2909
Reliability of respiratory-triggered 2D cine kat-ARC for the assessment of biventricular function in patients with repaired tetralogy of Fallot1Iwate Medical University, Yahaba, Japan, 2GE Healthcare, Munich, Germany, 3GE Healthcare, Tokyo, Japan
Synopsis
To assess the image quality, reproducibility, and accuracy of two-dimensional (2D)-cine k-adaptive-t Autocalibrating Reconstruction for Cartesian sampling (2D kat-ARC) for the quantification of biventricular volumes and function compared to 2D balanced steady state free precession (2D SSFP) in patients with repaired tetralogy of Fallot (TOF). In this study, we were able to find good reproducibility of biventricular volumes and ejection fraction (EF) between 2D SSFP and 2D kat-ARC sequences despite some drawbacks including an overestimation of right ventricular (RV) end-systolic volume and an underestimation of RV stroke volume and RVEF compared to 2D SSFP.
INTRODUCTION
The clinical course of repaired TOF patients is dependent on the degree of pulmonary regurgitation and RV dilation, while long-term complications include LV dysfunction. Hence, cardiac magnetic resonance (CMR) parameters of biventricular volumes and function have been identified as predictors of repaired TOF patients. Two-dimensional cine SSFP is the most common approach for the evaluation of volumes and systolic function in clinical practice. SSFP provides intrinsic advantages, especially its superior blood-myocardium contrast owing to blood in-flow effects. However, the conventional 2D cine SSFP sequence requires the suspension of respiration, and there are several factors that may limit the ability of patients to perform consistent breath-holds, such as anxiety, various medical conditions, and age. Recently, kat-ARC was investigated for 3D cine to overcome the technical limitations of 2D SSFP. However, no data is available concerning the reliability of respiratory-triggered 2D cine kat-ARC in clinical practice.This study aimed to assess the image quality, reproducibility, and accuracy of 2Dkat-ARC for the quantification of biventricular volumes and function in patients withrepaired TOF.METHODS
Thirty patients (14 [47%] men, mean age 32.2 ± 13.9 years) with repaired TOF at Iwate Medical University Hospital were performed CMR.All CMR examinations were performed at 1.5 T (SIGNA Artist, GE Healthcare, Waukesha, WI) with a 33-channel phased array receiver coil. Short-axis stack cine images were performed, in random order, in each patient using two different imaging techniques: the conventional 2D SSFP and 2D kat-ARC cine imaging.To estimate inter-observer variability, each operator performed a blinded analysis on randomly rearranged sequences of all patients and one of the two observers repeated the analysis on all patients after at least 1 month. The image quality scores were based on three main criteria: blood-to-myocardial contrast, endocardial edge delineation, and presence of motion artifacts throughout the cardiac cycle. The details of the image quality criteria are described elsewhere.1The endocardial and epicardial contours were automatically traced at end-systoleand end-diastole with manual trace when required. The most basal section was definedas the section in which at least 50% of the border of the lumen was surrounded bymyocardium. The papillary muscles and trabeculations of the RV were included as partof the blood pool.2 Subsequently, left ventricular EDV (LVEDV), LVESV, LV stroke volume (LVSV), LVEF, as well as RVEDV, RVESV, RVSV, and RVEF were calculated by automatically tracing the endocardial contours on short-axis stacks in end-diastole and end-systole for both dataset of sequences according to the Society for Cardiovascular Magnetic Resonance guidelines.3 The time required for imaging acquisition was recorded for both 2D SSFP cine and 2D kat-ARC.RESULTS
