2998
Motion Robust High-Resolution Pelvic Imaging using PROPELLER and Deep Learning Reconstruction1Department of Radiology, UW Madison, Madison, WI, United States, 2Global MR Applications & Workflow, GE Healthcare, Madison, WI, United States, 3Global MR Applications & Workflow, GE Healthcare, Denver, CO, United States, 4Global MR Applications & Workflow, GE Healthcare, Houston, TX, United States, 5GE Healthcare, Houston, TX, United States
Synopsis
We evaluated the utility of PROPELLER T2 FSE with deep-learning (DL) reconstruction in the setting of prostate and rectal imaging, with the goal of overcoming respiratory and peristaltic motion, improving image sharpness, and achieving high-resolution imaging within a comparable scan time to the traditional T2 FSE techniques. We demonstrated that in absence of DL reconstruction, the PROPELLER T2 FSE images suffer from excessive noise and lower subjective quality. However, with utilization of DL reconstruction, High-resolution and motion robust images were obtained at clinically acceptable scan times.
Introduction
High resolution T2 fast spin-echo (FSE) MRI of the pelvis is the main pulse sequence for characterization of disease and pathology for several clinical indications, including detection of prostate cancer in the transition zone as well as local staging of rectal cancer. The need for high signal-to-noise and high-resolution images for these indications results in prolonged scan times, which in turn lead to motion. Furthermore, the physiologic peristaltic motion of the rectum often results in blurring, which can render the images nondiagnostic. Hence, anti-peristaltic agents (e.g., glucagon) are often used for these MRI exams, and this leads to workflow disruptions, added cost, and patient dissatisfaction. Although PROPELLER imaging can reduce motion, it is often associated with prolonged scan times due to the need for oversampling to overcome streak artifacts. However, with utilization of a deep-learning reconstruction algorithm, we demonstrated a T2 FSE PROPELLER technique that achieved diagnostic quality images in comparable scan times to the current conventional techniques.Methods
