2986
FAST 3D vs. Compressed Sensing vs. Parallel Imaging: Image Quality Improvement on MRCP with and without Deep Learning Reconstruction1Radiology, Fujita Health University School of Medicine, Toyoake, Japan, 2Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University School of Medicine, Toyoake, Japan, 3Canon Medical Systems Corporation, Otawara, Japan, 4Radiology, Fujita Health University Hospital, Toyoake, Japan
Synopsis
We hypothesize that the newly developed FAST 3D can reduce examination time as well as Compressed SPEEDER and obtain MRCP without any degradation of image quality as compared with conventional parallel imaging technique in patients with hepatobiliary and pancreatic diseases. In addition, deep learning reconstruction (i.e.AiCE) has a potential to improve image quality of MRCP obtained by different protocols in routine clinical practice. The purpose of this study was to compare the capability of image quality improvement on MRCP with and without AiCE among FAST 3D, Compressed SPEEDER and conventional parallel imaging (SPEEDER) in patients with hepatobiliary and pancreatic diseases.
Introduction
Magnetic resonance cholangiopancreatography (MRCP) uses as a powerful tool for evaluating the liver, gallbladder, bile ducts, pancreas and pancreatic duct in various hepatobiliary and pancreatic diseases (1, 2). It is noninvasive and suggested as useful for not only morphological, but also functional evaluation in routine clinical practice. MRCP is usually obtained by 2D or 3D turbo spin-echo sequences with and without breath-holding. However, MRCP obtained with breath-holding is suggested as degradation of image quality. Recently, compressed sensing (Compressed SPEEDER) is introduced by Canon Medical Systems for reducing examination time without degradation of image quality (3). In addition, newly developed Fast 3D mode (FAST 3D) technique, which is one of the techniques for k-space based acceleration technique and applied with parallel imaging, is also introduced in routine clinical practice. Moreover, deep learning reconstruction (DLR) method, so called Advanced intelligent Clear-IQ Engine (AiCE), has a potential to improve image quality of MRI obtained by different protocols (3-4). However, no reports have been published for demonstrating the utility of FAST 3D and DLR for MRCP in various hepatobiliary and pancreatic diseases. We hypothesize that the newly developed FAST 3D can reduce examination time as well