3219
Assessment of dynamic thoracic motion for pre and post-surgical assessment using xt-PCA1Medical Physics, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, 2Department of Radiology, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, 3Medical Physics, King's College Hospital NHS Foundation Trust, London, United Kingdom, 4Department of Thoracic Surgery, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom
Synopsis
Despite recent advances in surgical techniques, postoperative complications arise in 24-41% of patients undergoing thoracic surgery. Here we present an MRI protocol for the pre and postoperative assessment of chest wall and diaphragmatic motion which provides valuable dynamic information to aid radiological assessment in these highly variable patients. We also propose a novel method for fully automated extraction of the diaphragm motion which can provide an additional tool to aid radiologists in making the distinction between expected and adverse postoperative pathologies.
Introduction
Despite recent advances in surgical techniques, postoperative complications arise in 24-41% of patients undergoing thoracic surgery.[1] Consequently, such interventions require careful planning. Specifically, pre-surgical diaphragmatic palsy or chest wall motion abnormalities, associated or not with other lung pathology, need careful assessment. Similarly, post-surgical functional complications such as impaired diaphragmatic movements or reduced chest wall motility can have a high impact on patients’ quality of life and recovery.Radiological assessment is key in these patients. Chest radiographs are the primary and most frequently used tool for thoracic assessment. However, the static and planar nature of these images makes them unsuitable to detect diaphragmatic and chest wall functional abnormalities [1]. Local clinical practice is to use ultrasound for assessing thoracic mobility in pre and post-operative patients, as this has the advantage of real-time imaging and wide availability. Nevertheless, it is limited by a narrow FOV and strong intra-operator variability.
In this abstract, we describe our work to develop an MRI protocol for the assessment of pre and post-operative chest dynamics utilising dynamic time-resolved imaging, incorporating principal component analysis (PCA) and clustering of xt-domain data (xt-PCA) to describe diaphragmatic motion measure.
Methods
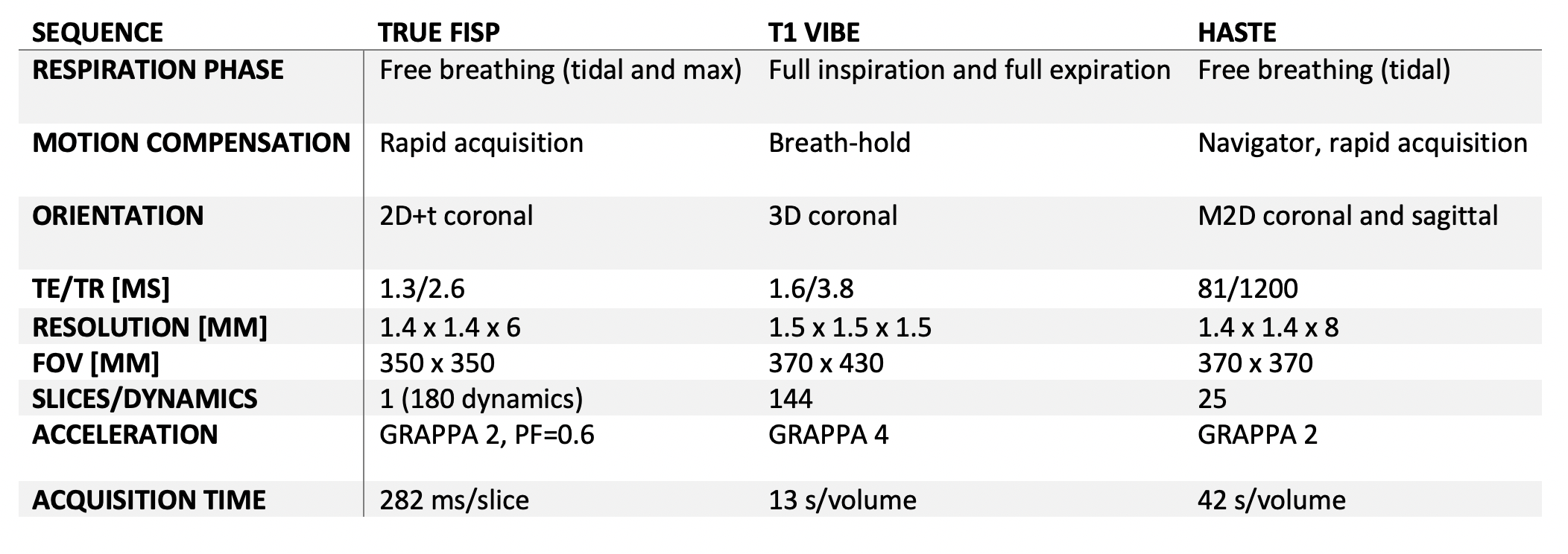
All data were acquired on 1.5T Siemens Aera scanners equipped with 18-channel body and 12-channel spine receive arrays. The protocol was initially performed on 3 healthy volunteers and 3 patients. One of the latter had right diaphragmatic palsy and needed pre-operative assessment; two were assessment of complication after thoracic surgery for lung cancer with robotic plication and chest wall reconstruction. The dynamic imaging protocol consisted of a coronal 2D+t True FISP cine, T1 weighted VIBE and T2 HASTE acquisitions (Table 1).For analysis of True FISP cine images, a fully-automated xt-PCA respiratory signal extraction method was developed. The software was developed in python and within the specifications of a local framework that facilitates integration with PACS. The objective of this processing was to extract a motion signal that describes the diaphragmatic function. For this purpose, we utilise a combination of PCA and signal clustering to extract the dominant motion signal (Figure 1).
