3180
Measuring motor unit morphology in upper extremities using motor unit magnetic resonance imaging (MUMRI)1Translational and Clinical Research Unit, Newcastle University, Newcastle upon Tyne, United Kingdom, 2Newcastle Biomedical Research Centre, Newcastle Biomedical Research Centre, Newcastle upon Tyne, United Kingdom, 3Northern Medical Physics and Clinical Engineering, Newcastle upon Tyne NHS Foundation Trust, Newcastle upon Tyne, United Kingdom
Synopsis
Motor unit (MU) magnetic resonance imaging (MUMRI) is a non-invasive technique which detects muscle fibre micro-contraction and is based on diffusion weighted MRI. To date MUMRI has been applied in conjunction with in scanner electrical stimulation to study MU activity in the lower leg. Here we present the first use of MUMRI in the upper limbs to study single human MUs. The acquired images show low levels of distortion and good fat suppression, allowing single human MU sizes and shapes to be determined. This is of interest in neuromuscular diseases as it is a non-invasive way to study MU morphology.
Introduction
A motor unit (MU) comprises a single motor nerve axon and the multiple skeletal muscle fibres that this innervates. Recently we have shown that MU activity can be detected using diffusion weighted magnetic resonance imaging, a technique called “motor unit MRI (MUMRI) [1].We have previously applied MUMRI alongside in-scanner electrical stimulation to study MUs in the lower leg muscles as these are relatively straight-forward to stimulate and image [2]. Neuromuscular disorders can present with onset in upper limb