as Compressed SPEEDER and obtain MRCP without any degradation of image quality as compared with conventional parallel imaging technique in patients with hepatobiliary and pancreatic diseases. In addition, AiCE has a potential to improve image quality of MRCP obtained by different protocols in routine clinical practice. The purpose of this study was to compare the capability of image quality improvement on MRCP with and without AiCE among FAST 3D, Compressed SPEEDER and conventional parallel imaging (SPEEDER) in patients with hepatobiliary and pancreatic diseases.Materials and Methods
This study included 42 patients (17 men, 15 women; mean age: 68 years;) with hepatobiliary and pancreatic diseases underwent MRCP by FAST 3D, Compressed SPEEDER and conventional SPEEDER techniques and reconstructed with and without newly developed DLR method (AiCE). For quantitative image quality assessment, percentage of coefficient of variations (%CVs) and contrast ratios (CRs) with liver at gallbladder (GB), common biliary duct (CBD) and main pancreatic duct (MPD) were calculated by ROI measurement. To qualitatively evaluate image qualities, overall image quality, lesion depiction and diagnostic confidence level were assessed by 5-point scoring system by two investigators with 7 and 27-year experiences, and each final score was determined by consensus of two readers. To determine the capability for quantitative image quality improvement, %CV and CR at each region were compared among all MRCP obtained by FAST 3D (MRCPFAST 3D), Compressed SPEEDER (MRCPCompressed SPEEDER) and conventional SPEEDER (MRCPconventional SPEEDER) with and without AiCE by Tukey’s HSD test. For comparison of each qualitative index, overall image quality, lesion depiction and diagnostic confidence level were also compared by Wilcoxon signed–rank test. A p value less than 0.05 was considered as significant at each statistical analysis.Results
Representative case is shown in Figure 1. Compared results of %CV and CR are shown in Figure 2 and 3. Whether AiCE was applied or not, mean examination times of MRCPFAST 3D and MRCPCompressed SPEEDER were significantly shorter than that of MRCPconventional SPEEDER (p<0.05). At liver, %CV of MRCPconventional SPEEDR with AiCE was significantly higher than that of MRCPFAST 3D and MRCPCompressed SPEEDER with AiCE (p<0.05). When compared at CBD and pancreas, CRs of MRCPCompressed SPEEDER with AiCE were significantly higher than those of MRCPFAST 