3210
Using GRASP-DCE MRI for the Identification of Subtypes of Lung Cancers from Benign Lung Lesions.1Zhongda Hospital, Medical School of Southeast University, Nanjing, China, 2SIEMENS Healcare, Shanghai, China
Synopsis
This study is expected to provide information about differentiating of benign from malignant pulmonary lesions with free-breathing Golden-angle RAdial Sparse Parallel (GRASP)-DCE MRI among 33 lung lesions. The results initially indicated that the quantitative DCE parameter maps calculated by GRASP-DCE MR could be a clinical useful technique for lung lesions detection.
Introduction
MRI is a useful tool for lung tumor detection, because it can provide multiple contrast in arbitrary orientation without the release of radiation. For lung tumors, conventional contrast-enhance T1W MRI requires patients hold breath for around 20 second at least twice before and after the injection of contrast agent, which makes the quantification of DCE perfusion impossible due to the long acquisition (longer than 5 min) in upper abdomen area. A recent approach, Golden-angle RAdial Sparse Parallel (GRASP)-DCE MRI, was proposed for DCE or CE MRI in moving organs (1). Such technique employs golden angle radial trajectory in k-space for data acquisition, which is insensitive to motion arised from the patients, and compress sensing algorithm for image reconstruction, which allows for high temporal and spatial resolution. It is already reported that GRASP can be performed under free breathing condition (2). The purpose of this study is to analysis the correlation between the quantitative parameters obtained from GRASP DCE between benign and different types of malignant lung tumors.Methods
