3000
T2-weighted Pelvic MR Imaging Using PROPELLER with Deep Learning Reconstruction for Improved Motion Robustness1Radiology, MD Anderson Cancer Center, Houston, TX, United States, 2Radiology, Stanford University, Stanford, CA, United States, 3Imaging Physics, MD Anderson Cancer Center, Houston, TX, United States, 4Biostatistics, MD Anderson Cancer Center, Houston, TX, United States, 5Global MR Applications and Workflow, GE Healthcare, Houston, TX, United States
Synopsis
In oncologic MRI, sagittal T2 weighted images are usually acquired to assess gynecologic malignancy. Motion artifacts may render pathology difficult to detect due to patient or bowel motion or the presence of air in the rectum. PROPELLER sequence has shown promising results to reduce motion-related artifacts. Our work shows that DL Recon can be combined with PROPELLER and further help reduce noise and improve the overall image quality for T2-weighted imaging of gynecological malignancies. The combination of PROPELLER (Non-DL) and DL reconstruction could be synergistic in improving image quality.
Summary of Main Findings
Deep Learning-based image reconstruction (DL-Recon) improved image quality with better image SNR, increased image sharpness and reduced artifacts.Synopsis
In oncologic MRI, sagittal T2 weighted images (WI) are usually acquired to assess gynecologic malignancy. Motion artifacts may render pathology difficult to detect. PROPELLER has shown promising results to reduce motion-related artifacts. Our work shows that DL-Recon can be combined with PROPELLER and further help reduce noise and improve the overall image quality for T2WI. The combination of PROPELLER (Non-DL) and DL reconstruction could be synergistic in improving image quality.Introduction
T2WI is an essential component of an MRI exam for the assessment of female gynecologic organs. However, conventional T2WI (Figure 1) and the fast spin echo and Turbo spin echo sequences are often degraded by bowel peristalsis, motion and breathing artifact and pulsation artifacts from the vessels. Such a degradation of image quality may result in loss of diagnostic information. The (Non-DL) uses periodically rotated overlapping k-space lines through the center of the k-space and therefor is more resistant to motion than the standard Cartesian sampling by the FSE or TSE sequence (1). DL and Machine Learning (ML) have recently been used in medical research (2, 3). For prostate MRI, ML and DL have been used successfully for prostate segmentation, cancer detection, evaluation of local aggressiveness, staging, pretreatment assessment, and biochemical recurrence (4). DL