3D or MRCPconventioal SPEEDER with AiCE (p<0.05). Interobserver agreements and qualitative index comparison results among all methods are shown in Figure 4. Interobserver agreement on each method was determined as moderate or substantial (0.44≤κ≤0.77). When applied AiCE, overall image quality, lesion detection or diagnostic confidence level on MRCP obtained by each technique and reconstructed with AiCE were significantly higher than those without AiCE (p<0.05). When compared each index, MRCPCompressed SPEEDER with and without AiCE were significantly lower than MRCPFAST 3D or MRCPconventional SPEEDER with and without AiCE (p<0.05).Conclusion
Newly developed DLR method (AiCE) can significantly improve image quality of MRCP at all protocols. Image quality of FAST 3D is generally superior to that of Compressed SPEEDER, and considered as compatible with conventional SPEEDR on MRCP, although lesion depiction and diagnostic confidence level have no significant difference among all acquisition methods.Acknowledgements
This study was financially and technically supported by Canon Medical Systems Corporation.References
- Welle CL, Miller FH, Yeh BM. Advances in MR Imaging of the Biliary Tract. Magn Reson Imaging Clin N Am. 2020; 28(3):341-352.
- Harrington KA, Shukla-Dave A, Paudyal R, Do RKG. MRI of the Pancreas. J Magn Reson Imaging. 2020 Apr 17. doi: 10.1002/jmri.27148. Online ahead of print.
- Ueda T, Ohno Y, Yamamoto K, et al. Compressed Sensing and Deep Learning Reconstruction for Women’s Pelvic MRI Denoising: Utility for Improving Image Quality and Examination Time in Routine Clinical Practice. Eur J Radiol. 2020 (in press)
- Kidoh M, Shinoda K, Kitajima M, et al. Deep Learning Based Noise Reduction for Brain MR Imaging: Tests on Phantoms and Healthy Volunteers. Magn Reson Med Sci. 2020; 19(3): 195-206.
Figures
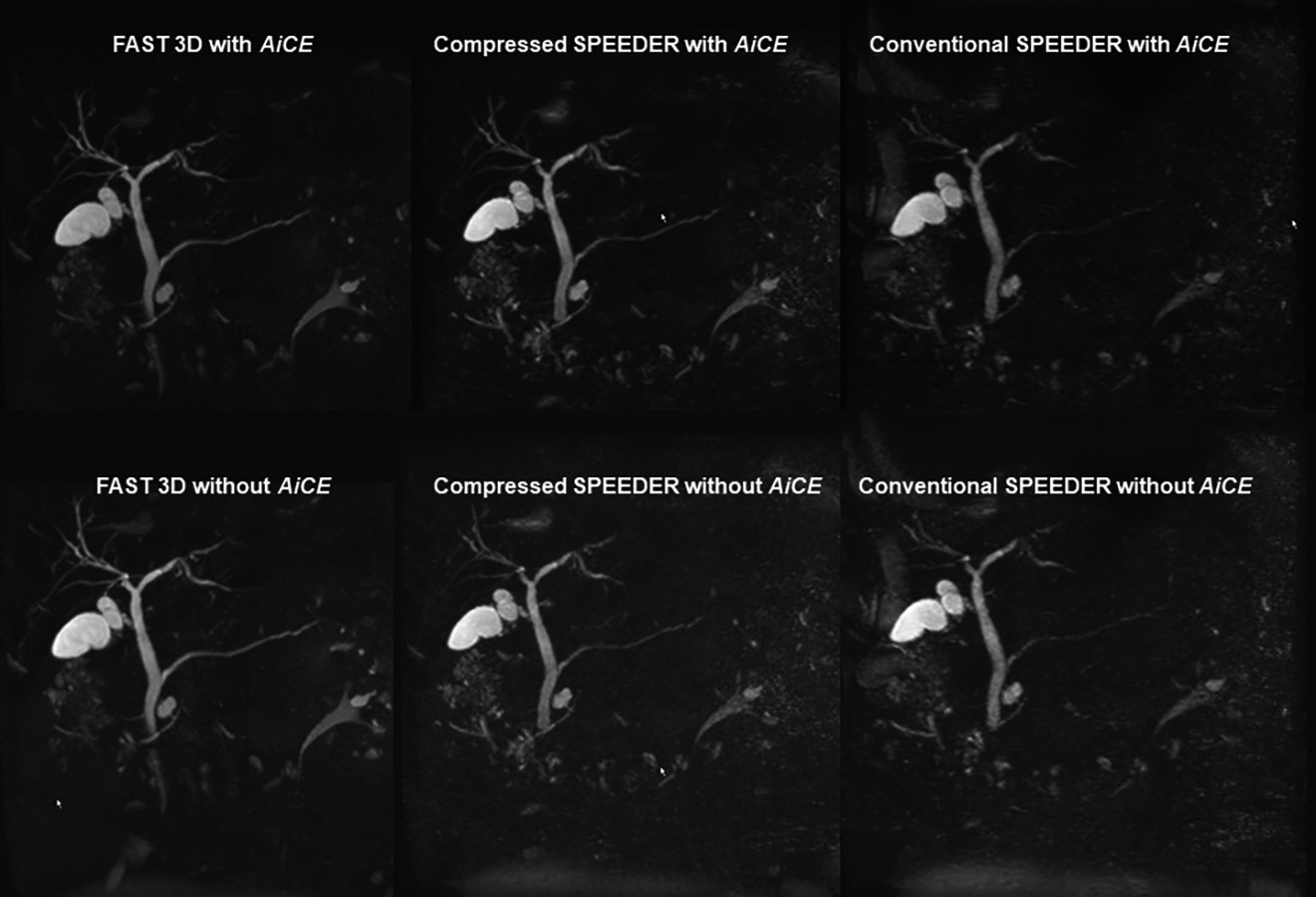
Figure 1. 71-year old patient with intraductal papillary mucinous neoplasm. (First line from L to R: MRCPFAST 3D with AiCE, MRCPCompressed SPEEDER with AiCE and MRCPconventional SPEEDER with AiCE; second line from L to R: MRCPFAST 3D without AiCE, MRCPCompressed SPEEDER without AiCE and MRCPconventional SPEEDER without AiCE).
MRCPFAST 3D and MRCPconventional SPEEDER more clearly depict intrahepatic bile duct as well as main pancreatic duct than MRCPCompressed SPEEDER, when applied AiCE or not. In addition, AiCE was able to improve image quality of MRCP obtained by each technique.