muscles or lower limb muscles [3]. Therefore, to increase the clinical translatability of MUMRI it is essential that it can also be applied to other body regions, for example the upper limb muscles. MRI of the upper limb muscles is more challenging, particularly in patients with neuromuscular disorders as they are often unable to be scanned in the head-first “superman” position and instead the arm is positioned laterally to the body. This off-isocentre placement can lead to increased B0 inhomogeneity image artifacts in diffusion weighted images and poorer fat suppression [4].
Here, we aimed to assess the feasibility of studying MU morphology with MUMRI in the forearm and hand muscles by extracting the size and shape of single motor units in those muscles.
Methods
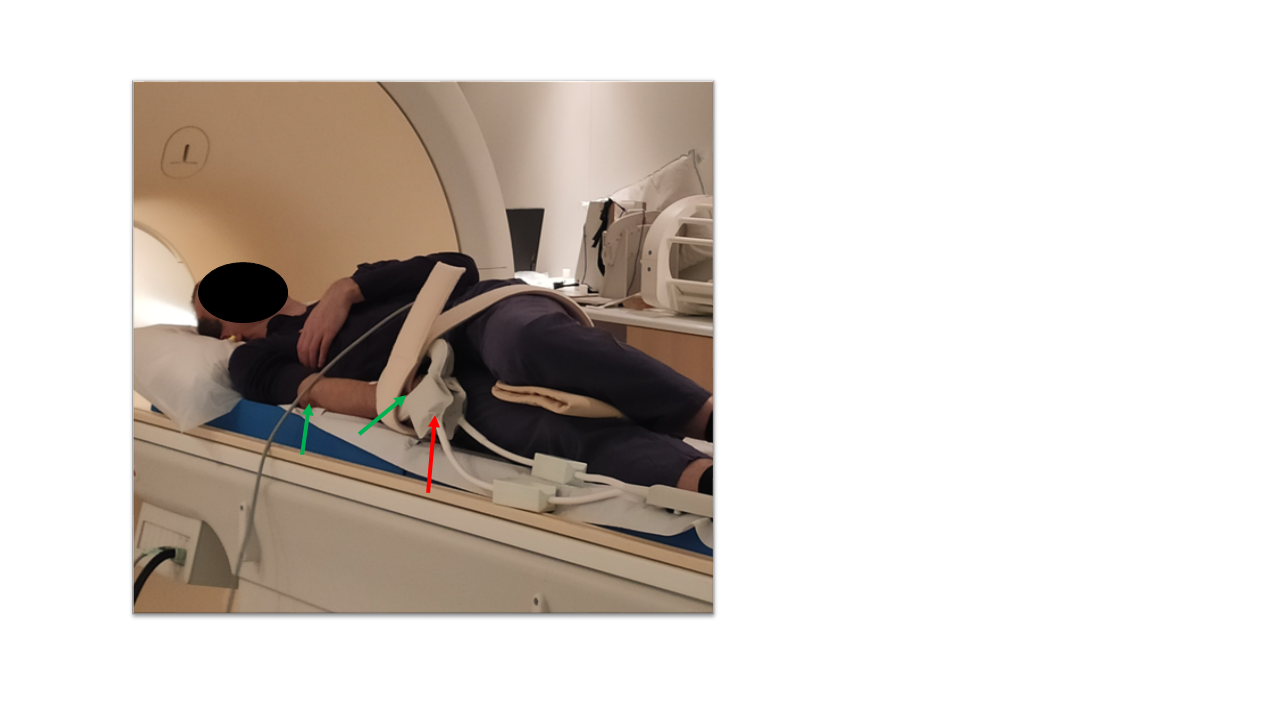
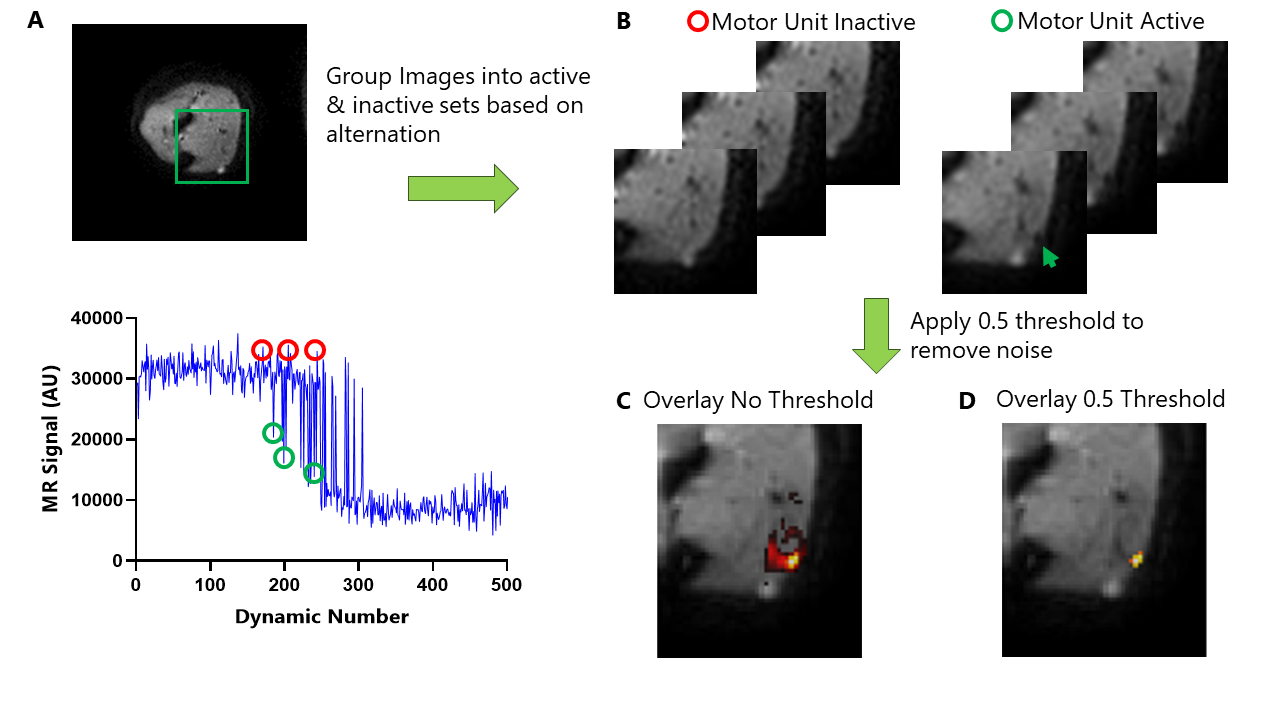
Data-acquisition: Lower arm and hand muscles of two healthy volunteers were scanned using a 3T Philips MR scanner. Volunteers were positioned head-first supine with a pair of FlexM coils wrapped around the forearm or hand (Fig. 1). The right ulnar nerve (forearm) or median nerve (hand) was electrically stimulated with a frequency of 1 Hz, with a bipolar square pulse wave 0.3 ms in duration. DWI images were acquired time-locked to this electrical stimulation (SE-EPI, b = 20s/mm2, voxel size =1.25x1.25x10mm,TR/TE=1000/36ms, Δ/δ=18.2/2.2ms, sensitisation slice direction, fat suppression = SSGR+SPAIR and an additional off resonance inversion pulse to supress olefinic fat). The stimulation protocol consisted of a ramp-down experiment