3 volunteers and 1 patients were included in this study with IRB approval and written informed consent. Imaging studies were performed on 3T MRI scanners on (SIGNA Premier, GE Healthcare, Waukesha, USA), using a 30-channel anterior surface coil and a 60-channel posterior coil embedded within the table. The typical imaging parameters of the FSE and PROPELLER included: axial orientation; FOV = 180 × 180 mm2 (High Res.) / 260 × 260 mm2 (Low Res.); matrix = 360x360 (High Res. PROPELLER) / 384x256 (High Res. FSE) / 384x224 (Low Res. FSE); slice thickness = 2.4 mm; number of slices = 30; phase wrap = 2 (High Res) / NA (Low Res.); flip angle = 120 (PROPELLER) / 111 (FSE) degrees; TE = 100 ms and TR = 3470 (PROPELLER) / 3000 (FSE). Two sets of images were generated from the PROPELLER and FSE raw data: one with conventional reconstruction and the other with deep-learning reconstruction. The deep-learning reconstruction was imbedded in the product reconstruction pipeline and consists of a deep convolutional network trained with a supervised learning approach using pairs of images representing near-perfect and conventional MRI images for noise and artifacts removal and high in-plane resolution (1,2). The database of training images spans a broad range of image content, enabling generalizability of the network across all anatomies. The network offered a tunable noise reduction factor to accommodate user preference. In this work, we chose 75% denoising level.Results
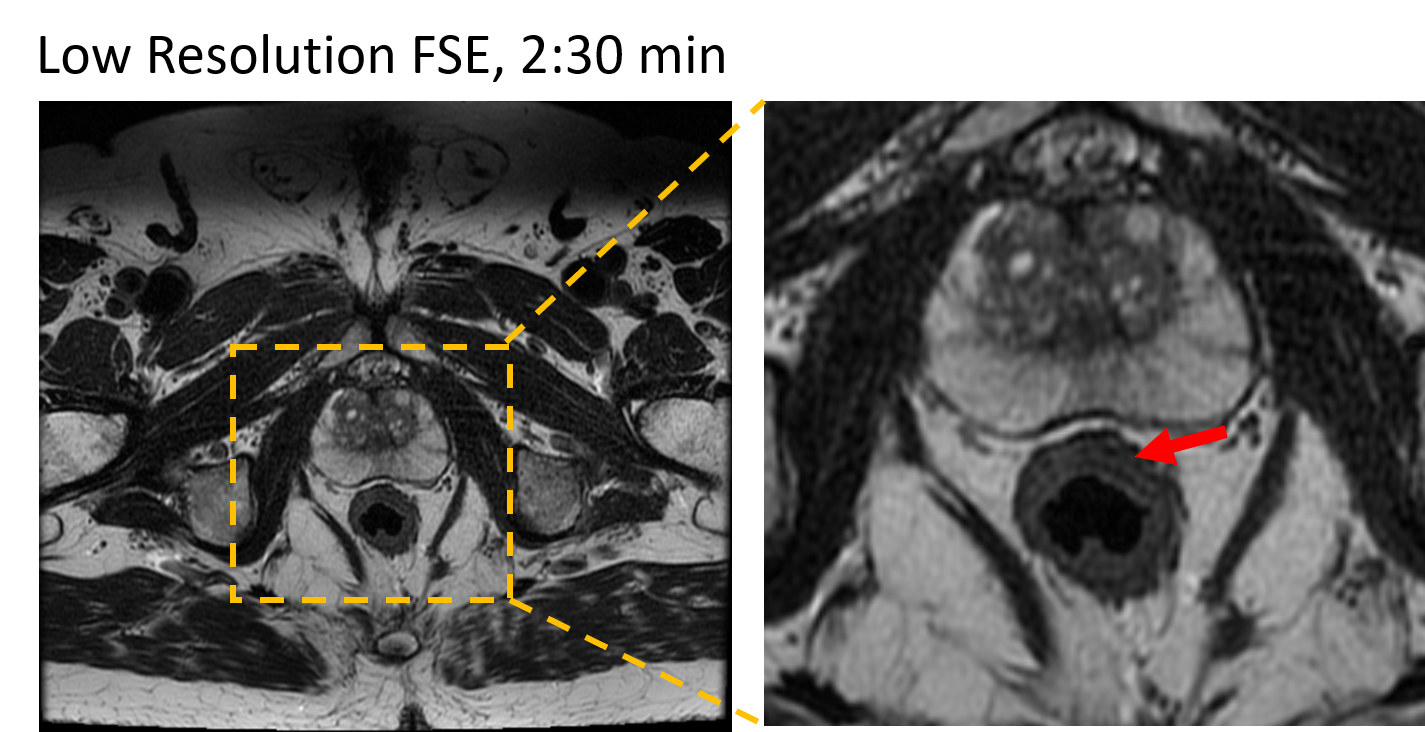
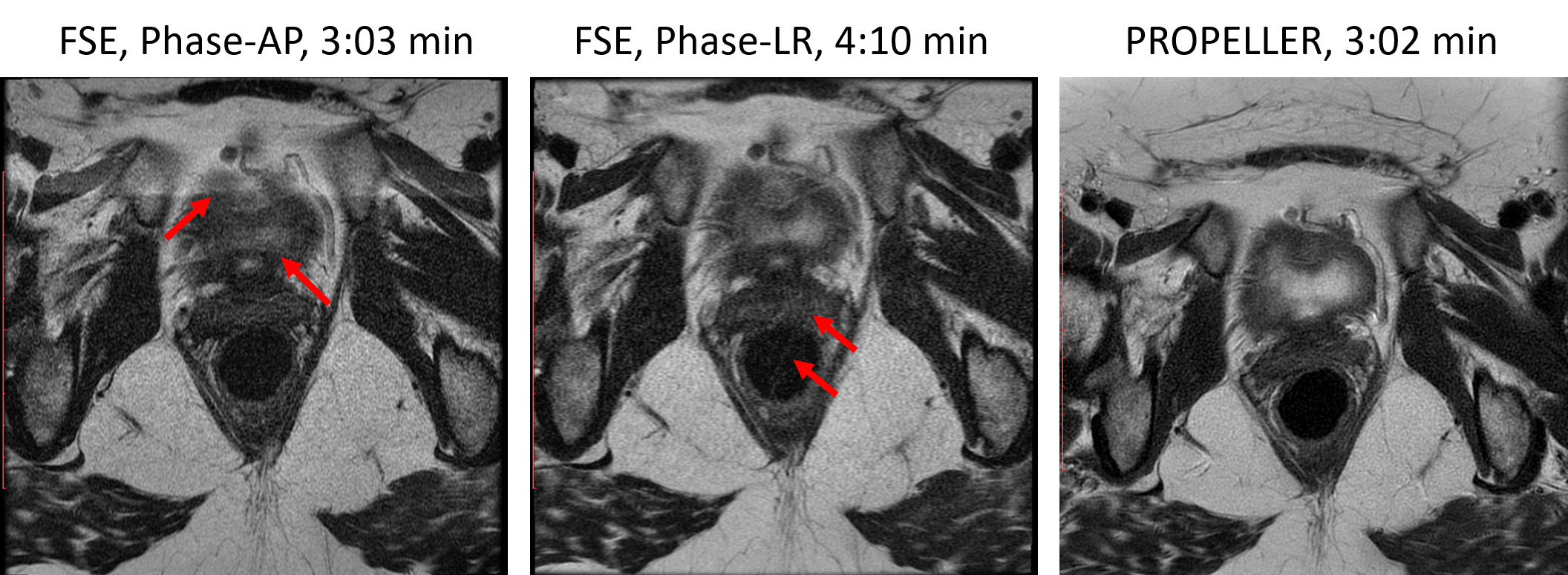
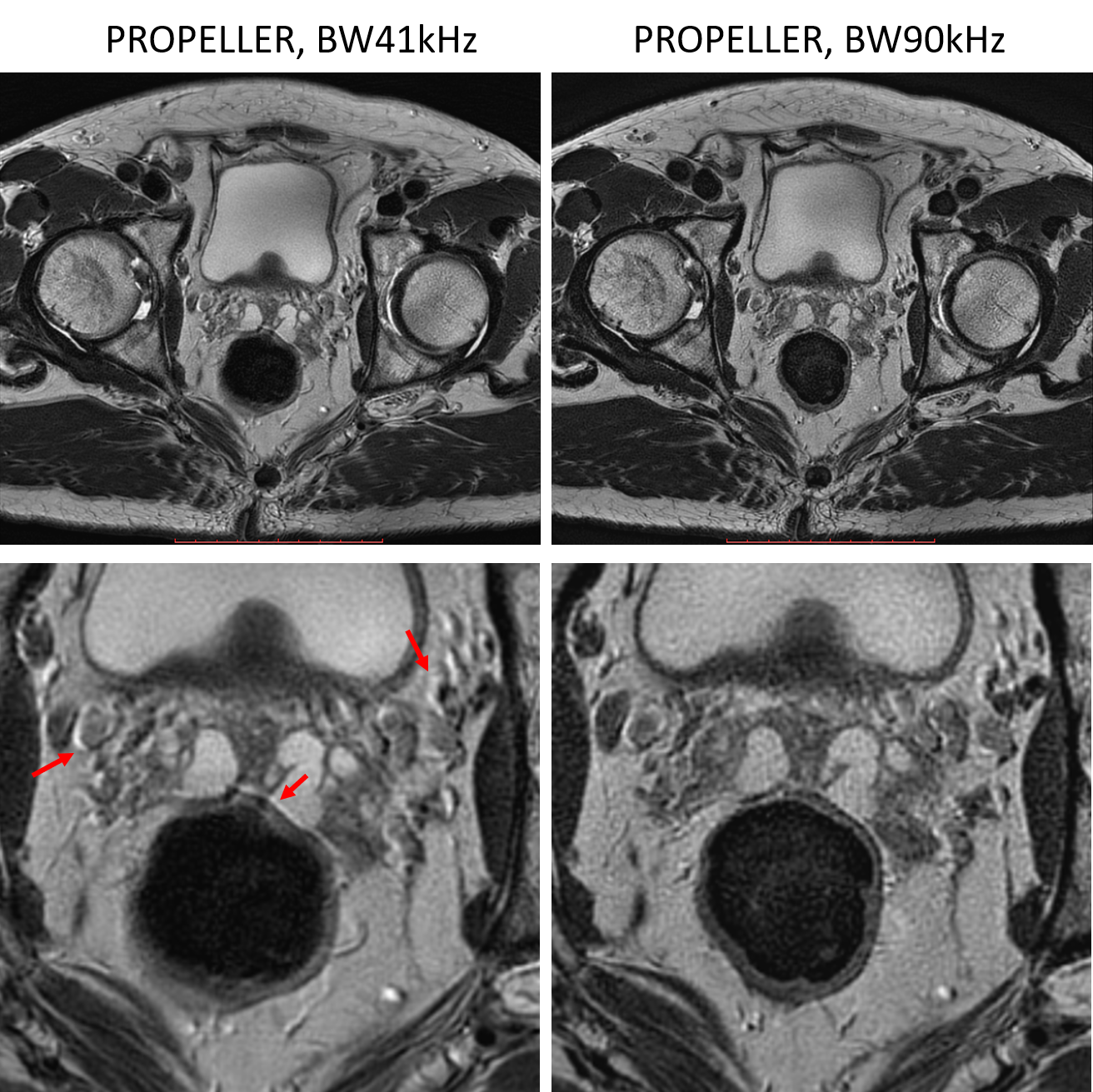
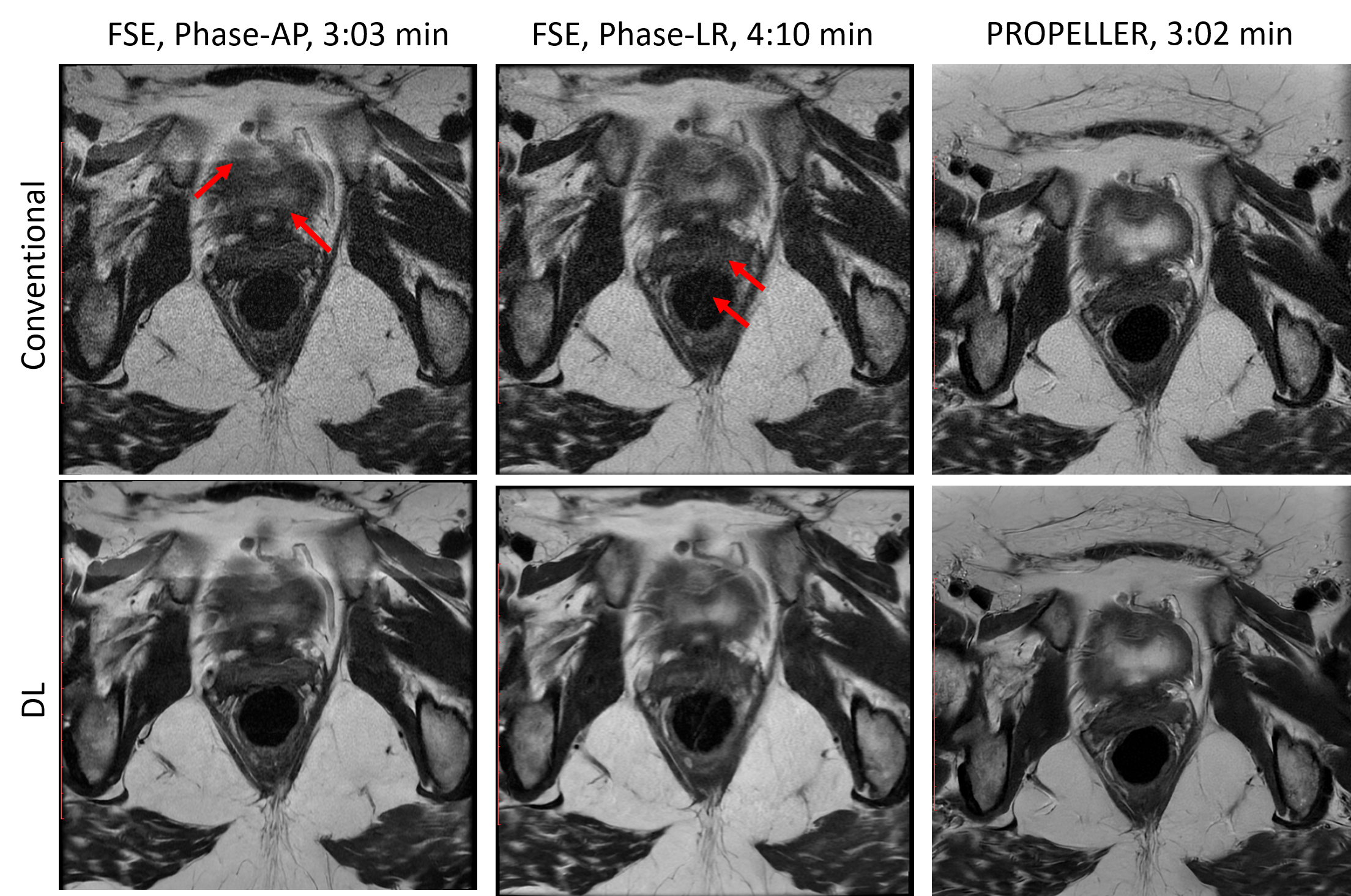
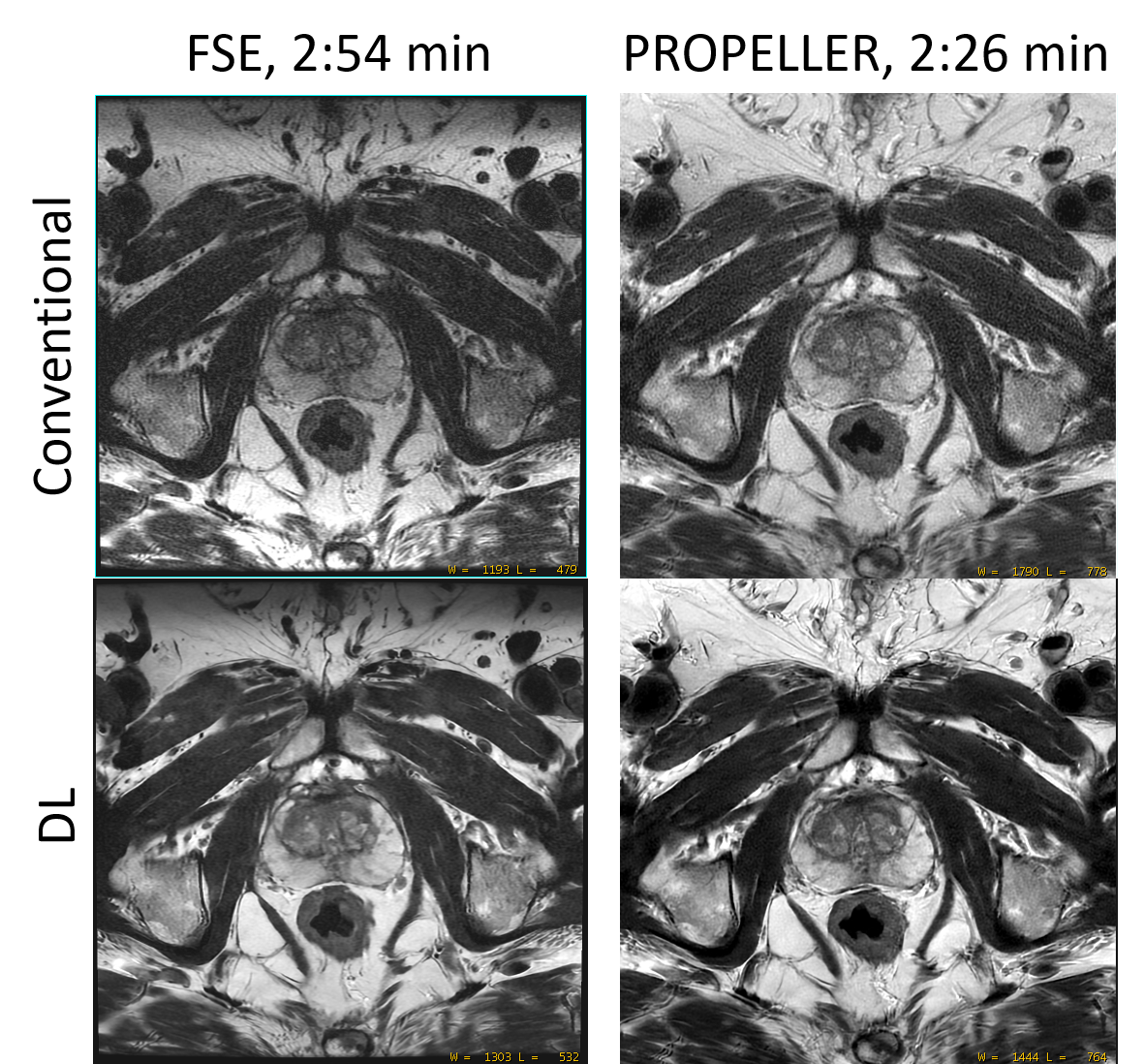
Rectal wall layers are often not well visualized in low resolution T2W FSE images, and ringing artifacts also make it worse, as shown in Figure 1. Increasing the in-plane resolution often requires multi-shot acquisition and also increases the scan time. Multi-shot FSE acquisition is sensitive to motion, such as respiratory motion, bowel motion, etc. For