3204
Diffusion Kurtosis Imaging and Intravoxel Incoherent Motion in diagnosis of active sacroiliitis with ankylosing spondylitis1Medical Imaging, Shanxi Medical University, Taiyuan, China, 2Department of Radiology, Shanxi Bethune Hospital, Taiyuan, China, 3MR Scientific Marketing, Diagnosis Imaging, Siemens Healthineers China, Beijing, China, 4MR Scientific Marketing, Diagnosis Imaging, Siemens Healthineers China, Shanghai, China
Synopsis
Advanced DWI techniques, diffusion kurtosis imaging (DKI) and intravoxel incoherent motion (IVIM), can complement physiological information to morphological information that was obtained with conventional MRI This study investigated the application of DKI and IVIM in diagnosis of active sacroiliitis with ankylosing spondylitis.
Synopsis
Advanced DWI techniques, diffusion kurtosis imaging (DKI) and intravoxel incoherent motion (IVIM), can complement physiological information to morphological information that was obtained with conventional MRI This study investigated the application of DKI and IVIM in diagnosis of active sacroiliitis with ankylosing spondylitis.Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease with unclear etiology of sacroiliitis and spondylitis, which is characterized as persistently alternations between the active and the chronic stage [1]. The progression of AS is closely related to hla-27, tumor necrosis factor and interleukin-17 [2]. At present, the treatment of AS is based on anti-tumor necrosis factor - α (TNF - α), therefore, the staging of inflammation of AS is important in clinical practice [3]. Clinical assessment of AS is as erythrocyte sedimentation rate (ESR) and Creactive protein (CRP), while study have shown that up to 40% of patients with AS in active stage did not show increased CRP or ESR [5]. MRI is a sensitive and noninvasive imaging method that can detect the activity in sacroiliitis with As, and advanced diffusion models, such as DKI and IVIM, can be used as an effective tool for diagnosing the activity of AS, especially in monitoring AS therapy [1]. This study evaluated the diagnosis value of DKI and IVIM in distinguish active or stable stage of sacroiliitis with ankylosing spondylitis.Methods
In total, 43 patients (average age 30.93 ± 9.533 years, 31 males, 12 females) with AS were enrolled in this study and divided into active group (23 cases) and chronic group (20 cases). The criteria of clinical and laboratory tests to determine the active and chronic group were as follows: for the active group, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) average score≥6 or between 4.0 and 6.0 with ESR≥20 mm/h or CRP≥3 mg/L; for the chronic group BASDAI average score < 4.0 or between 4.0 and 6.0 with ESR <20mm/h or CRP≤3mg/h. All patients underwent MRI scan on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) using 32-channel body coil with abdominal strap. Coronal T1WI-TSE and T2WI-fs images of bilateral sacroiliac joints were acquired. The diffusion imaging based on single shot echo planar imaging (SE-EPI) was obtained with 3 scan trace mode, with 10 b values (0, 50, 100,150,200,300,600,900,1200, 1500 