype commercial system (XeBox-E10, Xemed). Each subject received two identical scans at one-third of forced vital capacity (1/3 FVC, based on spirometry) within a single imaging session. For each scan, dissolved-phase 129Xe1 and proton acquisitions were performed in a single breath-hold as previously described.8 Gas-uptake measures were calculated from each 129Xe acquisition using an IDEAL fitting algorithm, and within-scan lung volumes were determined by segmenting proton lung images using a neural network-based toolbox.9 The following measures of repeatability were applied to whole-lung means: two-way random, single-measure, absolute-agreement intraclass correlation coefficient (ICC); coefficient of variation (CV); and coefficient of repeatability (CR). Volume-adjusted repeatability was assessed by adjusting the second measurement in each subject to account for scan-to-scan changes in lung volume based on scan-to-scan percentage changes in lung volume and gas ratio, and calculating ICC, CV, and CR after performing this adjustment.Results
Fig. 1 depicts the first and second gas uptake measurements in each individual subject, while Fig. 2 depicts the first and second lung volume measurements; Figs. 1 and 2 each list corresponding ICC, CV, and CR results for the healthy and COPD groups. Fig. 3 depicts fits of percent scan-to-scan changes in gas uptake measures vs. percent changes in lung volume, produced in the manner shown in Hahn et al.4 Fig. 4 depicts volume-adjusted repeatability results.Discussion
Repeatability of tissue-to-gas and RBC-to-tissue was greater than repeatability of RBC-to-gas in these subjects, in general agreement with previous results.5 It is possible that tissue-to-gas repeatability was greater than RBC-to-gas repeatability in these subjects as a result of the higher tissue signal, assuming that the noise amplitudes were similar across the two measures. RBC-to-tissue repeatability seems to exceed RBC-to-gas repeatability in part because tissue-to-gas and RBC-to-gas tended to vary concurrently with one another between scans within a subject, thereby minimizing RBC-to-tissue variability. Across all three gas uptake measures and for all three measures of repeatability, subjects with COPD displayed better repeatability than healthy subjects.Within-scan lung volume was highly repeatable in the population studied, as shown in Fig. 2. Accordingly, it seems sensible that adjusting gas uptake results from the second measurement based on scan-to-scan changes in lung volume based on the fit shown in Fig. 3 would produce some benefit to repeatability, but would not erase the bulk of scan-to-scan variation in gas uptake measures. This is borne out by the results shown in Fig. 4: repeatability measures improved in the subject sample after adjustment for lung volume, but noteworthy scan-to-scan variation remained in many subjects even after lung volume-based correction, indicating significant contribution to variability by noise or other hitherto-uninvestigated confounds. Relationships between scan-to-scan changes in gas uptake measures and lung volume in healthy subjects resembled previous findings.4 COPD subjects generally exhibited similar behavior to healthy subjects; there was a noteworthy difference in slope between the two groups, but it is possible that this was a product of the relatively small number of subjects and/or weak linearity in the COPD data.
Conclusion
Strong tissue-to-gas and RBC-to-tissue repeatability was found in same-day dissolved-phase 129Xe MRI of healthy subjects and subjects with COPD. Relationships of gas uptake measures to within-scan lung volume were similar to those previously observed, and regressing out scan-to-scan lung volume changes produced further improvements to repeatability, indicating that lung volume changes were an important source of scan-to-scan gas uptake variation.Acknowledgements
Research reported in this abstract was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number R01 HL109618.References
- Qing K, Mugler JP, Altes TA, et al. Assessment of lung function in asthma and COPD using hyperpolarized 129Xe chemical shift saturation recovery spectroscopy and dissolved-phase MRI. NMR Biomed. 2014;27:1490–1501.
- Qing K, Tustison NJ, Mugler JP, et al. Probing changes in lung physiology in COPD using CT, perfusion MRI, and hyperpolarized xenon-129 MRI. Acad Radiol. 2019;26(3):326–334.
- Myc L, Qing K, He M, et al. Characterisation of gas exchange in COPD with dissolved-phase hyperpolarised xenon-129 MRI. Thorax. 2020;thoraxjnl-2020-214924.