techniques have also been reported for improved image quality and noise reduction (5, 6). The DL technique we used in this work was based on a residual encoder. Instead of directly generating high SNR images, the residual encoder offered flexibility on noise reduction. This can help avoid aggressive denoising with a controlled level of noise, making the images more natural to human perception. The DL network was embedded into the reconstruction pipeline such that both conventional and DL image series could be generated from a single set of raw MRI data. Our hypothesis is that a combination of DL images will provide better image quality and decreased artifacts compared to the conventional Non-DL for T2WI of the pelvis.Materials and Methods
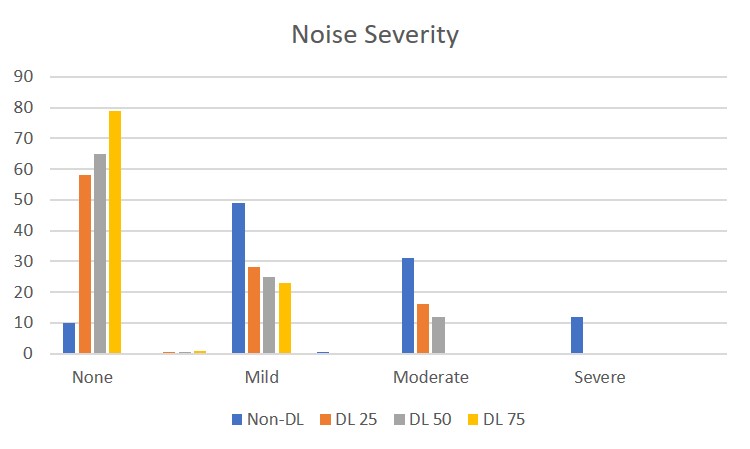
34 patients who underwent pelvic gynecologic MRI on the same scanner (GE 3T 750W, Waukesha, WI) were included in this prospective IRB approved trial. The average age of the subjects was 58 years, with a median age of 59 years and a range of 59-85 years. The specific sequences that were evaluated were sagittal T2W FSE and Non-DL of the pelvis with and without hysterectomy. Raw data from sagittal Non-DL imaging (FOV=20cm, matrix=300x300, slice thickness=5mm, NEX= 2.3) were acquired with a 24-channel torso array coil. The images were then reconstructed with conventional reconstruction and a DL. The DL comprised a deep convolutional residual encoder network trained using a prior database for noise removal and high in-plane resolution (7). The DL-reconstruction offered a tunable noise reduction factor to accommodate user preference. In this study three different noise reduction factors (DL 25%, DL 50% and DL 75%) were selected. The resulting images were blindly reviewed and scored qualitatively by three gynecologic MR imaging radiologists. Each radiologist scored the images by a side-to-side in the following categories: (i) overall image artifacts (present or absent), noise (none, mild, moderate and severe), relative sharpness (on a scale of 4, best sharpness was ranked 1 and the least sharp image was ranked 4), and overall image quality (excellent, diagnostic, and impairing diagnosis). All the readers also ranked their sequence preference on a 4-point scale (1-best4- worst). The reader ratings were summarized using frequencies and percentages. Generalized estimating equation method (GEE) was used to assess the effect of methods on the Likert scales, adjusting for reader. A region of interest of at least 1cm 2 in size was drawn on the left iliacus muscle and the ventral abdomen fat and CNR and SNR were calculated. Pair-wise comparisons among methods with respect to the SNRs and CNRs were performed based on a linear mixed model. P-values of pairwise comparisons were adjusted using the Tukey-Kramer method to control overall type I error rate. Inter-observer agreement was assessed using the kappa statistic. P-value was considered statistically significant at less than 0.05.Results
