3176
Imaging of calf muscle contraction in pediatric patients with cerebral palsy: comparison of voluntary motion and electrically evoked motion1Department of Radiology, Division of Radiological Physics, University Hospital Basel, Basel, Switzerland, 2Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 3Department of Radiology, Division of Neuroradiology, University Hospital Basel, Basel, Switzerland, 4Laboratory for Movement Analysis, University Children's Hospital Basel, Basel, Switzerland, 5Hugh Williamson Gait Laboratory, The Royal Children's Hospital Melbourne, Parkville, Australia, 6Department of Orthopedic Surgery, University Children's Hospital Basel, Basel, Switzerland
Synopsis
Aim of this study is to investigate the feasibility of phase contrast imaging at 3T for assessment of muscle function in children with cerebral palsy. Time-resolved cine phase contrast MRI was synchronized with (a) electrical muscle stimulation (EMS) of the calf muscle (b) voluntary plantarflexion following visual instructions. The achieved force was higher for the voluntary task, but its periodicity was lower compared to the stimulated contraction. Therefore, it was not possible to resolve two distinct velocity peaks for voluntary contraction and release, but it was during EMS, in case the tolerated current was high enough to evoke sufficient contraction.
Introduction
Cerebral palsy (CP) is a sensorimotor dysfunction caused by damage to the developing brain leading to weakness and spasticity of the affected muscles1. Evoked muscle contraction induced by electrical muscle stimulation (EMS) can be used to study muscle function, measured with a time-resolved phase contrast (PC) MRI method2, but occasionally in patients, especially younger ones, the maximum tolerated current can be too low to evoke sufficiently periodic contractions3. Cine PC MRI has also been applied to assess voluntary leg muscle contraction in adults4,5. However, in CP, there is the challenge that patients cannot always freely control movement of their limbs. We applied both methods in an ongoing clinical study in pediatric patients with CP3 to check the feasibility of a children-suited voluntary exercise.Methods
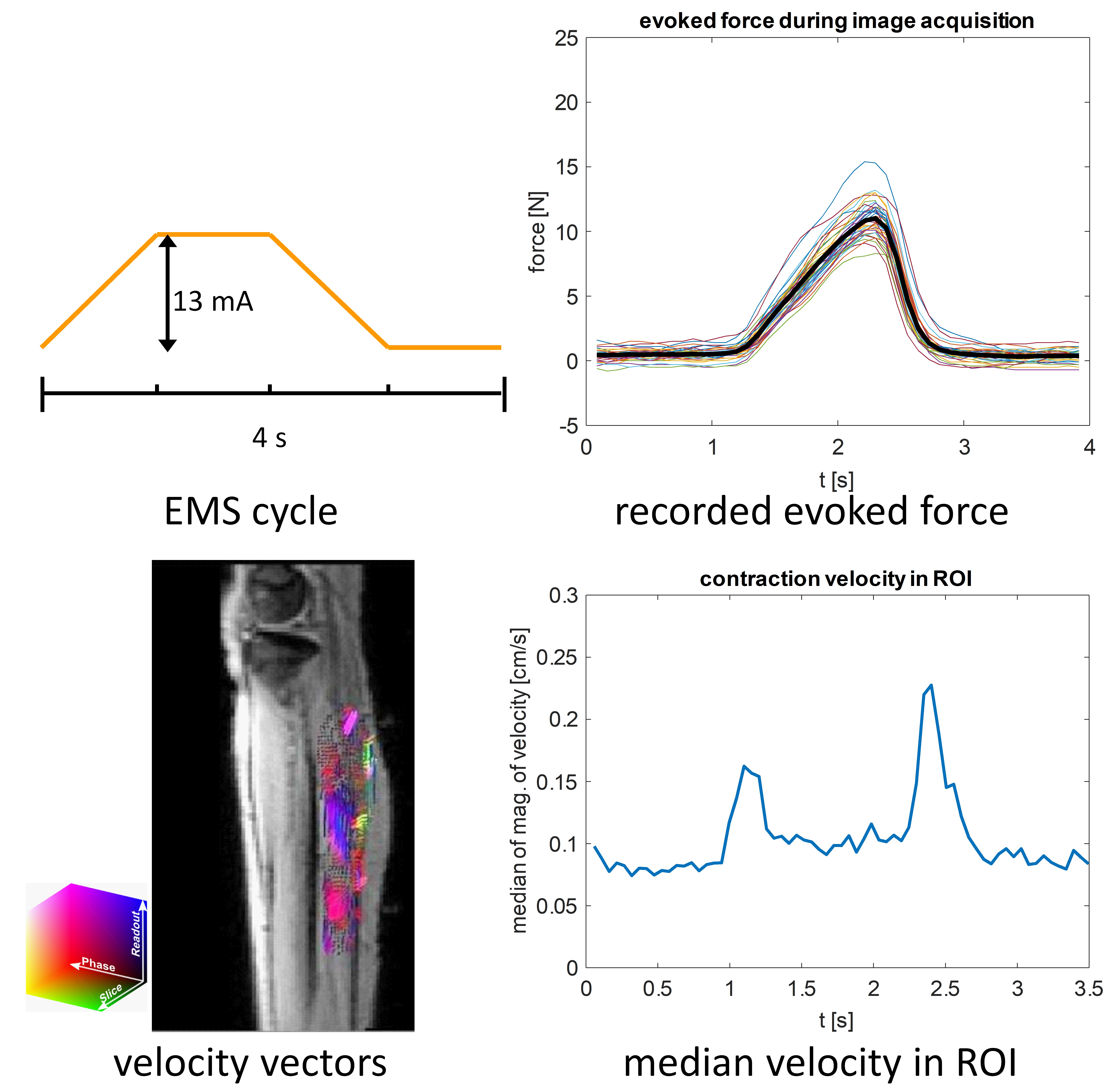
So far, two children with CP were examined. A 14 y girl (diparetic) was scanned twice within 3 months, a 10 y boy (hemiparetic) was scanned once. The triceps surae muscle group of the (more) affected leg was imaged in a 3T whole body clinical MRI scanner. Two experiments (A and B) were performed in one session.