- Hahn AD, Kammerman J, Evans M, et al. Repeatability of regional pulmonary functional metrics of hyperpolarized 129Xe dissolved phase MRI. J Magn Reson Imaging. 2019;50(4):1182–1190.
- Kern AL, Gutberlet M, Qing K, et al. Regional investigation of lung function and microstructure parameters by localized 129Xe chemical shift saturation recovery and dissolved‐phase imaging: a reproducibility study. Magn Reson Med. 2019;81:13–24.
- Kaushik SS, Freeman MS, Yoon SW, et al. Measuring diffusion limitation with a perfusion-limited gas - hyperpolarized 129Xe gas-transfer spectroscopy in patients with idiopathic pulmonary fibrosis. J Appl Physiol (1985). 2014;117(6):577–585.
- Weatherley ND, Stewart NJ, Chan H, et al. Hyperpolarised xenon magnetic resonance spectroscopy for the longitudinal assessment of changes in gas diffusion in IPF. Thorax. 2019;74(5):500–502.
- Qing K, Tustison NJ, Altes TA, et al. Gas uptake measures on hyperpolarized xenon-129 MRI are inversely proportional to lung inflation level. ISMRM 23rd Annual Meeting and Exhibition. 2015;1488.
- Tustison NJ, Avants BB, Lin Z, et al. Convolutional neural networks with template-based data augmentation for functional lung image quantification. Acad. Radiol. 2019;26(3):412–423.
Figures
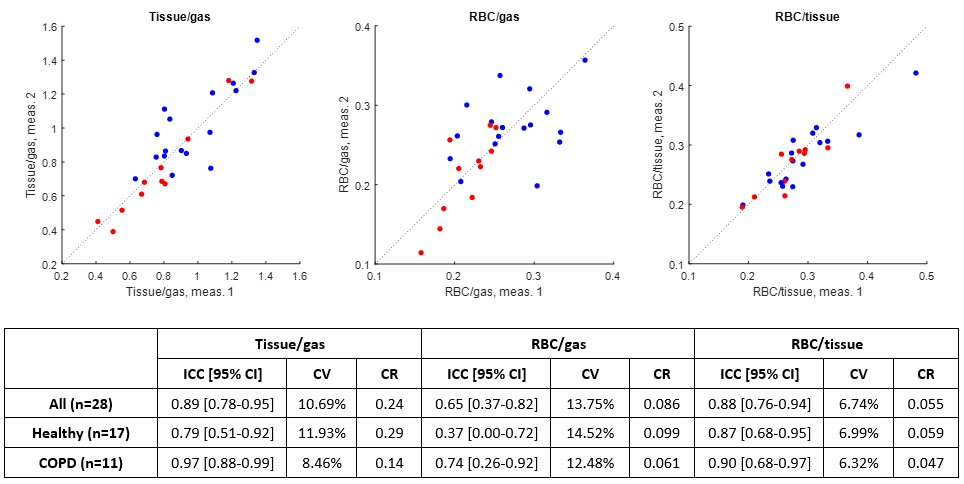
Fig. 1. Second measurements vs. first measurements of tissue-to-gas, RBC-to-gas, and RBC-to-tissue, in healthy subjects (blue) and in COPD subjects (red), as well as intraclass correlation coefficient (ICC), coefficient of variation (CV), and coefficient of repeatability (CR) for each of the three gas uptake measures.
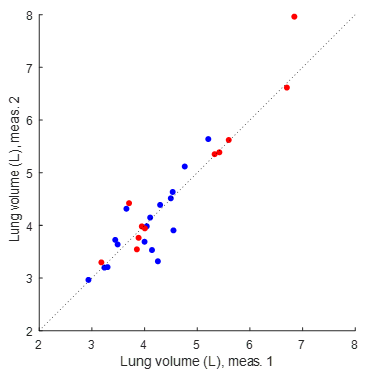
Fig. 2. Second
measurement vs. first measurement of within-scan lung volume. For all subjects,
ICC = 0.93 (n = 28, 95% confidence interval: [0.85 – 0.97]). For healthy
subjects, ICC = 0.82 (n = 17, 95% confidence interval: [0.58 – 0.93]).