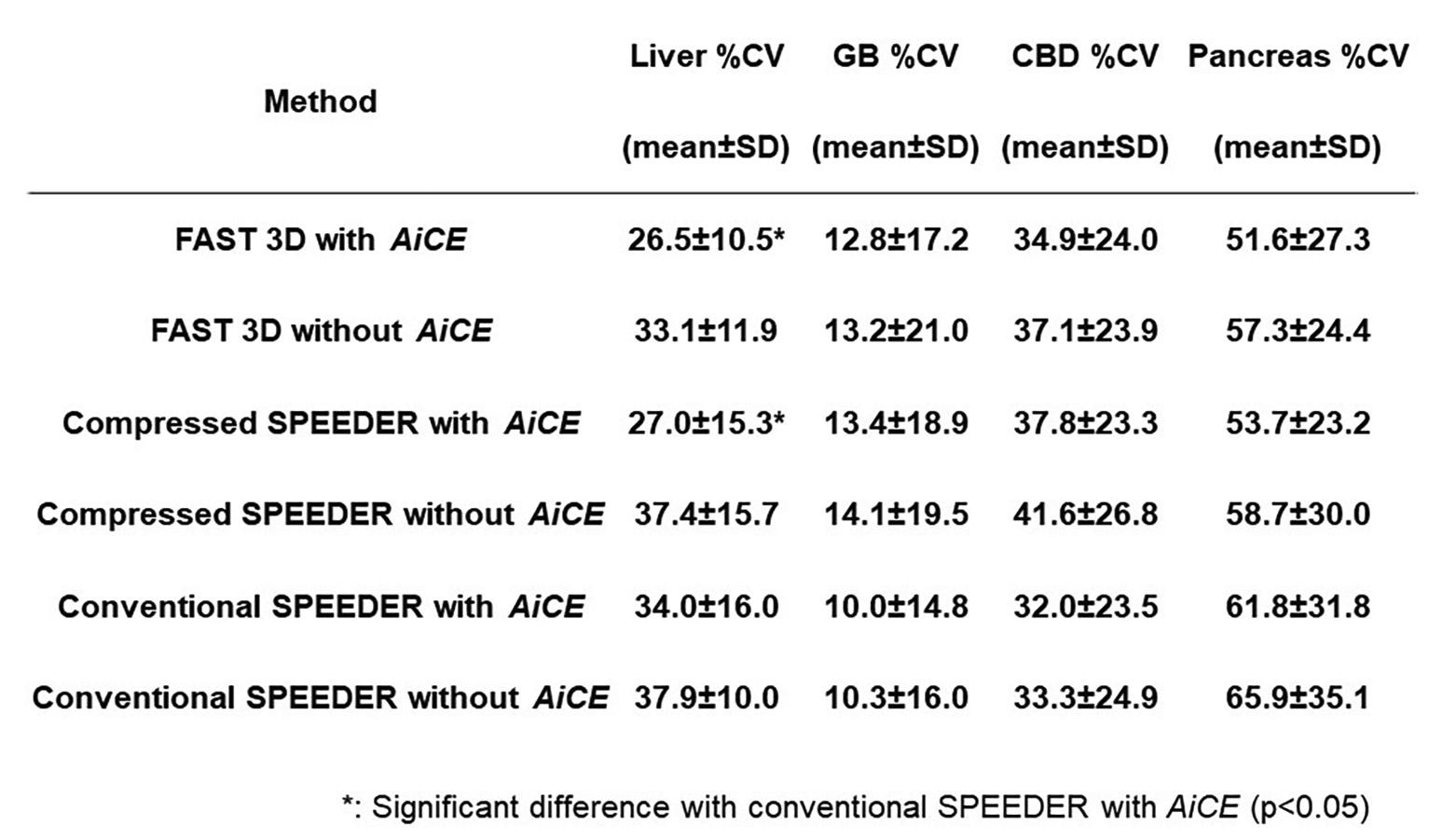
Figure 2. Compared results of %CV in liver, galbladder, comon bile duct and pancreas.
%CV of MRCPconventional SPEEDER with AiCE was significantly higher than that of MRCPFAST 3D and MRCPCompressed SPEEDER with AiCE (p<0.05).