(A) For the induction of a periodic contraction, a two-channel commercially-available EMS device with self-adhesive electrodes attached to the muscle belly was used. The maximum voluntary force (MVF) was measured in the scanner before the scan. The evoked force was recorded with a foot pedal device with a built-in force sensor during the scan6,7. The EMS cycle (Fig. 1 top left) had 30 pulses/s and a pulse width of 300 µs. The amplitude of the stimulation current was individually adjusted within the comfort levels (here 8-14 mA) to a point that induced visible force output of at least 5% MVF if possible. A three-directional cine gradient echo PC velocity encoding sequence (1 parasagittal slice, voxels: 2.2x2.2x5.0 mm3, velocity encoding 10 cm/s, echo time 9.7 ms, bandwidth/pixel 400 Hz/px, flip angle 10°, FOV 280x140 mm2, acquisition time 2:28 min, 67 temporal phases, temporal resolution of 52 ms) was synchronized to the EMS cycle.
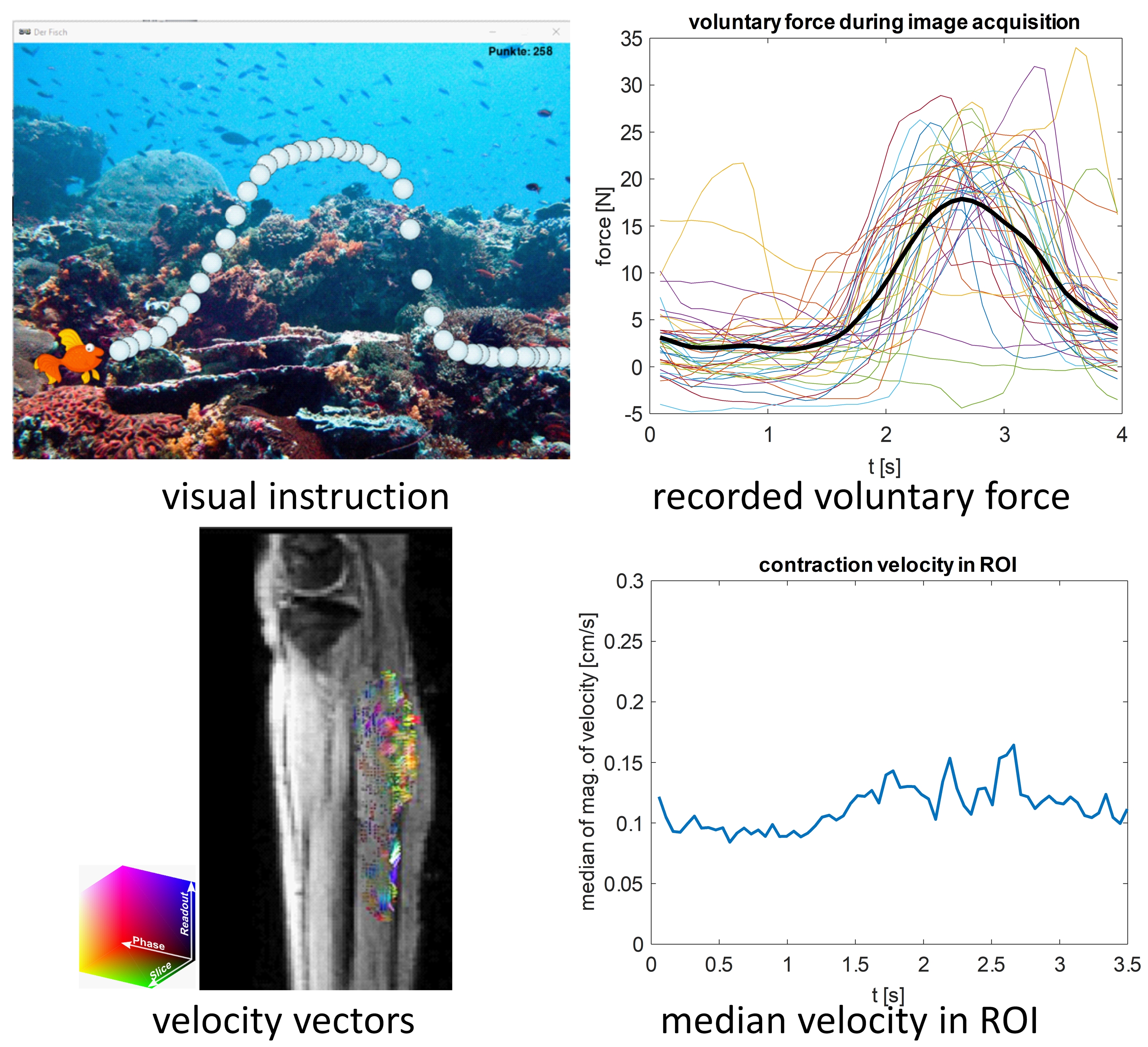
(B) A voluntary exercise paradigm, consisting of a periodic curve with pre-set amplitude (depending on the MVF) and a period of 4 s, was projected on a screen in the scanner room. The shape of the predefined curve was the average of the force time courses of two adult volunteers who previously performed a periodic exercise after a trigger signal in the same set-up. The force generated by the plantarflexion on the pedal was recorded and overlayed in real-time on the predefined curve. In the style of a video game (the fish has to hit as many bubbles as possible, Fig. 2 top left) the patient was supposed to follow the predefined curve by pressing the pedal. After a training period of 5 min the voluntary motion was performed during the scan. The code for the display of the exercise paradigm and the real-time force values were written in Python. The cine PC sequence was applied, with the acquisition synchronized to the default periodic curve, i.e. the acquisition window (3.5 s) started every 4 s in the resting phase.
To visualize the contraction time course, a ROI was drawn on the calf muscles and the velocity vector field was displayed for every temporal phase2. For the velocity time course, the median of the magnitude of the velocity vectors in the ROI was calculated for each phase.
Results
(A) The maximum tolerated stimulation current and the developed force at this current showed a relatively large variability between the two sessions for the girl. Data quality of the velocity vector fields was sufficient in one session for the girl and in the session with the boy. Then, the time course of the contraction speed showed distinctive peaks for contraction and release (Fig. 1), which were considerably below 1 cm/s.(B) The amplitude of the voluntary force (that could be generated by the patients without much effort), was higher than the amplitude of the stimulated force. However, the periodicity was lower (Fig. 2). Therefore, it was not possible to resolve two distinct peaks. Nevertheless, the median velocity during motion was well over the baseline in all three sessions.