starting at a current causing significant MU activity, and was then decreased in 0.01 mA steps, with each step repeated 5 times, until no signal voids were seen (acquisition time ≈18 minutes).Data-analysis: We created MU activity maps using the MU behaviour called alternation (Fig. 2A/B). At a certain current threshold a motor nerve will fire and the connected muscle fibres will contract in an all or nothing manner. However, as the current strength approaches this threshold, the particular nerve will fire on some occasions, but not on others. This is known as MU alternation. MU activity maps were created by taking the difference between two groups of images - images where the motor unit was firing (presence of a signal void), and where the MU was not firing (no signal void) (Fig 2B). Maps were normalised to the maximal signal intensity and all voxels with a signal intensity smaller than 0.5 were removed (Fig. 2C/D) [2]. The remaining region reflects the MU and its cross sectional area (CSA) and Feret diameters were determined.
Results
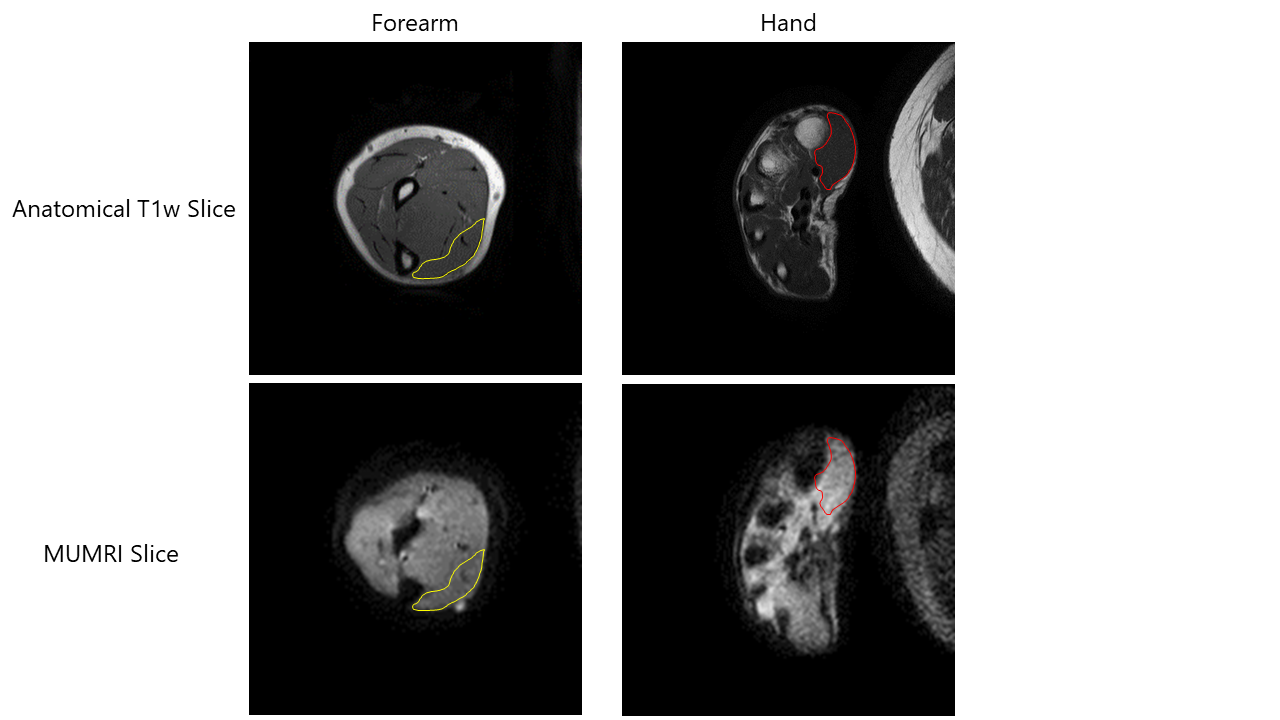
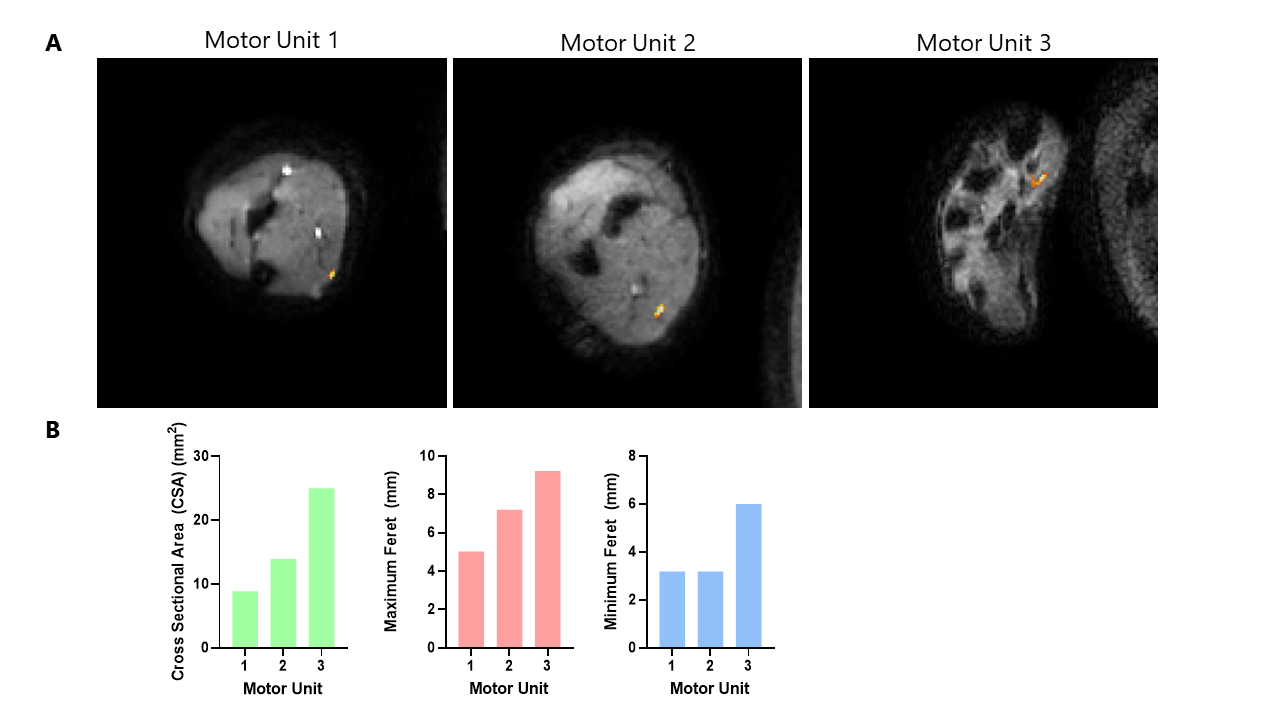
The diffusion scans of the forearm and hand muscles with the arm placed laterally to the side of the body were good quality, appearing to have low distortion and good fat suppression (Fig. 3). We were able to extract three MUs from the DWI data, two from the flexor carpi ulnaris in the forearm and one from the abductor pollis in the hand. The two MUs in the forearm were elliptical in shape and their CSA were 8.9 mm2 and 13.9 mm2, their maximum Feret diameters were 