2991
T2WI liver MRI with deep learning-based reconstruction: a clinical feasibility study in comparison to conventional T2WI liver MRI1Department of Radiology, Zhongshan Hospital, Shanghai, China, 2United Imaging Healthcare, Shanghai, China, 3Shanghai United Imaging Intelligence, Shanghai, China
Synopsis
Liver magnetic resonance imaging (MRI) is limited by several technical challenges, including relatively long acquisition time and respiratory motion artifacts. Recently, deep learning methods have been proposed to reconstruct undersampled k-space data by training deep neural networks. In this study, we raised a U-net convolutional neural network architecture to improve the reconstruction speed and image quality of liver T2-weighted MRI. This technique was able to cover the whole liver during one breath hold and showed promising performance in image quality and lesion detectability.
Introduction
Despite its improved sensitivity and specificity in the detection of liver tumors compared with ultrasonography (US) and computed tomography (CT) 1, liver magnetic resonance imaging (MRI) is still limited by several technical challenges, such as relatively long acquisition time and respiratory motion artifacts 2. Recently, deep learning methods have been proposed to reconstruct undersampled k-space data by training deep neural networks 3,4. Among these deep neural network studies, a U-net architecture has been proposed to reconstruct images. This architecture is originally intended for image segmentation with contracting and expanding paths to capture the global and local contexts simultaneously. The goal of this study was to improve the reconstruction speed and image quality of liver T2-weighted (T2WI) MRI by using a U-net convolutional neural network (CNN) architecture.Materials and Methods
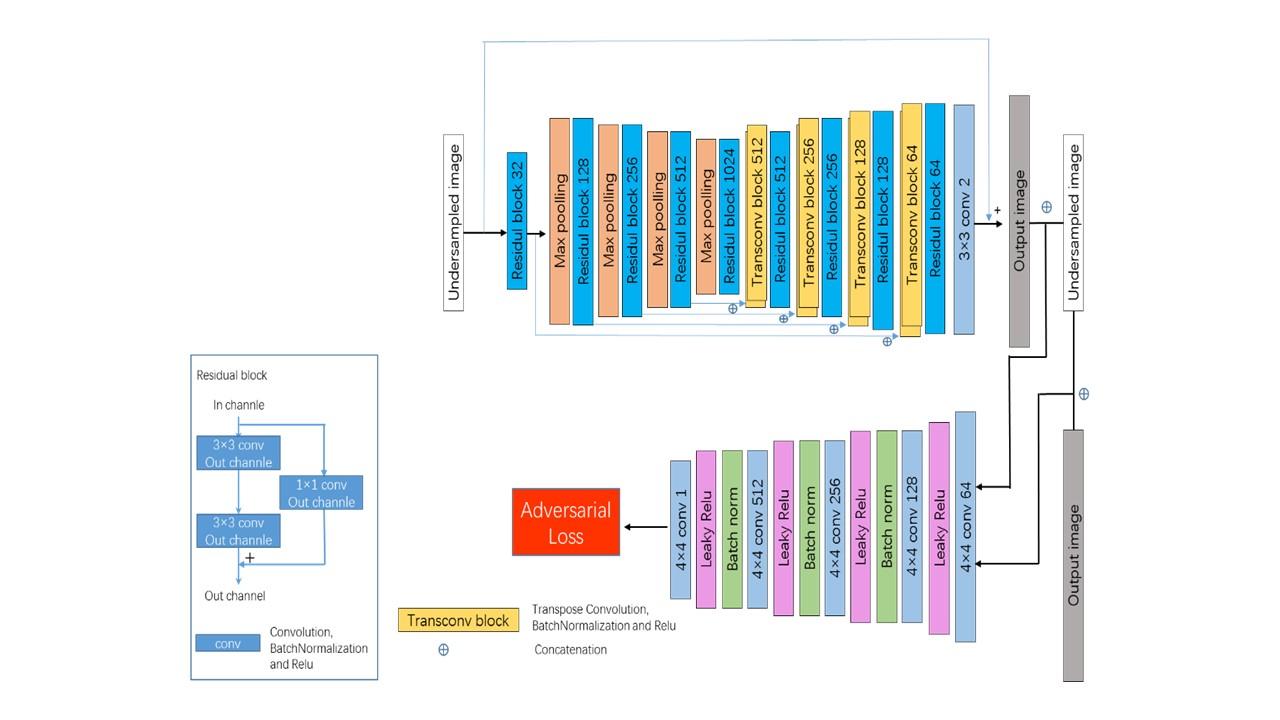
One hundred and fifty-two adult patients with suspected liver diseases were included in this prospective study. All patients underwent conventional multi-breath-hold (MBH) T2WI sequence and single-breath-hold (SBH) T2WI sequence with deep learning-based reconstruction sequence at 3.0 T MR scanner (uMR 770, United Imaging Healthcare, Shanghai, China).An extended fully CNN with paired images 3 was utilized in this study to realize the deep learning-based reconstruction. The input of the network was the real and imaginary part of the under-sampled images after applying the inversed Fourier transform to their corresponding k-space signal, and the output of the network was the real and imaginary part of the reconstructed sequences. This network was similar to conventional U-net, except that the convolution operation in the original U-net was replaced by residual blocks 