First, the data was transposed into xt space along the super-inferior direction. PCA was then performed for every xty projection where y indicates the left-right index of the projection within the slice. From this xt-space, 3 principal components were extracted [2]. The components of all projections were passed to a modified coil clustering algorithm to extract the dominant motion signal [3]. In the original coil clustering method, the cross-correlation of each RF coil element is analysed and singular value decomposition used to extract a low-rank approximation of the motion signal. Here we take advantage of the fact that those coil elements represent unique views of the motion signal and other views can be substituted. In this case, the views of this signal are the individual principal components of the xt projections.
Results
Example images acquired using this protocol are shown in Figure 2. In this case, the data were acquired in a patient who had undergone successful left upper lobectomy with chest wall reconstruction. The motion resolved images enabled the reporting radiologist to assess chest wall and diaphragm excursion while the static images provide high-resolution T2-weighted images for assessment of focal lung or pleural pathology.Figure 3 shows representative signals produced with the xt-PCA analysis. The diaphragm signals extracted using the xt-PCA are semi-quantitative but can provide patient-specific measures of tidal function, as well as indicators of the inspiratory and expiratory reserve.
The temporospatial information of the xt-PCA analysis enables the diaphragm motion to be examined in each lung individually. In figure 4, the extracted signals for each lung in a healthy volunteer have similar amplitudes, whereas, in a patient with right diaphragmatic palsy, we see a much smaller signal produced in the right lung relative to the left indicating reduced right diaphragm mobility and compensatory increased excursion of the left diaphragm. In this case, the valuable metric that indicates impaired lung function is the intrapatient difference of right/left signals.
Discussion
The interpretation of postoperative images can be complex, as the reporting radiologist will have to differentiate ‘expected’ post-surgical alterations to normal physiology from real pathological alterations.[4] The fully automatic extraction of the diaphragm motion signal using the methods described here may provide an additional tool to aid radiologists in making this distinction.Other than qualitative visual assessment, key metrics used for assessment of diaphragmatic motion in patients include tidal volume, expiratory reserve and inspiratory reserve. However, these metrics require large 4D volume acquisitions that can be difficult to achieve due to the requirement for long acquisitions with strict gating strategies that may not be effective in patients with reduced lung function. The xt-PCA signals produced here enable a method for semi-quantitative intra-patient assessment of these key metrics. As can be seen in figures 3 and 4, the magnitude of the xt-PCA diaphragm signal is not indicative of lung function or volume.
The protocol described here has been deployed clinically and initial results have been promising. Planned continuation of this trial with larger patient populations will determine whether the MRI protocol and xt-PCA analysis can improve the quality of patient care.
Acknowledgements
No acknowledgement found.References
[1] Cicchetti, Giuseppe, et al. "Imaging of postsurgical complications occurring after thoracic surgery: review of the main surgical procedures and early and late complications." European Congress of Radiology 2017, 2017.
[2] Pang, Jianing, et al. "ECG and navigator‐free four‐dimensional whole‐heart coronary MRA for simultaneous visualization of cardiac anatomy and function." Magnetic resonance in medicine 72.5 (2014): 1208-1217.
[3] Zhang, Tao, et al. "Robust self‐navigated body MRI using dense coil arrays." Magnetic resonance in medicine 76.1 (2016): 197-205.
[4] Bommart, S., et al. "Imaging of postoperative complications following surgery for lung cancer." Diagnostic and interventional imaging 98.1 (2017): 11-20.
Figures