Discussion and Conclusion
In this pilot study, the voluntary motion using our paradigm was well tolerated and the children were very motivated. The force output was larger than the one achieved with the maximum tolerated stimulation current, which is promising for detectable contraction velocities. Yet the periodicity over the acquisition time was not sufficient to resolve two distinct velocity peaks for contraction and release. This was achieved with the EMS-paradigm. However, if the tolerated current is too low to evoke a detectable periodic motion then the dynamic MR measurement fails. Our cine PC approach relies on the repeated consistent execution of the motion task, which is problematic in patients with poor coordination skills and weakness, as in CP patients. For comparison, it is planned to assess the performance of the voluntary motion in healthy children.Acknowledgements
The study was supported by the Swiss National Science Foundation (Grant Number 173292).References
1. Mathewson MA, Lieber RL. Pathophysiology of muscle contractures in cerebral palsy. J Orthop Res. 2015 Jan;33(1):33-9.
2. Deligianni X, Pansini M, Garcia M, Hirschmann A, Schmidt-Trucksäss A, Bieri O, Santini F. Synchronous MRI of muscle motion induced by electrical stimulation. Magn Reson Med. 2017 Feb;77(2):664-672.
3. Weidensteiner C, Deligianni X, Santini F, Haas T, Madoerin P, Bieri O, Bracht-Schweizer K, Rutz E, Garcia M, Brunner R: Imaging of calf muscle contraction in pediatric patients with cerebral palsy and healthy children by dynamic phase contrast MRI, Proc ISMRM 2019, #141.
4. Mazzoli V, Gottwald LM, Peper ES, Froeling M, Coolen BF, Verdonschot N, Sprengers AM, van Ooij P, Strijkers GJ, Nederveen AJ. Accelerated 4D phase contrast MRI in skeletal muscle contraction. Magn Reson Med. 2018 Nov;80(5):1799-1811.
5. Sinha U, Malis V, Csapo R, Narici M, Sinha S. Shear strain rate from phase contrast velocity encoded MRI: Application to study effects of aging in the medial gastrocnemius muscle. J Magn Reson Imaging. J Magn Reson Imaging. 2018 Nov;48(5):1351-1357.
6. Santini F, Bieri O, Deligianni X, OpenForce MR: A low-cost open-source MR-compatible force sensor. Concepts Magn Reson Part B Magn Reson Eng. 2018;48B(4):e21404.
7. Deligianni X, Hirschmann A, Place N, Bieri O, Santini F. Dynamic MRI of plantar flexion: A comprehensive repeatability study of electrical stimulation-gated muscle contraction standardized on evoked force. PLoS One 2020 Nov 5;15(11):e0241832.
Figures