5, which consisted of two convolution operations and a skipping connection. In order to facilitate the convergence speed during learning, a long skipping connection was also added to the network between the input and output of the network to learn the residual between the fully-sampled images and under-sampled images. The least squared generative adversarial network training strategy 6 was adopted to further improve the quality of the reconstructed images. Details of the network are shown in Figure 1.
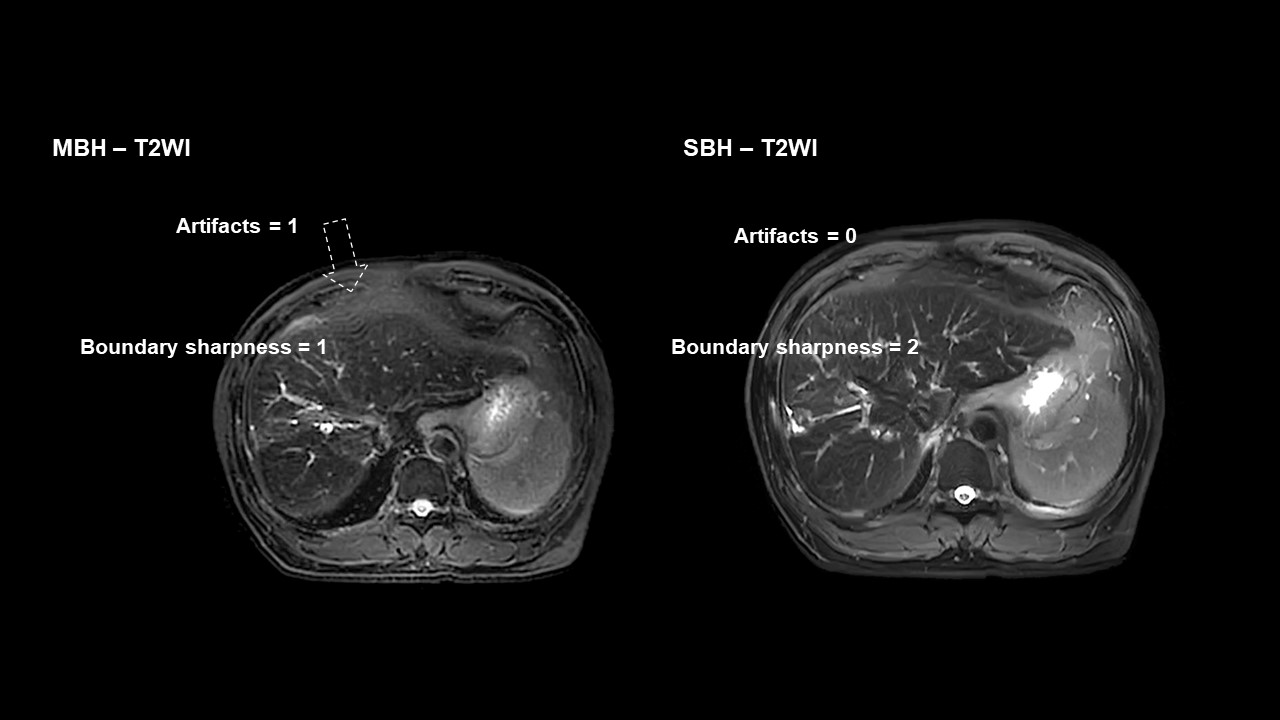
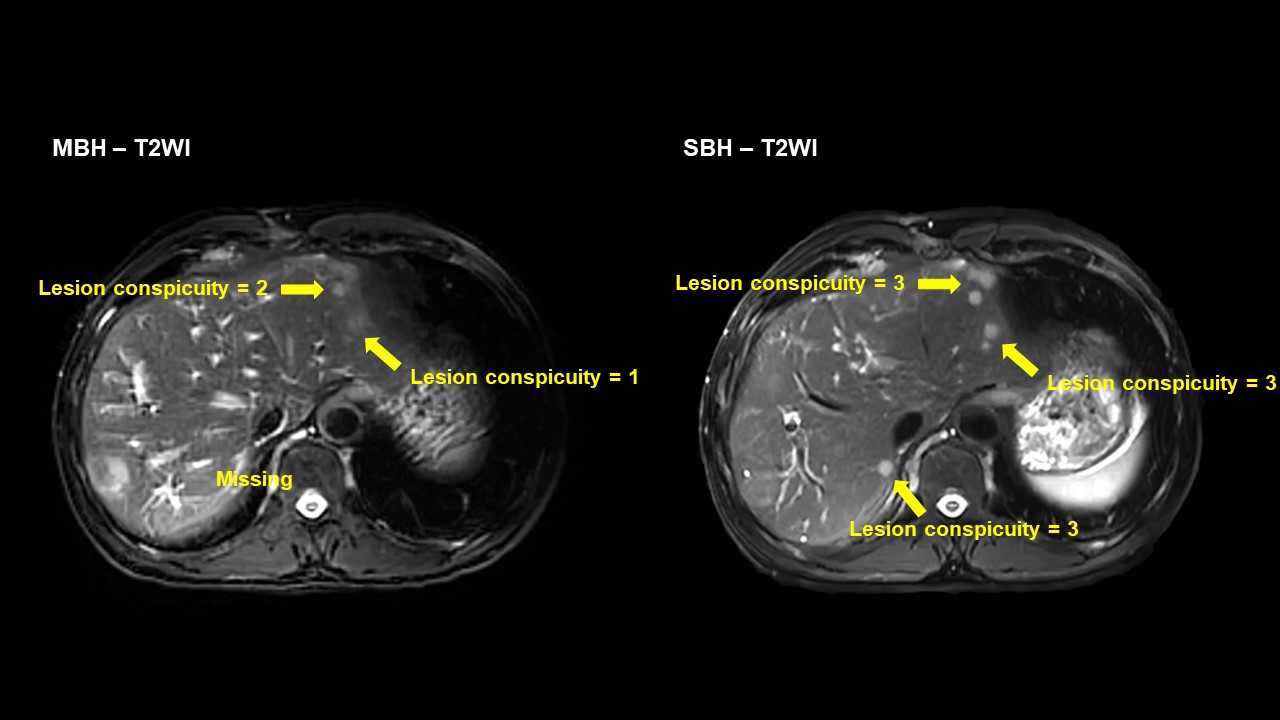
Imaging analyses were performed by two experienced radiologists. To assess the image quality, each reader evaluated the motion artifacts on a four-point scale: score 0: absent, no visible motion artifacts; score 1: mild, minor motion artifacts, not impairing diagnostic quality; score 2: moderate, moderate motion artifacts, interfering with diagnostic quality; score 3: severe, prominent motion artifacts, impairing diagnostic quality. Liver boundary sharpness was graded on a four-point scale: score 0: no visible boundary; score 1: ill-defined boundary; score 2: obscure boundary; score 3: well-defined boundary. To evaluate the lesion detectability, lesion conspicuity was rated on a four-point scale: score 0: absent; score 1: poor; score 2: moderate; score 3: good.