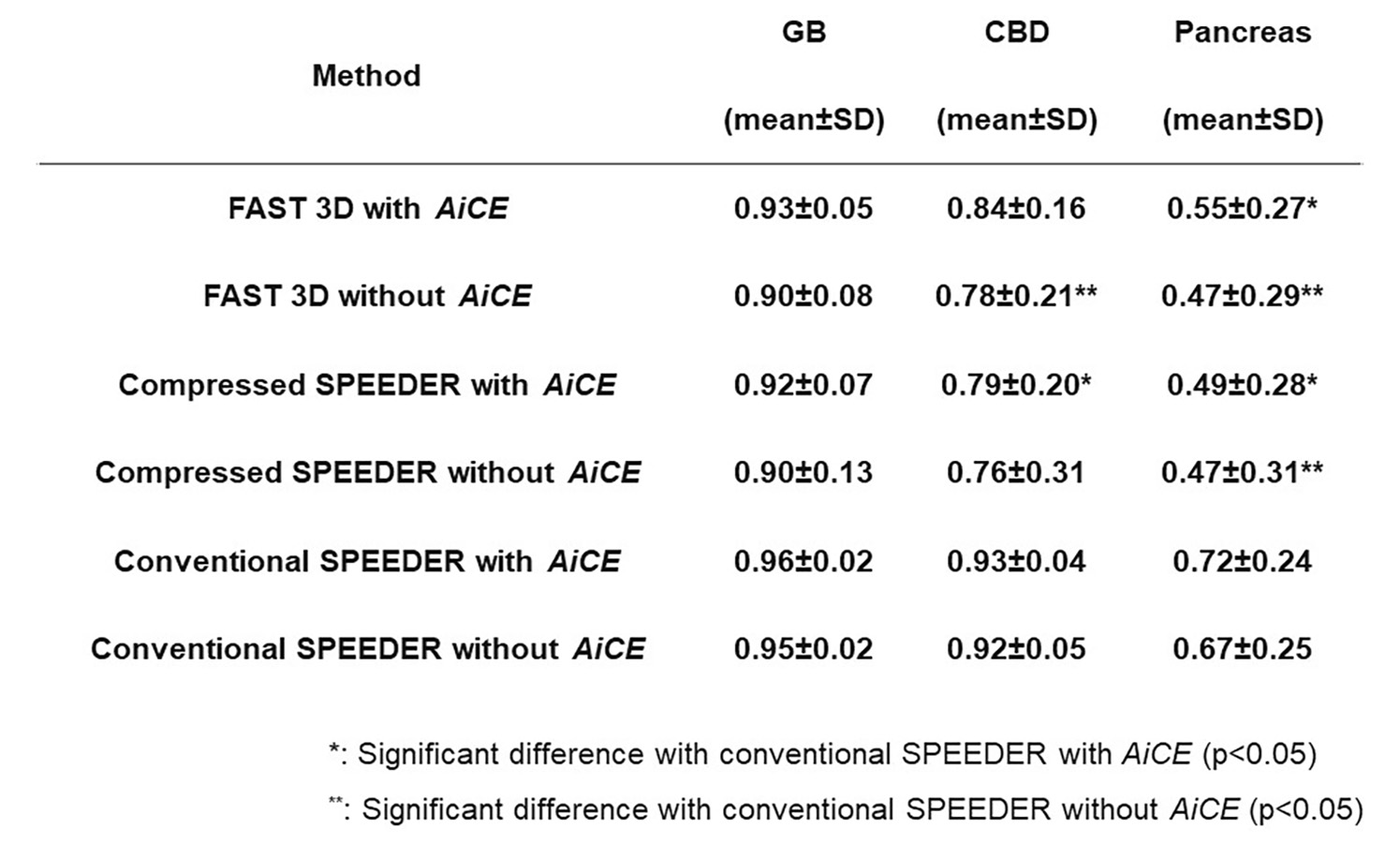
Figure 3. Compared results of CR in galbladder, comon bile duct and pancreas.
CRs at CBD and pancreas of MRCPconventional SPEEDER with AiCE were significantly higher than that of MRCPFAST 3D or MRCPCompressed SPEEDER with AiCE (p<0.05). In addition, CRs at CBD and pancreas of MRCPconventional SPEEDER without AiCE were significantly higher than that of MRCPFAST 3D or MRCPCompressed SPEEDER without AiCE (p<0.05).