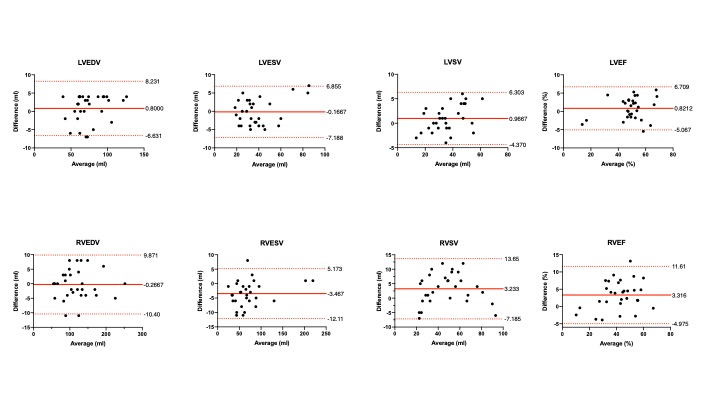
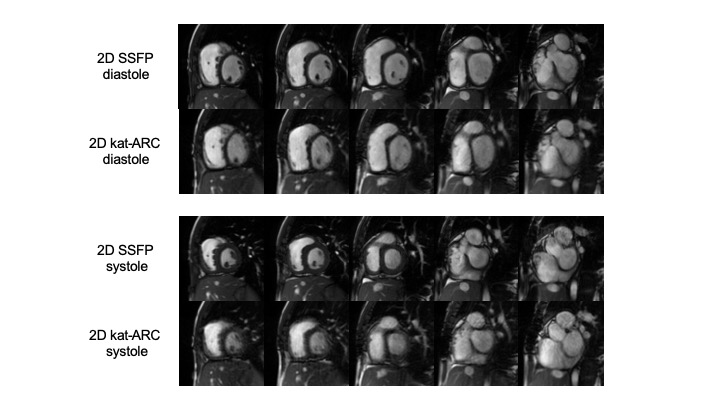
The time of acquisition of the 2D kat-ARC was significantly shorter than that of 2DSSFP (35.2 ± 9.1 sec vs. 80.4 ± 16.7 sec, respectively; p < 0.0001). An analysis of image quality showed significant impairment of the 2D kat-ARC compared with the 2D SSFP with inferior results for blood-to-myocardial contrast, endocardial edge definition, and motion artifacts.The inter-observer variability showed strong correlations for both sequences withthe results of ICC (≥ 0.93) for all measurements of LV and RV. The intraobserver differences were also strongly correlated, with ICC ≥ 0.95.The Bland-Altman plots showed strong agreement between the two sequences (Figure. 1) and the linear regression yielded good agreement between the two techniques (r ≥ 0.95). Compared with 2D SSFP, 2D kat-ARC demonstrated no significant difference interms of biventricular EDV, LVESV, LVSV, and LVEF. However, the RVESV for 2Dkat-ARC was overestimated compared with that for 2D SSFP (2D kat-ARC = 73.8 ±43.2 ml vs. 2D SSFP = 70.3 ± 44.5 ml, respectively; p = 0.0002). The RVSV and RVEF for 2D kat-ARC were underestimated compared with those for 2D SSFP (2D kat-ARC RVSV = 46.2 ± 20.5 ml vs. 2D SSFP = 49.4 ± 20.4 ml, p = 0.0024; 2D kat-ARC RVEF = 40.2 ± 12.7% vs. 2D SSFP = 43.5 ± 14.0%, p = 0.0002). A representative case is shown in Figure 2.DISCUSSION
The RV in this study population was more dilated than the LV. Moreover,delineating the endocardium of the RV is more challenging than the LV owing to agreater proportion of trabeculated myocardium in patients with repaired TOF. In this study, blood-myocardial boundaries were more blurred in the 2D kat-ARC sequence. Therefore, the boundary lines at end-systole might be located outside the trabecular layer, which would give a slightly larger end-systolic volume in the 2D kat-ARC sequence in this study. Even though the difference in the values of RVESV and RVSV were within 5 ml, and RVEF was within 5% between two sequences, we should consider this technical limitation when tracing the RV boundary at end-systole in patients with repaired TOF.CONCLUSION
This study demonstrates that respiratory-triggered 2D kat-ARC cine is a reliable andreproducible technique that could be used in the evaluation of biventricular volumes andfunction. However, the RVESV was overestimated and the RVSV and RVEF wereunderestimated using 2D kat-ARC compared with those using conventional breath-hold2D cine SSFP.Acknowledgements
No acknowledgement found.References
1. Pednekar AS, Wang H, Flamm S, et al. Two center clinical validation and quantitative assessment of respiratory triggered retrospectively cardiac gated balanced-SSFP cine cardiovascular magnetic resonance imaging in adults. J Cardiovasc Magn Reson 2018; 20: 44.
2. Petersen SE, Aung N, Sanghvi MM, et al. Reference ranges for cardiac structure and function using cardiovascular magnetic resonance(CMR) in Caucasians from the UK Biobank population cohort. J Cardiovasc Magn Reson 2017; 19: 18.
3. Christopher M. Kramer, Jörg Barkhausen, et al. Standardized Cardiovascular Magnetic Resonance Imaging (CMR) Protocols: 2020 Update. J. Cardiovasc Magn Reson 2020; 22: 17.
Figures