3044
Diffusion Tensor Imaging and Tractography in Deep Brain Stimulation Postoperative Patients with Parkinson's Disease1Department of Radiology, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China, 2Department of Neurosurgery, Center for Functional Neurosurgery, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China, 3MR Collaborations, Siemens Healthcare Ltd., Shanghai, China, 4MR Application Development, Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 5Department of Radiology, Wayne State University, Detroit, MI, United States
Synopsis
Preliminary evidence supports the safety of diffusion weighted tractography in postoperative patients with deep brain stimulation. Here we further test the feasibility in both DBS-on and DBS-off status. Both DBS ON and OFF diffusion weighted imaging are safe and the tractography results are significantly comparable. Furthermore, we found that the nigrostriatal pathway's deterministic tractography is feasible. Our results highlight that DBS ON DTI is particularly fitting for those patients who cannot control their disease symptoms without stimulation but need MRI.
INTRODUCTION
Nigrostriatal pathway, dentate rubro thalamic (DRTT) and hyperdirect pathway have been shown to be involved with control of motor behavior or to be responsible in the pathophysiology of tremor in Parkinson's disease (PD) patients [1-3]. The distances between deep brain stimulation (DBS) electrodes and specific white matter fiber tracts in patients may affect the outcome of surgery [4]. During the recovery process of post-DBS patients, the white matter fiber may change, that is, neural plasticity. Therefore, it is of great clinical and research value to evaluate the white matter tracts after DBS. Preliminary evidence supports the safety of diffusion weighted tractography in postoperative patients with DBS, but it has not been reported whether the different states of DBS (switch on or off) affect the fiber bundle reconstruction, and whether it is feasible to depict the tracks using deterministic tractography method.METHODS