A total number of 32 patients (33 lesions) were included in this study, and all the patients were divided into 4 groups, which are Adenocarcinoma, Squamous carcinoma, SCLC and benign lesions, according to the pathological results. All MR exams were performed on a 3 T MRI scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) with a 18-channel body coil. The conventional axial T1WI and coronal and axial TSE T2W images were acquired before contrast injection. Dynamic contrast-enhanced MR data were acquired using GRASP during free breathing, and reconstructed with a temporal resolution of 2.9 sec/phase for the first 26 periods and 7.6 sec/phase for the left 30 periods). The detailed protocol were: TR/TE=2.9/1.28ms, FOV=400x400mm2, spatial resolution=1.4x1.4mm2, slice thickness=3mm, number of slice=80, total number of spokes=1519, total acquisition time=5min40se. For post processing, the quantitative perfusion analysis was performed using a standard Tofts model (Tissue4D, Siemens Healthcare, Erlangen, Germany) to generate the volume transfer coefficient (Ktrans,min-1) , rate constant between extracellular/extravascular space (EES) (Kep,min-1), the interstitial volume (Ve,ml/ml).Pearson correlation coefficients were calculated to evaluate the repeatability in the perfusion measurements. The one-way analysis of variance (ANOVA) followed by the least significant difference (LSD)-t method of multiple comparisons were used to compare the quantitative perfusion results across different histologic types.Results
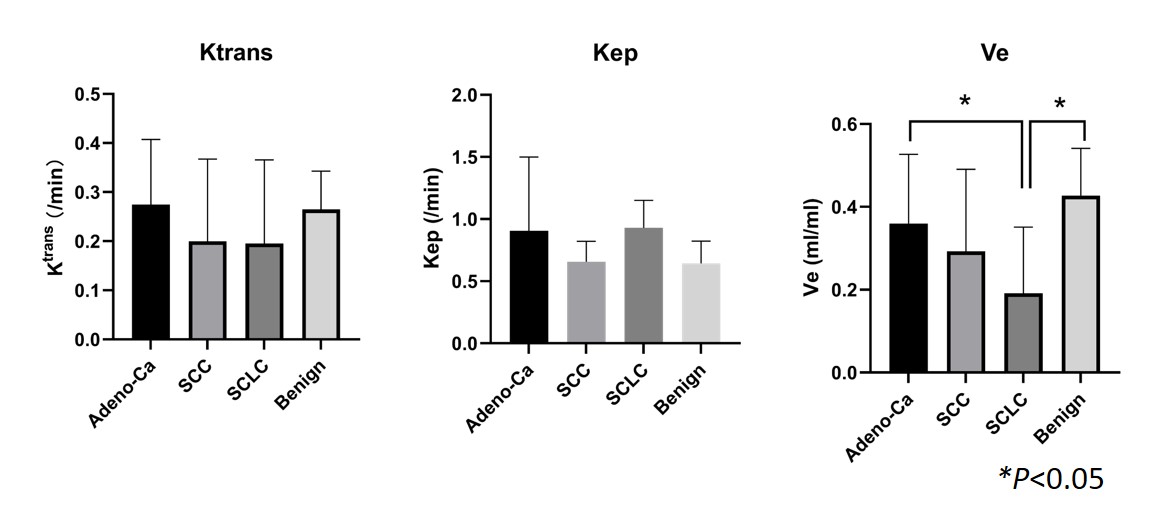
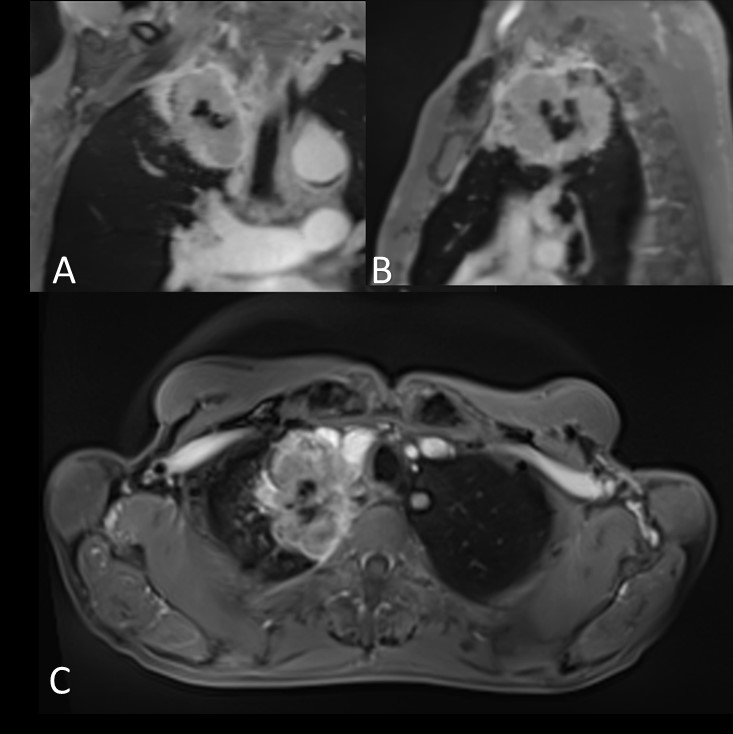
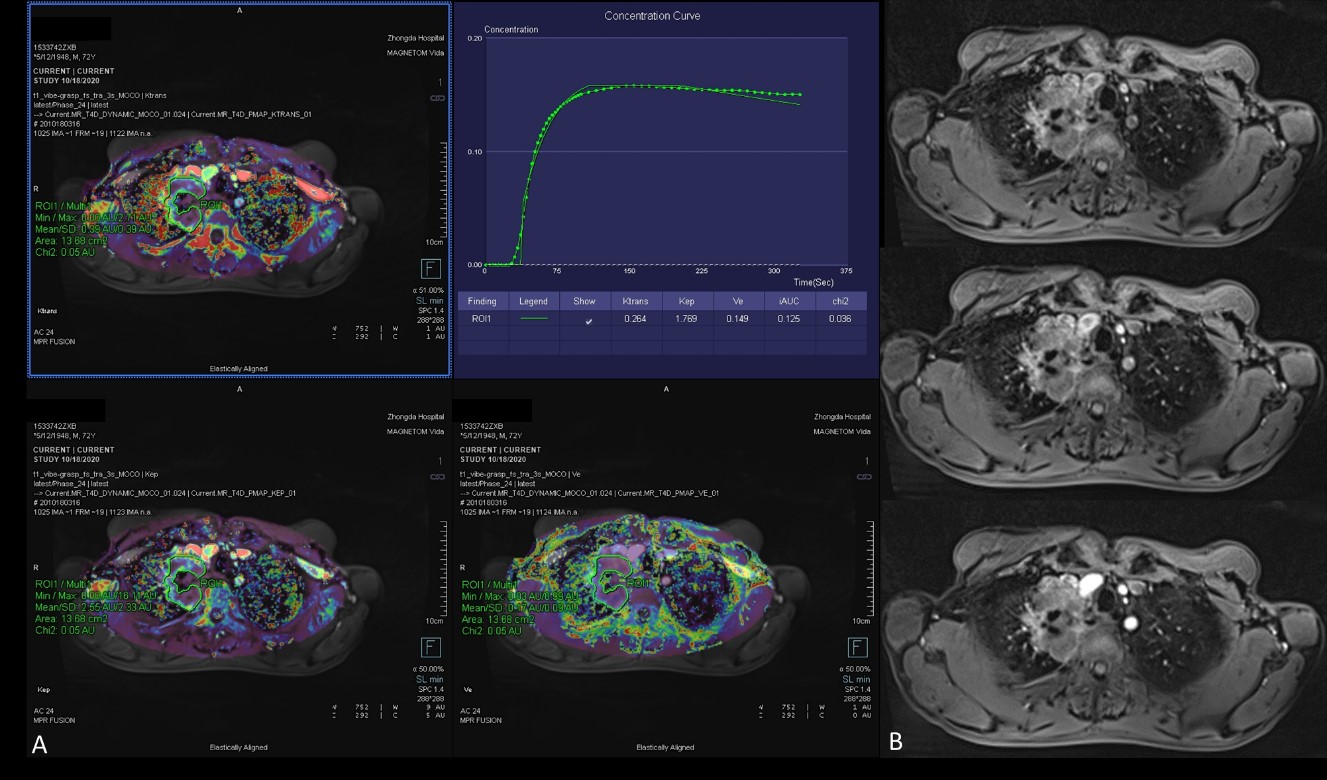