rectal imaging, it can reduce the scan time by choosing phase encoding along the A-P (Anterior-Posterior) direction, but this make it very sensitive to respiratory motion, as shown in Figure 2a. Phase encoding can be applied along L-R (Left-Right) direction to minimize the respiratory motion artifacts. However, this will further increase the scan time and also cannot avoid bowel motion artifacts, as shown in Figure 2b. As shown in Figure 2c, PROPELLER can be used to minimize motion artifacts in rectal imaging, but the scan time is usually longer than FSE. If keeping the scan time same to that of FSE, the SNR of PROPELLER image is low. Although reducing receiver bandwidth could improve the SNR, it also made the chemical artifacts more visible in high-resolution PROPELLER images (Figure 3a). High receiver bandwidth is preferred in high-resolution PROPELLER imaging. To improve the SNR without increasing scan time or reducing in-plane resolution, a deep-learning based reconstruction method was applied to both FSE and PROPELLER image reconstruction, as shown in Figure 4. With improved SNR and resolution, the motion artifacts were also more visible in FSE DL images. However, PROPELLER DL image showed less motion artifacts due to its robustness to motion. With improved SNR and in-plane resolution using the deep-learning based reconstruction method and the robustness to motion, high-resolution PROPELLER images showed improved image sharpness and overall image quality compared to FSE images.Conclusion
PROPELLER T2-weighted images of pelvis with DL reconstruction resulted in improved image quality, including improved SNR, in-plane resolution and robustness to motion.Acknowledgements
No acknowledgement found.References
1. R. Marc Lebel, Performance characterization of a novel deep learning-based MR image reconstruction pipeline, arXiv:2008.06559
2. Xinzeng Wang, Daniel Litwiller, Marc Lebel, Ali Ersoz, Lloyd Estkowski, Jason Stafford, Ersin Bayram. High resolution T2W imaging using deep learning reconstruction and reduced field-of-view PROPELLER, ISMRM 2020: 820
Figures