mm2/s). The sequence parameters were as follows: TR= 3910ms, TE= 71ms, PAT= 2, FOV= 320 × 320mm2, matrix= 128 × 128; slice thickness:3mm. The parameters derived from DKI and IVIM were calculated by a prototype software (Siemens Healthcare, Erlangen, Germany), including Mean Diffusion (MD) and Mean Kurtosis (MK), and IVIM parameters includes Pure diffusion (D), Pseudo diffusion coefficient (D*) and Perfusion fraction(f). For each patient, the maximum cross-sectional area of lesion was manually drawn on each of DKI and IVIM metric maps as the region of interest (ROI) by visual inspection according to T2WI-fs and B=600mm2/s diffusion images, which were more than 1 mm away from the edge of the lesions, avoided blood vessels, bone cortex, bone destruction area, cystic change area and sclerotic area. Differences in all diffusion parameters between active stage and chronic stage were compared using the independent sample t test, and the diagnostic effectiveness was evaluated by receiver operating characteristic (ROC) curve analysis.Results
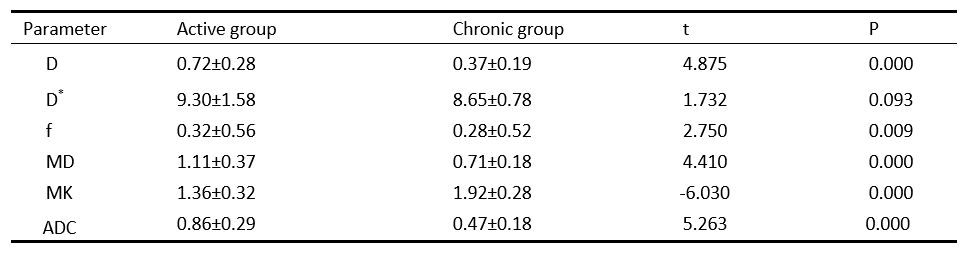
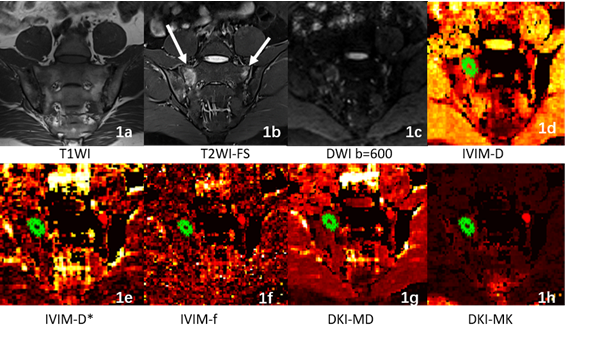
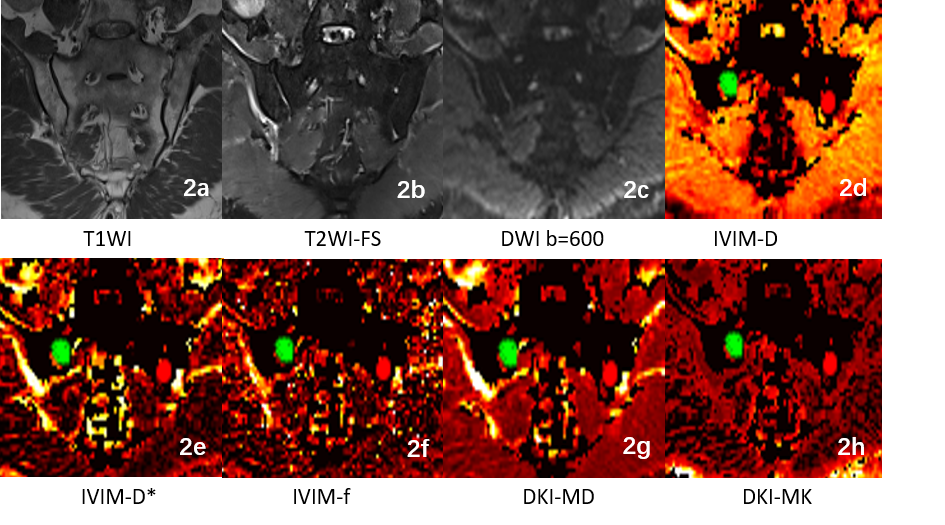
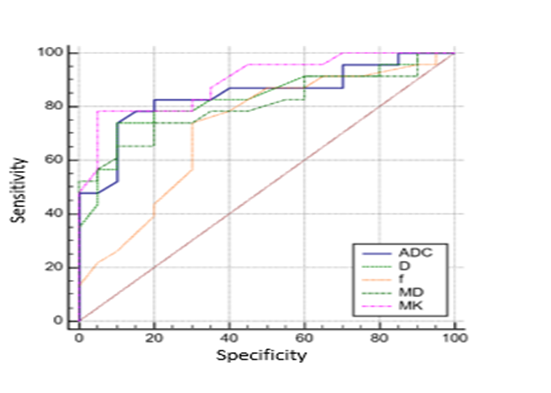
As shown in Table 1, between active group and chronic group, significant differences was observed in DWI-ADC, DKI-based MD and MK, and IVIM-based D and f(p<0.05). One representative case is shown in Figure 1 and Figure 2. Figure 3 and Table 2 demonstrated that the AUCs of ADC, DKI-MK, DKI-DK, IVIM-D and IVIM-f were all above 0.7, and the DKI-MK achieved the highest AUC (0.895) and specificity (0.9) in the diagnosis of active sacroiliitis with ankylosing spondylitis.Discussion and Conclusion
Ankylosing spondylarthritis (AS) is a chronic inflammatory disease that involves the axial joints and entheses, and the diagnosis and treatment of active sacroiliitis with ankylosing spondylitis can significantly improve patients’ living quality. Currently, the diagnosis of AS based on CRP and ESR have certain limitation, therefor it is essential to find a noninvasive and sensitive method for early diagnosis. This study applied IVIM and DKI advanced diffusion imaging techniques to quantitively diagnosis the active sacroiliitis with AS. The results show IVIM-DWI and DKI are feasible for diagnosis of SIJ activity of AS. Among these parameters, DKI-MK is the most valuable parameter in differentiation of active or chronic stage of AS.Acknowledgements
None.References
1. Zhao YH,Li SL,Liu ZY,et al.Detection of Active Sacroiliitis with Ankylosing Spondylitis through Intravoxel Incoherent Motion Diffusion-Weighted MR Imaging[J].European Radiology,2015,25(9):2754-2763.
2. Pedersen SJ, Maksymowych WP.The Pathogenesis of Ankylosing Spondylitis: an Update[J].Current Rheumatology Reports,2019,21(10):1-10.
3. Braun J, Baraliakos X, Godolias G, Böhm H (2005) Therapy of ankylosing spondylitis – a review Part I: Conventional medical treatment and surgical therapy. Scand J Rheumatol 34:97–108.
4. Zochling J, Braun J, van der Heijde D (2006) Assessments in ankylosing spondylitis. Best Pract Res Clin Rheumatol 20:521–537.
Figures