2903
Double breath-hold whole heart cine cardiac MR imaging using a new 72-channel local receive array1Biomedical Engineering & Physics, Amsterdam UMC, Amsterdam, Netherlands, 2Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 3Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 4Radiology, Leiden University Medical Center, Leiden, Netherlands, 5Cardiology, Amsterdam UMC, Amsterdam, Netherlands
Synopsis
Currently, a standard short-axis cardiac CINE protocol consists of ~7 breath-holds which is time-consuming, costly and patient-unfriendly. We investigated whether it is feasible to accurately quantify biventricular morphology and function in 3 to 2 breath-holds using a new 72‑channel receive array and (compressed-)SENSE acceleration. To that end, we performed a comparison between a 16 channel local array with a SENSE-factor 2 and the new coil with (compressed‑) SENSE factors of 2, 4 and 6. In all cases, left ventricular ejection fractions were similar with acceptable image quality decline for higher acceleration, facilitating cardiac function assessment in only 2 breath-holds.
INTRODUCTION
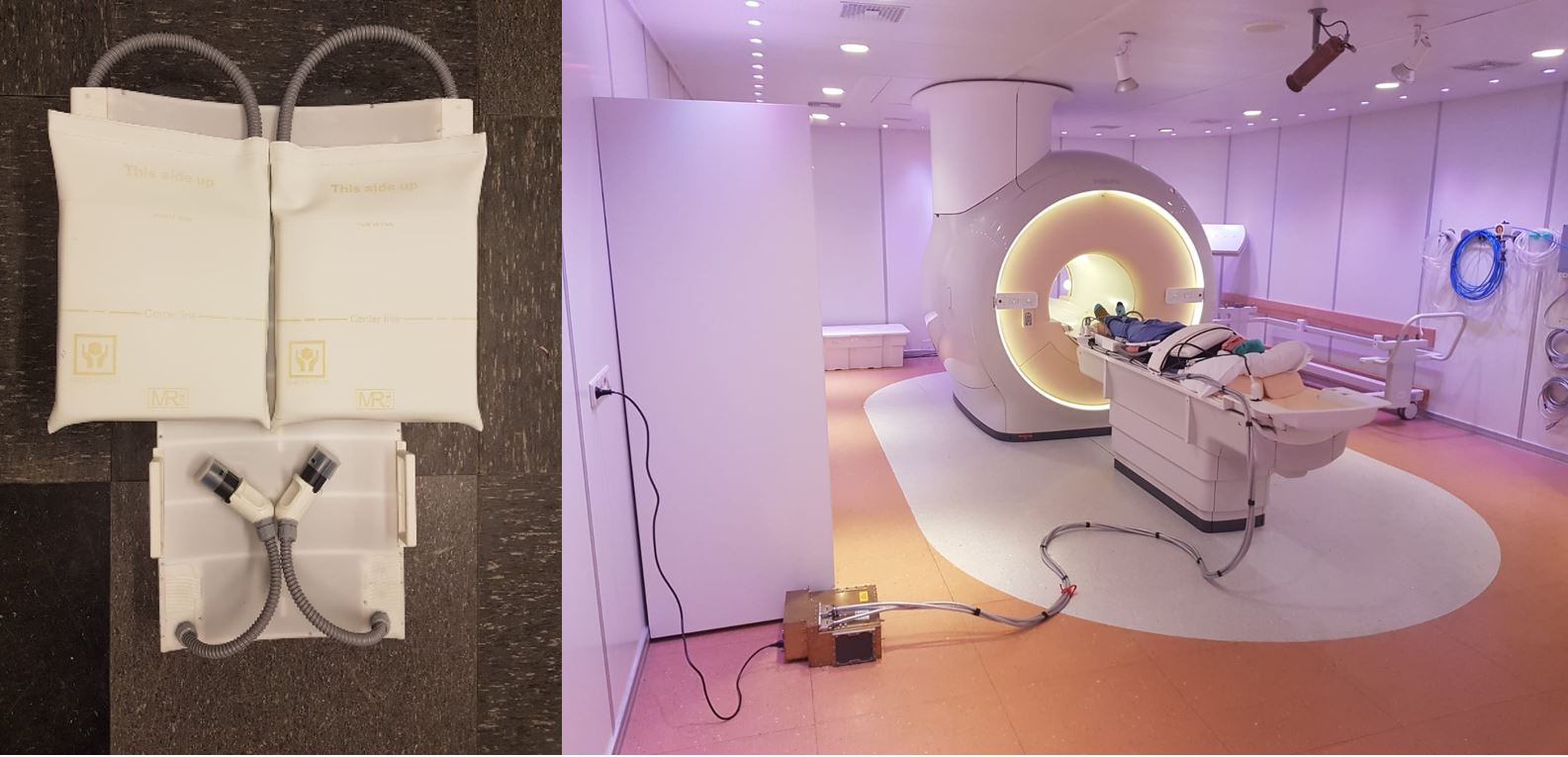
Cardiovascular Magnetic Resonance (CMR) imaging is considered the gold standard for assessment of biventricular function and morphology. Clinically, a typical short-axis (SAx) CINE protocol consists of a retrospectively