5.0 mm and 7.2 mm and their minimum Feret diameters were 3.2 mm for both (Fig. 4). The MU in the hand was crescent shaped and had a CSA of 25.0 mm2 and maximum and minimum Feret diameter of 9.2 mm and 6.0 mm, respectively (Fig. 4).Discussion
We were able to image single MUs in the forearm and hand muscles. The MU dimensions (CSA and Feret diameters) and shape of these MUs were similar to those described with MUMRI in the lower leg (being average CSA = 26.7±11.2 mm2, average Maximum Feret = 10.7±3.3 mm and average Minimum Feret = 4.5 ± 1.2 mm) [2]. This is also in line with scanning EMG studies, which presented a range of (1.69 – 10.17 mm for the maximum diameter of single MUs in the biceps brachii) [5]. A single MU can be studied in a clinically feasible scan time frame of approximately 30 minutes per muscle group. This means MUMRI can be applied to the upper limbs in conjunction with in-scanner electrical stimulation to elicit MU activity.Conclusions
In this proof of principle work we have demonstrated that MUMRI can be successfully applied to the upper limb muscles and we can image single human MUs and extract the size and shape of them. This increases the clinical translatability of the MUMRI technique. The next steps will be to apply MUMRI in the upper arm muscles and tongue muscles, as these are common muscles for neuromuscular disease onset and difficult muscles to perform invasive techniques in such as needle electromyography. MUMRI could offer a non-invasive alternative to study MU morphology and activity in these muscle groups.Acknowledgements