Interobserver agreement was calculated by using the Bland-Altman method and Cohen’s kappa. The lesion detection rate from the SBH-T2WI and MBH-T2WI was compared by using the chi-square test. The motion artifact scores, boundary sharpness scores and lesion conspicuity scores were compared by using the nonparametric Wilcoxon matched pairs test.
Results
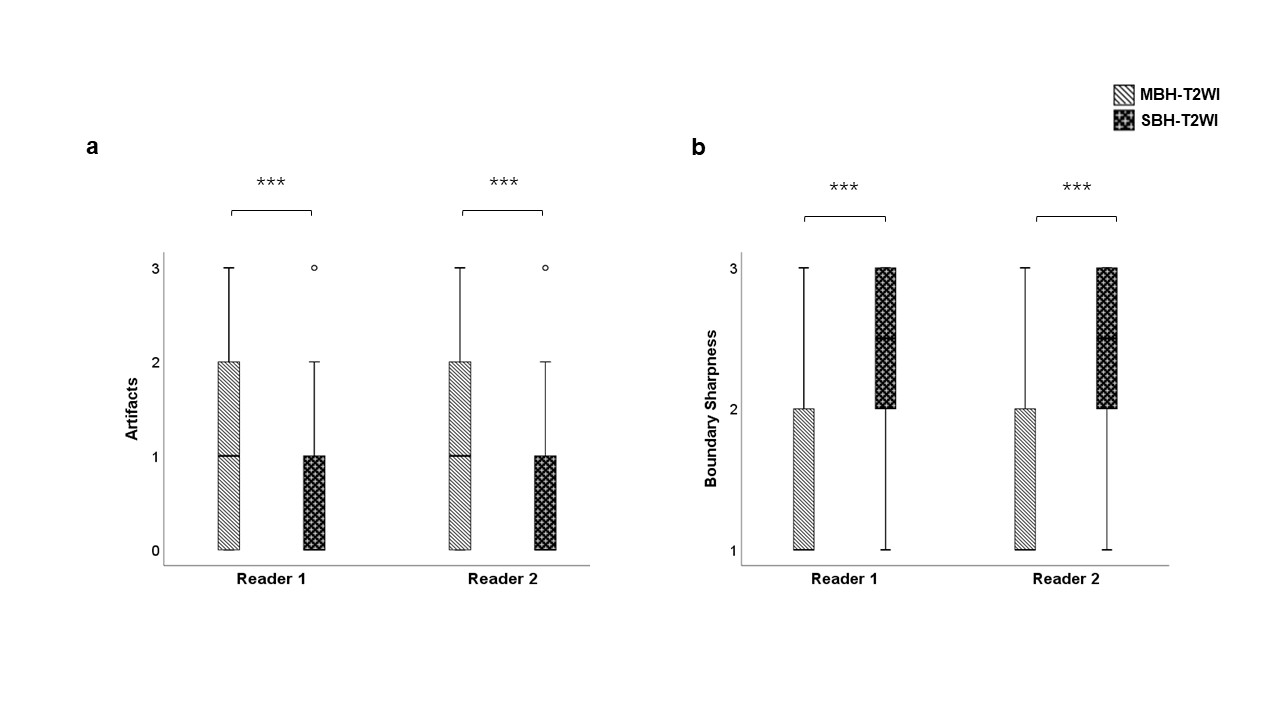
The lesion detection rate of SBH-T2WI was significantly higher than MBH-T2WI (P<0.001). Besides, the difference of lesion detection rate between the two sequences was statistically significant for small (≤10 mm) liver lesions (P<0.001), while was not significant for large (>10 mm) lesions (P=0.253).Example of image quality analysis is shown in Figure 3. The motion artifact score of SBH-T2WI was significantly lower than MBH-T2WI (P<0.001) and the boundary sharpness score of SBH-T2WI was significantly higher than MBH-T2WI (P<0.001) (Figure 3).