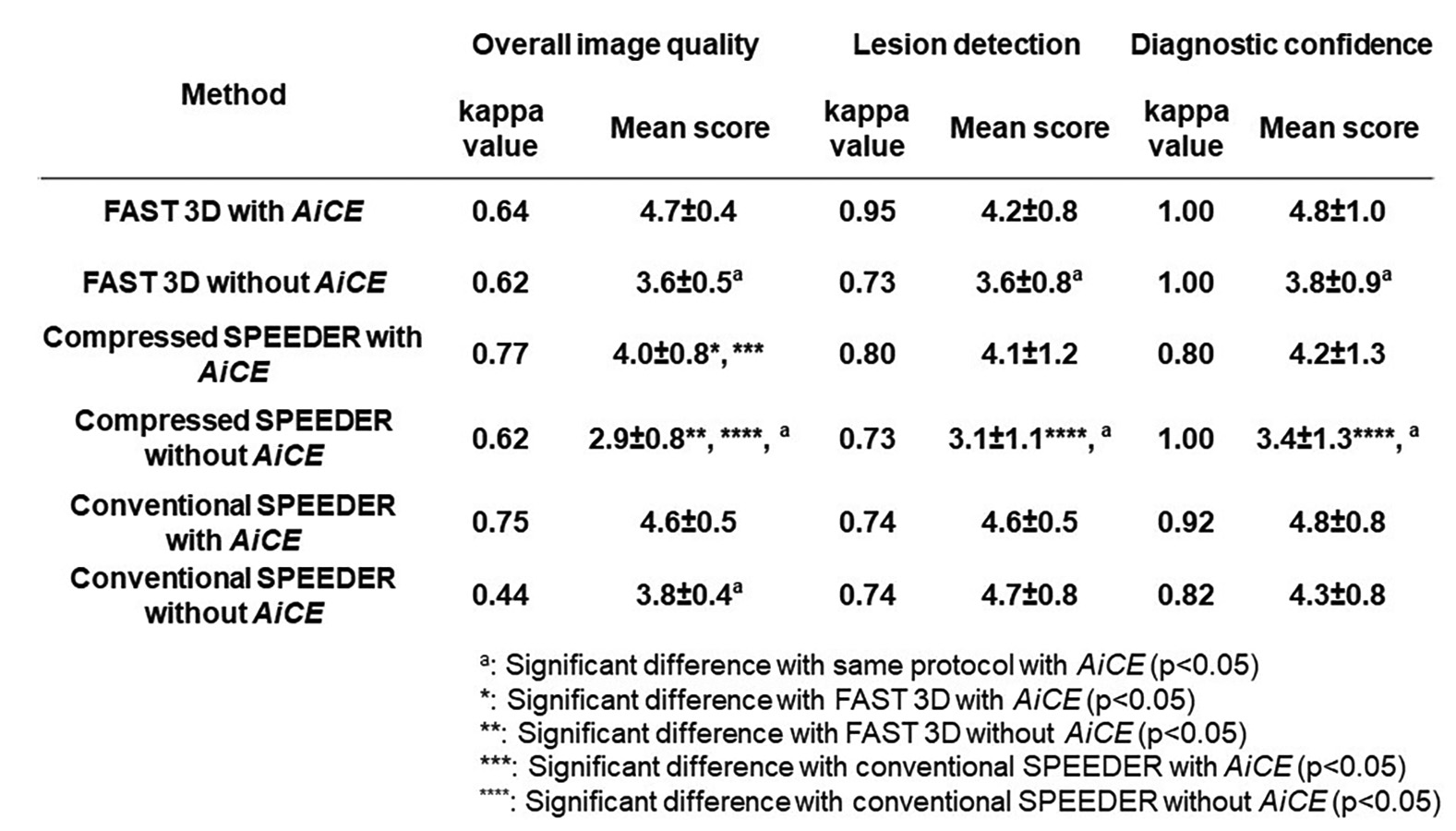
Figure 4. Compared results of interobserver agreement and qualitative image qualities among all methods.
Interobserver agreement on each method was ranged between 0.44 and 0.77. When applied AiCE, each index on MRCP obtained by each technique and reconstructed with AiCE were significantly higher than those without AiCE (p<0.05). On each index, MRCPCompressed SPEEDER with and without AiCE were significantly lower than MRCPFAST 3D or MRCPconventional SPEEDER with and without AiCE (p<0.05).