For COPD subjects, ICC = 0.95 (n = 11, 95% confidence interval: [0.84 –
0.99]).
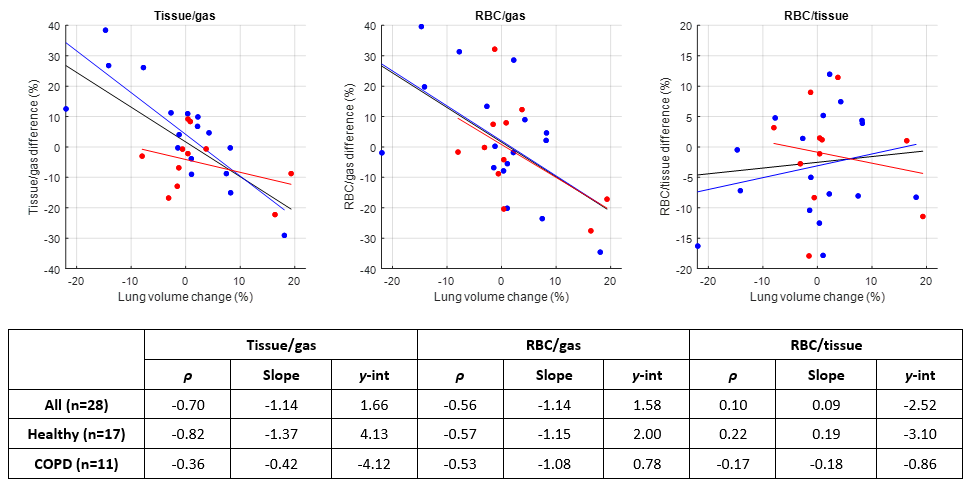
Fig. 3. Percent change in gas uptake ratios vs. percent
change in lung volume, for healthy subjects (blue) and COPD subjects (red),
with linear fits to all subjects (black line), healthy subjects (blue line),
and COPD subjects (red line), as well as correlation coefficients ρ,
slopes, and y-intercepts for each of the fits.
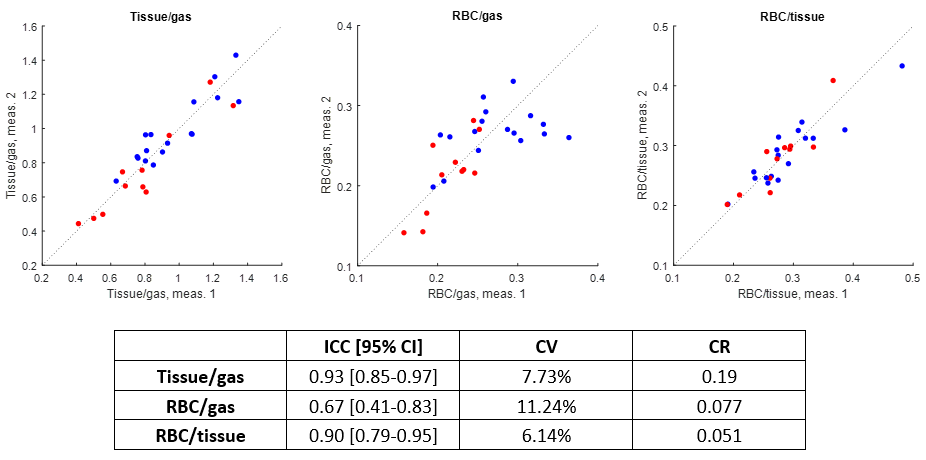
Fig. 4. Adjusted second vs. first measurements of the gas
uptake measures in healthy subjects (blue) and in COPD subjects (red), after
correcting all subjects using the fit of gas ratio vs. lung volume for all
subjects. Resulting intraclass correlation coefficient (ICC), coefficient of
variation (CV), and coefficient of repeatability (CR) for each of the three gas
uptake measures are also shown.