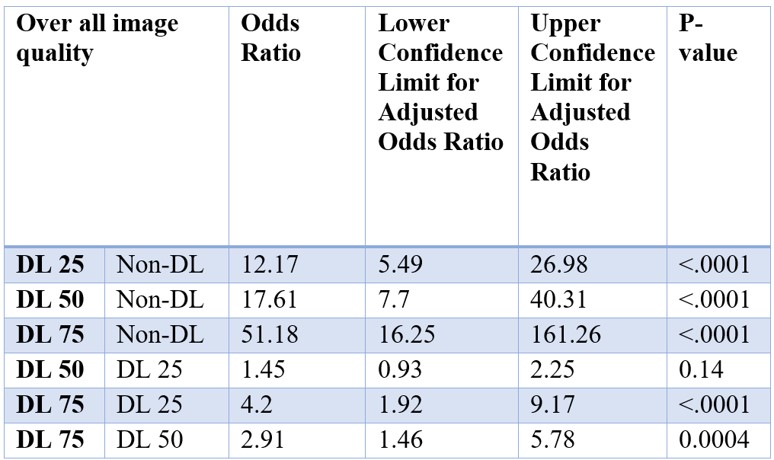
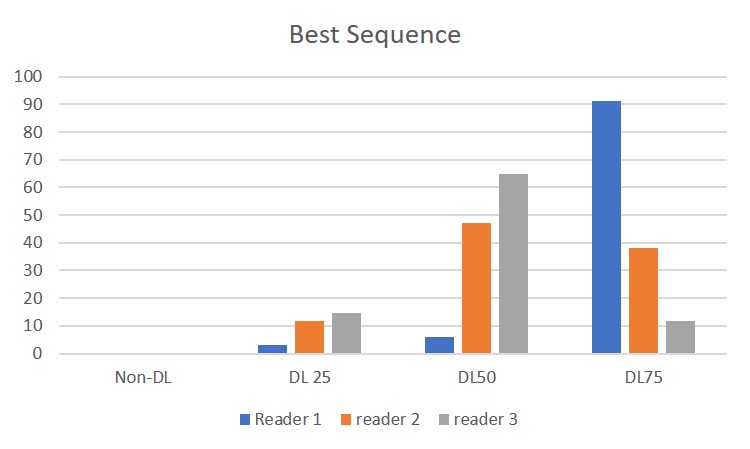
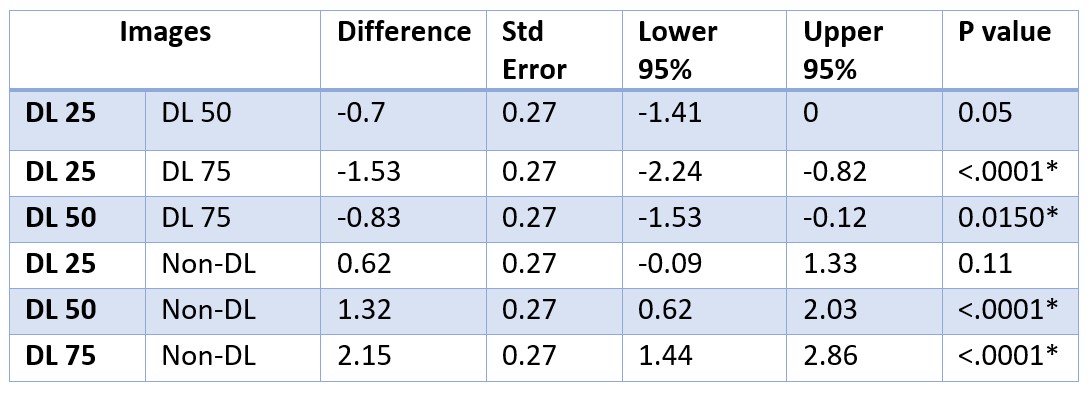
Figure 2 lists the results for overall image quality for each series. For image quality DL25%, DL50% and DL75% images were significantly better than non-DL (p<0.0001). Additionally, DL 50% and DL 75% images were ranked by readers as best sequences in 86% cases (Figure 3). The SNR (Figures 4 & 5) of iliacus muscle on DL recon images was significantly better than non-DL images at p<0.0001*. There was no difference in CNR. Although all the readers preferred DL images, especially DL 50% and DL 75% images, the kappa statistics showed little or no agreement in the best denoising level among the readers. Because different readers may have different preferences on SNR levels, it may be desirable for the software to offer such flexibility in the noise reduction level.Conclusion
PROPELLER sagittal T2-weighted images of the female pelvis with DL reconstruction resulted in improved image quality and SNR.Acknowledgements
No acknowledgement found.References
1. Zaccagnino E, Devincent C, Leelakanok N, Phelps AS, Zapala M, Worters PW, et al. Assessment of quiet T2 weighted PROPELLER sequence in pediatric abdominal imaging. Clin Imaging. 2019;53:12-6.
2. Lundervold AS, Lundervold A. An overview of deep learning in medical imaging focusing on MRI. Z Med Phys. 2019;29(2):102-27.
3. Davenport T, Kalakota R. The potential for artificial intelligence in healthcare. Future Healthc J. 2019;6(2):94-8.
4. Cuocolo R, Cipullo MB, Stanzione A, Ugga L, Romeo V, Radice L, et al. Machine learning applications in prostate cancer magnetic resonance imaging. Eur Radiol Exp. 2019;3(1):35.
5. Kidoh M, Shinoda K, Kitajima M, Isogawa K, Nambu M, Uetani H, et al. Deep Learning Based Noise Reduction for Brain MR Imaging: Tests on Phantoms and Healthy Volunteers. Magn Reson Med Sci. 2019.
6. Jiang D, Dou W, Vosters L, Xu X, Sun Y, Tan T. Denoising of 3D magnetic resonance images with multi-channel residual learning of convolutional neural network. Jpn J Radiol. 2018;36(9):566-74.
7. Kim KH, Do WJ, Park SH. Improving resolution of MR images with an adversarial network incorporating images with different contrast. Med Phys. 2018;45(7):3120-31.
Figures