cardiac gated two-dimensional segmented k-space cine balanced steady state free precession (bSSFP) sequence(1). The advantage of bSSFP is that it provides superior blood pool to myocardium contrast with a high signal-to-noise ratio (SNR) facilitating accurate delineations of the left and right ventricular endo- and epicardial borders, wall trabeculation and papillary muscles. In routine clinical practice a stack of 14 2D SAx slices is acquired covering the whole heart from base to apex and covering the full cardiac cycle. The acquisition is segmented over multiple breath-holds to minimize respiratory-motion artefacts. With SENSE 2 parallel imaging, typically 2 slices can be acquired per breath-hold of approximately 12 seconds each, totaling about 7 breath-holds. Performing multiple breath-holds can be problematic for some patients (e.g. heart failure) and motion-related artefacts are therefore not uncommon (2). Higher acceleration factor could be facilitated by higher parallel imaging factors requiring a receiver coil with increased number of receiver coils (3-6). Here, we performed a comparison between a 16 channel local array with SENSE 2 and a recently developed 72-channel receiver array(7) with (compressed‑)SENSE (C-SENSE) factors of 2, 4 and 6, facilitating heart-covering CINE imaging with as low as 2 breath-holds.METHODS
8 healthy subjects (5 female), aged 31 ± 8 years, body weight 73 ± 10 kg, heart rate 59 ± 11 beats/min were included with writtenly acquired informed consents. CMR examinations were performed with a 3T MR scanner (Ingenia, Philips Healthcare, Best, The Netherlands). Whole-heart SAx cine bSSFP images were acquired using ECG-gating. Firstly, cine SAx acquisitions were acquired with a standard 16-channel coil and SENSE=2 requiring 7 breath-holds. Subsequently, the subjects were repositioned in the scanner with the 72-channel receiver coil and cine SAx acquisitions were repeated with SENSE acceleration factors of 4 (3 breath-holds), 6 (2 breath-holds) and C-SENSE=2 (7 breath-holds), 4 (3 breath-holds), and 6 (2 breath-holds) (Figure 1). The standard 12-element posterior coil array integrated in the patient table was used during all acquisitions. Imaging parameters were: Field-of-View (FOV): 350 x 350, repetition time (TR) ms/echo time (TE) ms, 2.8–3.1/1.40–1.70; flip angle (FA), 45°; slice thickness 8 mm (0.5 mm slice gap); acquired temporal resolution, 37-40 ms. Volumetric quantifications were done using Medis Suite 3.1 (Medis Medical Imaging Systems, Leiden, The Netherlands). Quantitative analysis was performed by a single reviewer, supervised by an experienced cardiologist (15+ years) specialized in cardiac imaging. Quantitative variables included left and right ventricular volumes