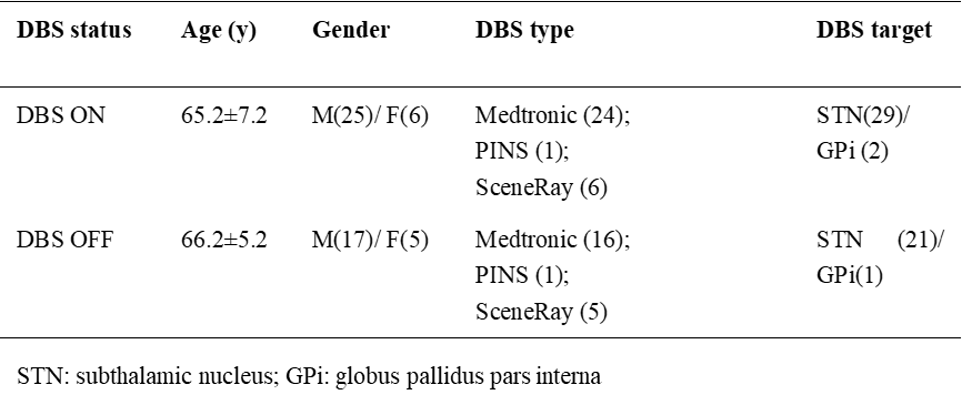
This study was approved by the local Institutional Review Board and all subjects signed a consent form. A total of 31 postoperative PD cases were collected on a 1.5 T MR scanner (Magnetom Aera; Siemens Healthcare, Erlangen, Germany) with a 16-channel head coil. At first, all the 31 patients were scanned with the DBS device on. After turning off the DBS device for about one hour, 22 of them were rescanned using the same MRI protocol. The complete sequence consisted of 64 diffusion-weighted directions with b = 1000 s/mm2 and 16 interspersed scans where b = 0 s/mm2. TR= 6500 ms, TE= 126 ms, matrix= 110×110, voxel size= 2×2×2 mm3, BW= 1336 Hz/pix, acquisition time= 9 min and 13 s, SAR= 0.34±0.02 w/kg, lower than the recommend threshold level (0.4 w/kg) [5]. Nine patients with severe shaking symptoms after turning off the DBS device gave up the second scan. The clinical data of subjects were shown in Table 1. For a visually image quality assessment (QA) [6], A trained analyst visually inspected all 80 volumes for each diffusion tensor imaging (DTI) scan. Any volume that appeared to contain artifact was recorded. The deterministic tractography method was used to reconstruct the fibers[7]. The track count numbers between left and right-side fibers in both DBS ON and OFF images, and the differences between DBS ON and OFF in the same side fibers were compared using paired t-test. Findings of a p value > 0.05 were considered significantly similar.RESULTS
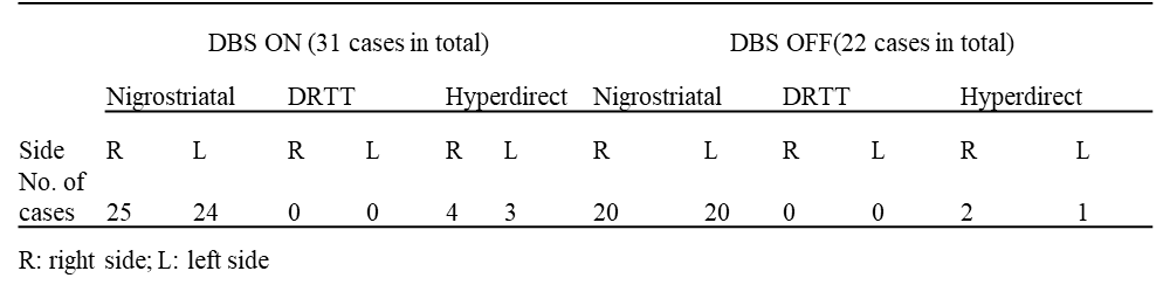
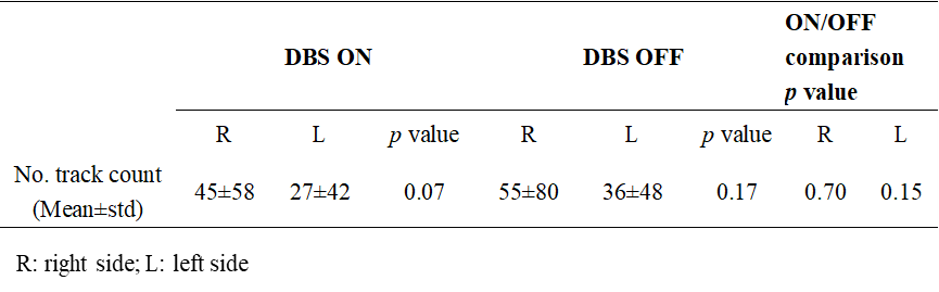
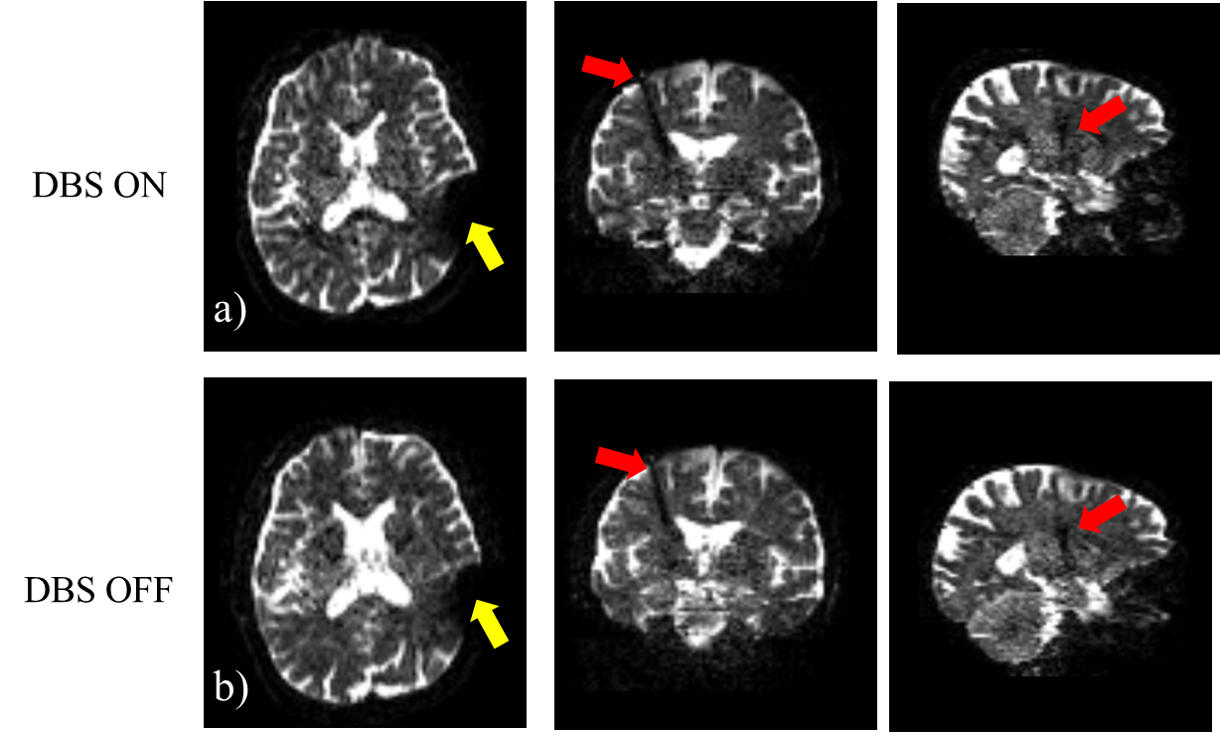
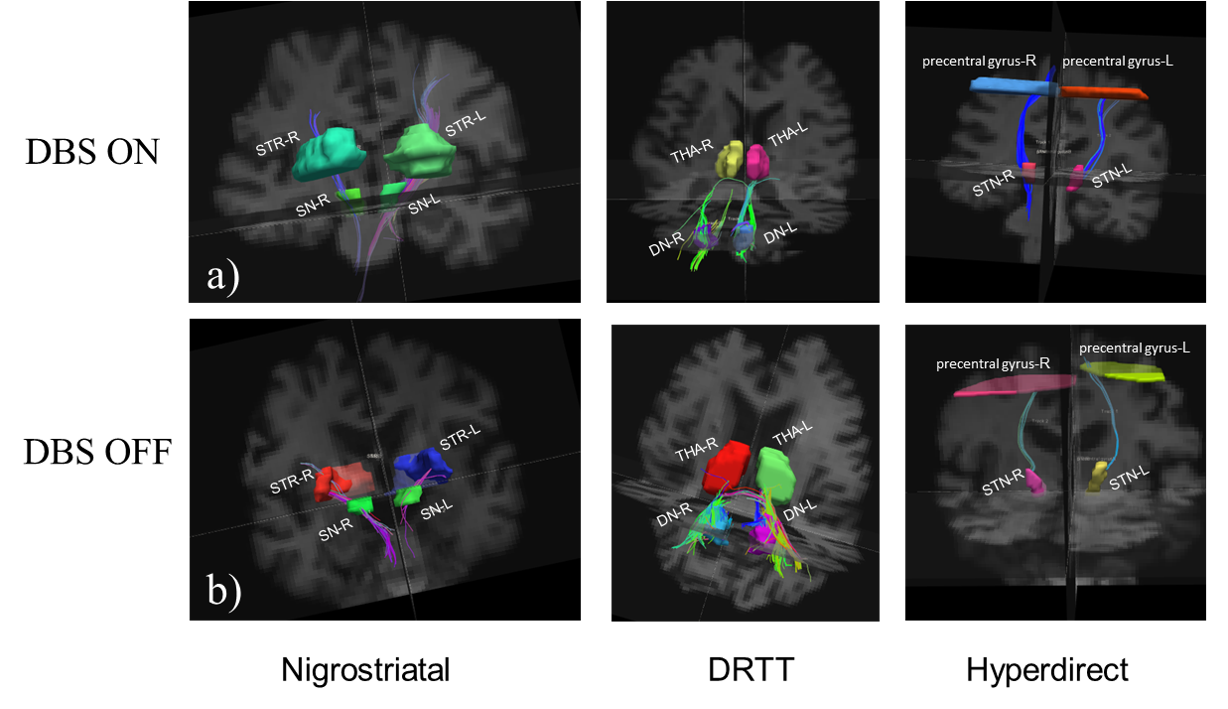