There were 32 patients (10 females, mean age, 64.6 years, years range from 42-80) enrolled in the present study with 4 benign SPL and 29 LCs: 6 small cell carcinomas (SCLC), 7 squamous cell carcinomas (SCC), and 16 adenocarcinomas (Adeno-Ca). For all the calculated DCE maps, Ve enjoys the best performance in distinguishing benign and malignant lung tumors. To be more specific, for the group of Adeno-Ca and benign lesions, Ve values (0.36±0.167 and 0.428±0.114, respectively) was significantly higher than that of the SCLC group (0.192±0.160) (seen in Figure 1). The post-contrast images and calculated DCE maps of a representative patient were illustrated in Figure 2&3.Discussion & Conclusions
This study successfully performed free breathing DCE acquisition for all the patients with lung tumors. The combination of golden angle radial trajectory in k-space and compress sensing reconstructions can provide high special and temporal resolutions for DCE MRI. The results indicated that DCE-derived Ve is a promising parameter for differentiating LC from benignity.Acknowledgements
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. This prospective study was approved by the Institutional Review Board (NO:2020ZDSYLL178-P01).No study subjects or cohorts have been previously reported.References
1. Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine. 2014; 72(3):707–717.
2. Lihua C, Xianchun Z, Youli W, et al. A Study of the Correlation of Perfusion Parameters in High-Resolution GRASP MRI With Microvascular Density in Lung Cancer. Journal of Magnetic Resonance Imaging. 2018; 49(4): 1186–1194.
3. Kim, J. Y., Kim, S. H., Kim, Y., et al. Enhancement parameters on dynamic contrast enhanced breast MRI: Do they correlate with prognostic factors and subtypes of breast cancers? Journal of Magnetic Resonance Imaging. 2015;33(1):72–80.
Figures