and LV masses in end-diastole and systole. In this abstract we will focus on left ventricular ejection fraction (LVEF), but similar analyses were performed for a range of functional parameters (including volumes, cardiac output). Bland-Altman analyses and two-sided paired t-tests were performed between 16-channel SENSE=2 acquisitions and the accelerated protocols with the 72-channel coil. A sigmoid-curve was fitted to the signal intensity at the blood-pool – septum interface to quantify image sharpness (width of the sigmoid curve) and blood-to-myocardium contrast (BMC). Visual expert scoring of all slices, graded on a scale of 1 to 5 (1 = nondiagnostic, 2 = suboptimal, 3 = adequate, 4 = good, 5 = excellent) were performed by the cardiologist with focus on endocardial edge delineation (EED) and presence of artefacts. All statistical analyses were performed using R (v. 4.0.3) and Rstudio (v. 1.3.959). P-values of < 0.05 were considered significant.RESULTS
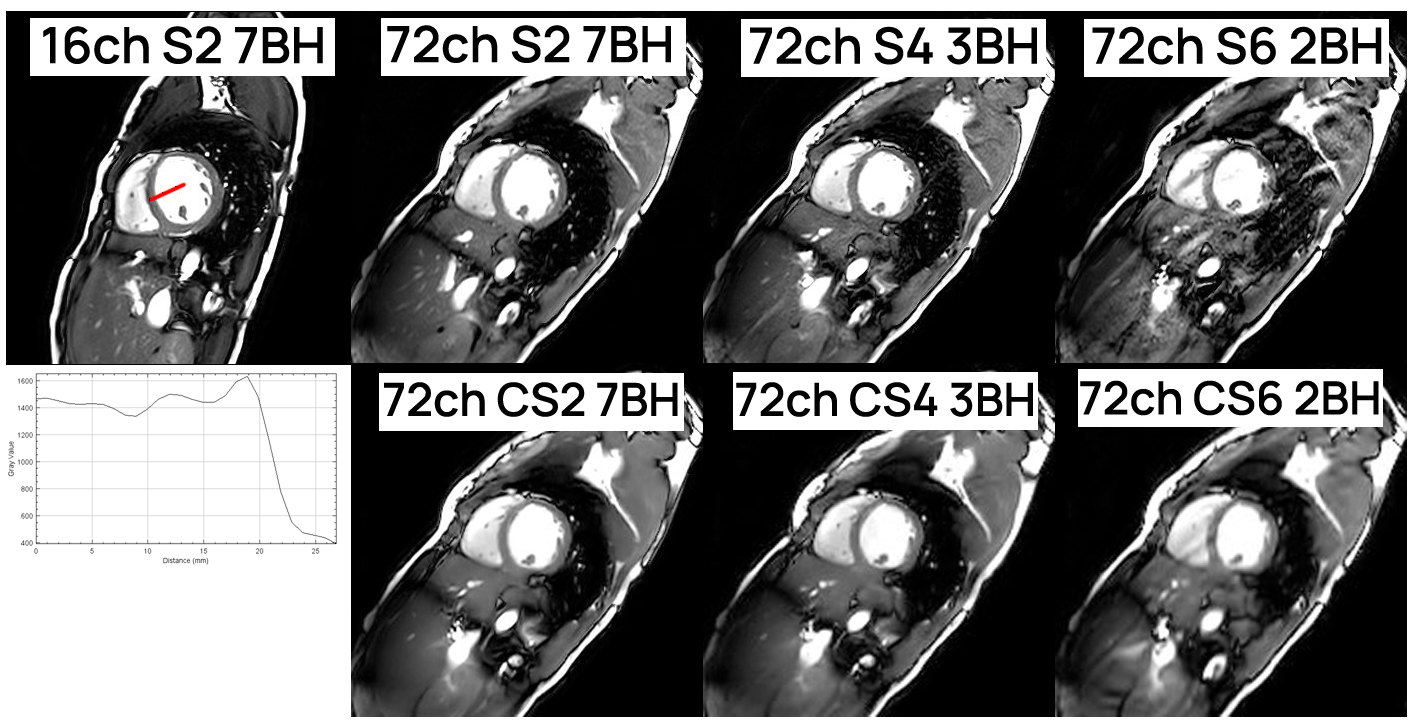
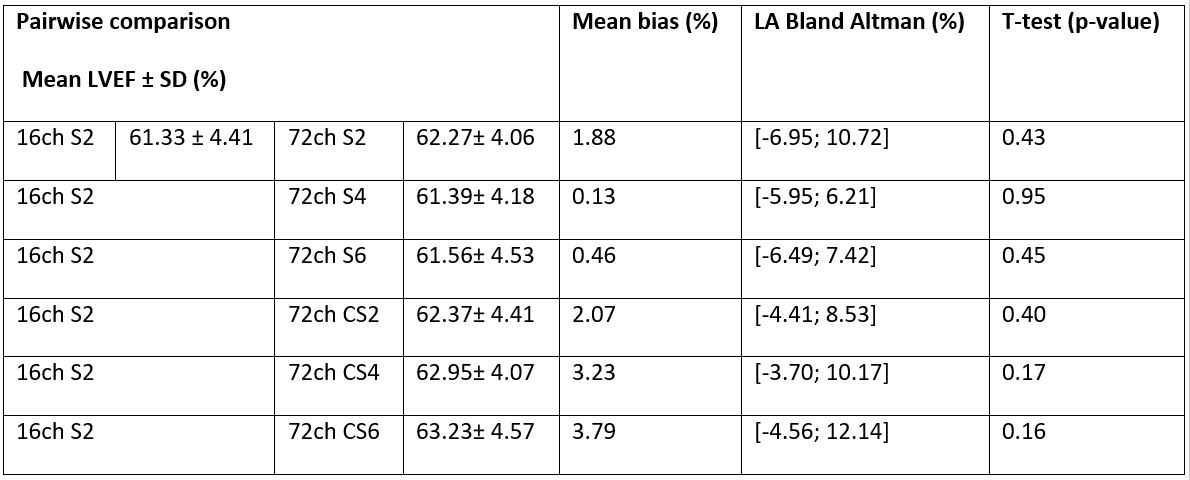
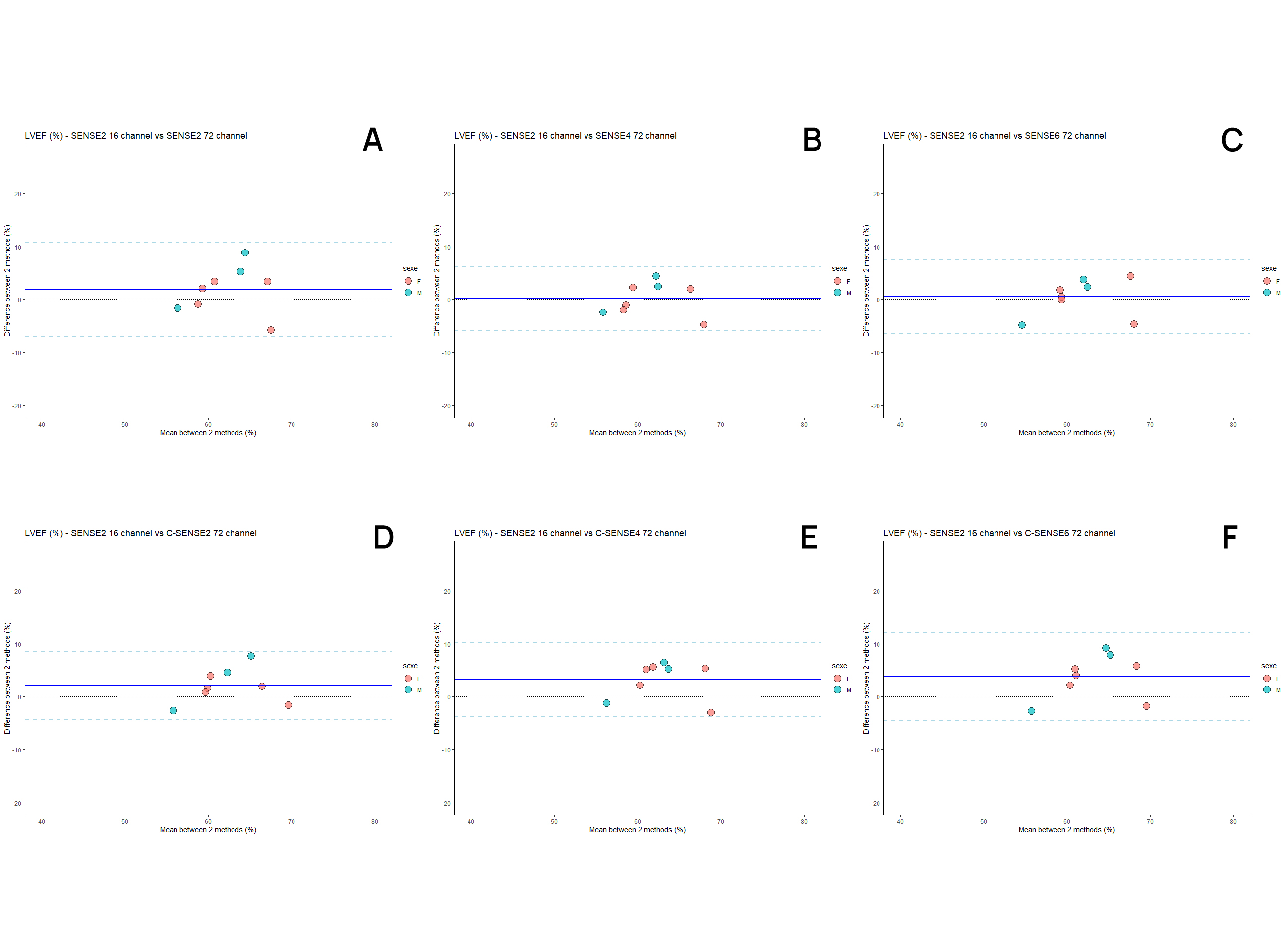
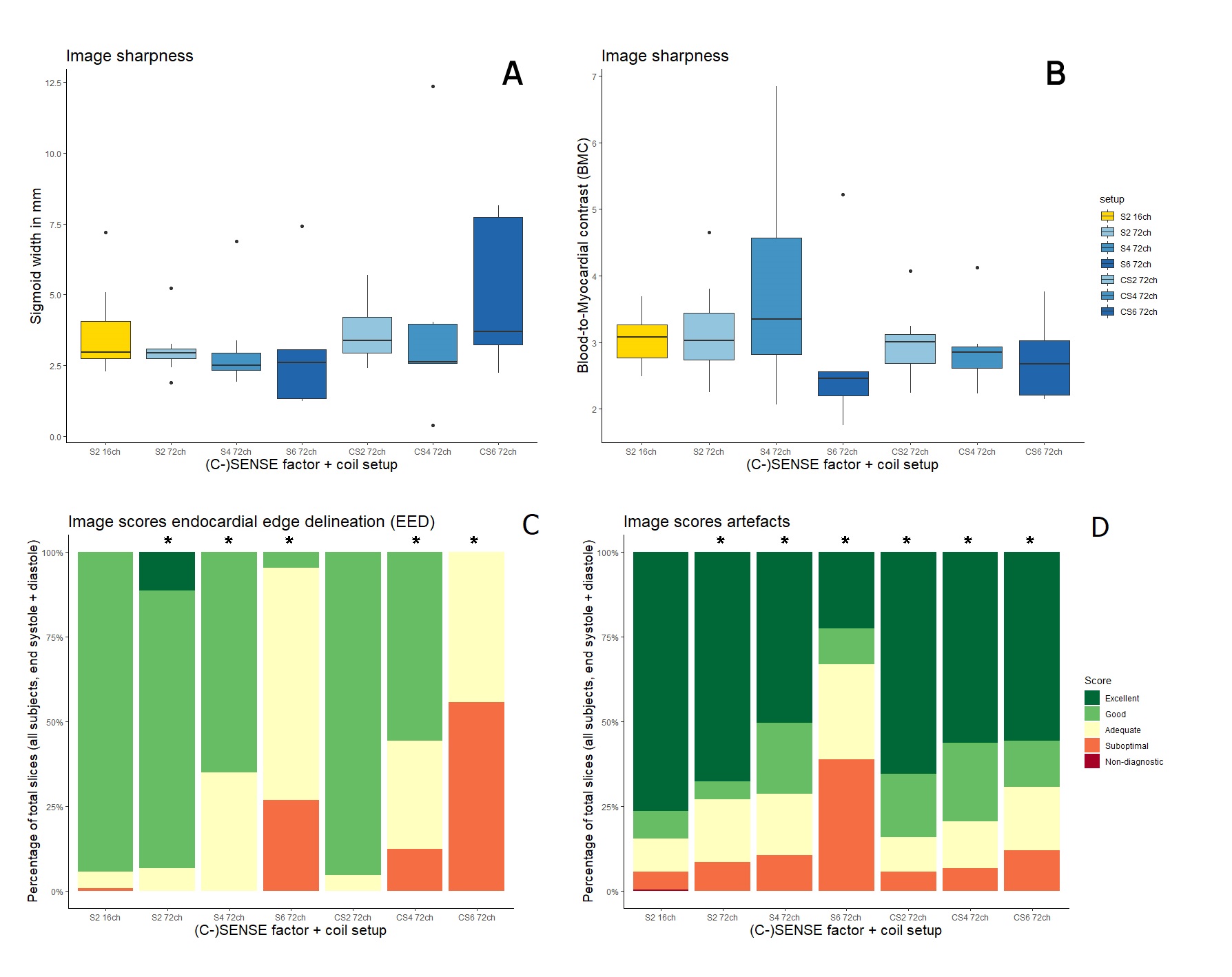
Figure 2 shows mid-ventricular single slices acquired with both setups (16ch, 72ch) and various (C-)SENSE factors 2, 4 and 6. No differences (Table 1) were found in LVEF compared to the reference 16 channel local array SENSE 2 setup (61.33 ± 