The B0 images of one representative subject in DBS ON and OFF states, respectively, were shown in Figure 1. Figure 2 shows the deterministic tracking result of the same representative subject in two states: a) DBS ON,and b) DBS OFF. For both the DBS-ON and DBS-OFF DTI, nigrostriatal pathway can be reconstructed in more than two-thirds cases; hyperdirect pathway can be seen in a small number of cases (about 1/10); and DRTT cannot be reconstructed at all. The number of the successfully reconstructed cases were shown in Table 2. The track count numbers of right nigrostriatal pathway were larger than that of the left nigrostriatal pathway, but there were no significant differences (DBS ON: p value=0.07; DBS OFF: p value=0.17). Compared the nigrostriatal pathway track count numbers of the DBS ON to the DBS OFF, there were no statistical differences in both side (right side: p value=0.7; left side: p value=0.15) as shown in Table 3.DISCUSSION
The susceptibility-induced artifacts and the quality of the images were visually assessed. In general, the image quality is as good as Muller’s previous work, while they used a 25-min protocol[4]. The artifact was found to be generated by the connector wire fixing cap and the electrode wire, resulting in signal loss observed over the occipital lobe. Given that access to MRI scanners in most centers is limited, it would be an advantage if the scanning time could be shortened as much as possible without compromising the quality of the images. The proposed 9-min scanning protocol in this study is more practical in clinic.Both DBS ON and OFF DTI are safe and feasible. DBS ON DTI is especially suitable for those patients who cannot control their disease symptoms without stimulation but need MRI.
Deterministic tractography of the nigrostriatal pathway is feasible in PD patients after DBS surgery. The track count numbers between left and right-side nigrostriatal pathway in both DBS ON and OFF images, and between DBS ON and OFF in the same side fibers were significantly comparable.