This work was supported by the Medical Research Council Confidence in Concept (CiC) award [Newcastle University study number 1621/7484/2018]. Rubicon research programme (project number: 452183002) of the Dutch Research Council (NWO) and NIHR Newcastle Biomedical Research Centre. The NIHR Newcastle Biomedical Research Centre (BRC) is a partnership between Newcastle Hospitals NHS Foundation Trust and Newcastle University, funded by the National Institute for Health Research (NIHR). This paper presents independent research funded and supported by the NIHR Newcastle BRC. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social CareReferences
[1] Whittaker R, Porcari P, Braz L, et al. Functional magnetic resonance imaging of human motor unit fasciculation in amyotrophic lateral sclerosis. Annals of Neurology. 2019; 85: 455-9. https://doi.org/10.1002/ana.25422
[2] Birkbeck MG, Heskamp L, Schofield IS, et al. Non-invasive imaging of single human motor units. Clinical Neurophysiology. 2020; 131: 1399-1406. https://doi.org/10.1016/j.clinph.2020.02.004
[3] McDonald CM. Clinical approach to the diagnostic evaluation of hereditary and acquired neuromuscular diseases. Physical Medicine and Rehabilitation Clinics of North America. 2012; 23: 495-563
[4] Johnson D, Stevens KJ, Riley G, et al. Approach to MR Imaging of the Elbow and Wrist: Technical Aspects and Innovation. Magnetic Resonance Imaging Clinics of North America. 2015; 23: 355-366
[5] Stålberg E, Dioszeghy P. Scanning EMG in normal muscle and in neuromuscular disorders. Electroencephalography and clinical Neurophysiology. 1991; 81: 403-416
Figures