4.41%), although an overestimating trend is visible with increasing C-SENSE factors according to the Bland-Altman mean bias (C-SENSE 4: 3.23 [-3.70; 10.17], C-SENSE 6: 3.79 [-4.56; 12.14] (Figure 3). Image sharpness was not significantly different (Figure 4), though a declining BMC trend was visible in C-SENSE. The qualitative scores in all slices of EED where significant decreasing from the reference 16 channel local array SENSE 2 setup except for 72 channel C-SENSE 2. Expert quality scores of artifacts were gradually decreasing from the reference 16 channel local array SENSE 2 setup with increasing acceleration.DISCUSSION
LVEF determined from accelerated acquisitions with SENSE and C-SENSE factors up to 6 were similar to conventionally acquired reference values. Image quality (EED and artifacts) decreased progressively with increasing acceleration; however none of the images were graded as suboptimal or lower in EED. Taken together, (C-)SENSE 4 and 6 with the new 72 channel local array seems usable from a quantitative perspective, but qualitatively the EED and artifacts are somewhat comprised. Our next step is to investigate whether free-breathing cardiac CINE imaging is possible with currently investigated (C )SENSE factors and the new 72-channel receive array.CONCLUSION
Quantification of biventricular morphology and function is feasible in just 3 breath holds using SENSE 4 without comprising image quality (EED and artifacts) using a new 72-channel receive array. (C-)SENSE 4 and 6 remain usable at the expense of somewhat compromised image quality (EED and artifacts).Acknowledgements
No acknowledgement found.References
1. Scheffler K, Lehnhardt S. Principles and applications of balanced SSFP techniques. European Radiology. 2003;13(11):2409-18.
2. Saeed M, Van TA, Krug R, Hetts SW, Wilson MW. Cardiac MR imaging: current status and future direction. Cardiovasc Diagn Ther. 2015;5(4):290-310.
3. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952-62.
4. Schmitt M, Potthast A, Sosnovik DE, Polimeni JR, Wiggins GC, Triantafyllou C, et al. A 128-channel receive-only cardiac coil for highly accelerated cardiac MRI at 3 tesla. Magnetic Resonance in Medicine. 2008;59(6):1431-9.
5. Hardy CJ, Giaquinto RO, Piel JE, Rohling KW, Marinelli L, Blezek DJ, et al. 128-channel body MRI with a flexible high-density receiver-coil array. J Magn Reson Imaging. 2008;28(5):1219-25.
6.Gruber B, Froeling M, Leiner T, Klomp DWJ. RF coils: A practical guide for nonphysicists. J Magn Reson Imaging. 2018.
7. Gosselink M, Klarenberg, H., Lamb, H.J., Strijkers, G.J., Leiner, T., Klomp, D.W.J., Froeling, M. Highly accelerated cardiac imaging using a high-density 72 channel local receiver array at 3 Tesla. ISMRM 2019. 2019.
Figures