CONCLUSION
Both DBS ON and OFF DTI are safe and the tractography results are significantly similar. It is feasible to depict the nigrostriatal pathway using deterministic tractography method based on the postoperative DTI. Postoperative DTI may provide a promising tool in the future, to align the post-operative electrode position in relation to the intra-cerebral fiber tracks or to evaluate the changes of the fibers.Acknowledgements
No acknowledgement found.References
[1] Tan WQ, Yeoh CS, Rumpel H, et al. Deterministic Tractography of the Nigrostriatal-Nigropallidal Pathway in Parkinson's Disease. Sci Rep. 2015;5:17283.
[2] Hana A, Hana A, Dooms G, Boecher-Schwarz H, Hertel F. Depiction of dentatorubrothalamic tract fibers in patients with Parkinson's disease and multiple sclerosis in deep brain stimulation. BMC Res Notes. 2016;9:345.
[3] Hammond C, Bergman H, Brown P. Pathological synchronization in Parkinson's disease: networks, models and treatments. Trends Neurosci. 2007;30(7):357-364.
[4] Muller J, Alizadeh M, Li L, et al. Feasibility of diffusion and probabilistic white matter analysis in patients implanted with a deep brain stimulator. Neuroimage Clin. 2020;25:102135.
[5] Larson PS, Richardson RM, Starr PA, Martin AJ. Magnetic resonance imaging of implanted deep brain stimulators: experience in a large series. Stereotact Funct Neurosurg. 2008;86(2):92-100.
[6] Roalf DR, Quarmley M, Elliott MA, et al. The impact of quality assurance assessment on diffusion tensor imaging outcomes in a large-scale population-based cohort. Neuroimage. 2016;125:903-919.
[7] Muller J, Alizadeh M, Mohamed FB, et al. Clinically applicable delineation of the pallidal sensorimotor region in patients with advanced Parkinson's disease: study of probabilistic and deterministic tractography. J Neurosurg. 2018;1-12.
Figures