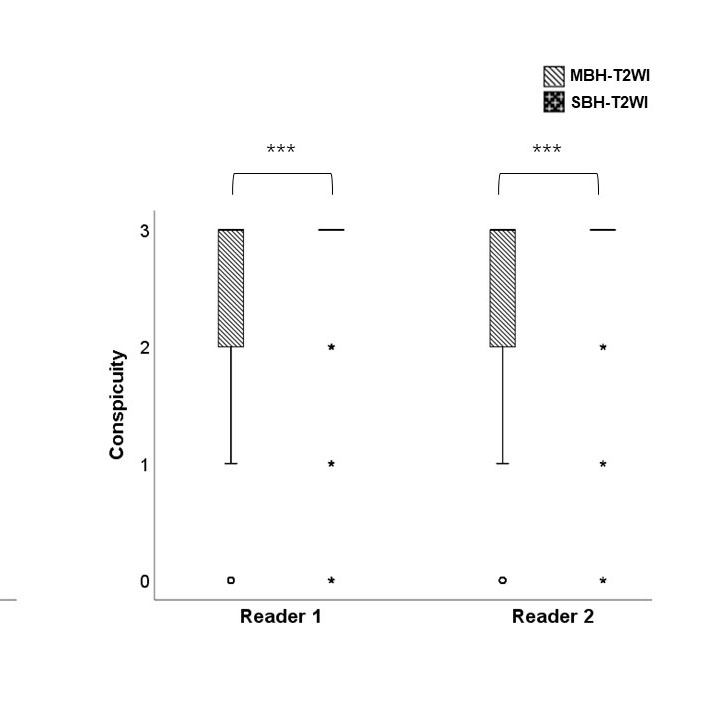
Example of focal liver lesion assessment is shown in Figure 4. The lesion conspicuity score of SBH-T2WI was significantly higher than MBH-T2WI (P<0.001) (Figure 5).
Discussion & Conclusion
Acquisition time in MRI can be reduced by faster scanning or sub-sampling. The former comes at the expense of image resolution and/or signal noise ratio. For the latter, many reconstruction methods such as half-Fourier (HF), parallel imaging (PI), compressed sensing (CS) and the combination of these methods, have been introduced in clinical MRI 7,8. However, the feasible acceleration factors of above reconstruction methods were often limited to relatively small number by various reconstruction artifacts. In recent years, CNN, an architecture widely used in the field of artificial intelligence (AI), opens a new possibility to solve the inverse problem of MRI reconstruction in an efficient manner. For MRI reconstruction, these approaches typically learn the proper transformation between the input (i.e. zero-filled under-sampled k-space) and target (i.e. the fully-sampled k-space) by minimizing a specific loss-function through a training process. In this study, compared with the conventional MBH-T2WI, the SBH-T2WI sequence with deep learning-based reconstruction showed promising performance as it provided significantly better image quality and lesion detectability, within a relatively shorter acquisition time.Acknowledgements
No acknowledgement found.References
1. Colli A, Fraquelli M, Casazza G, et al. Accuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic review. American Journal of Gastroenterology. 2006;101(3):513-523.
2. Schreiber-Zinaman J, Rosenkrantz AB. Frequency and reasons for extra sequences in clinical abdominal MRI examinations. Abdominal Radiology. 2017;42(1):306-311.
3. Xiang L, Chen Y, Chang W, et al. Ultra-fast t2-weighted mr reconstruction using complementary t1-weighted information. Paper presented at: International Conference on Medical Image Computing and Computer-Assisted Intervention2018.
4. Cheng JY, Chen F, Pauly JM, Vasanawala SS. Method for performing magnetic resonance imaging reconstruction with unsupervised deep learning. In: Google Patents; 2020.
5. He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. Paper presented at: Proceedings of the IEEE conference on computer vision and pattern recognition2016.
6. Mao X, Li Q, Xie H, Lau RY, Wang Z, Paul Smolley S. Least squares generative adversarial networks. Paper presented at: Proceedings of the IEEE international conference on computer vision2017. 7. Yu JS, Kim KW, Kim YH, Jeong EK, Chien D. Comparison of multishot turbo spin echo and HASTE sequences for T2‐weighted MRI of liver lesions. Journal of Magnetic Resonance Imaging. 1998;8(5):1079-1084.
8. Yoon JK, Kim M-J, Lee S. Compressed sensing and parallel imaging for double hepatic arterial phase acquisition in gadoxetate-enhanced dynamic liver magnetic resonance imaging. Investigative radiology. 2019;54(6):374-382.
Figures