2895
Title: 3T contrast-enhanced coronary magnetic resonance angiography in the assessment of myocardial hyperemia in acute myocarditis.1Radiology, Union Hospital, School of Medical Technology and Engineering, Fujian Medical University, Fuzhou, China, 2Diagnostic imaging, Siemens Healthcare, Shanghai, China., Shanghai, China, 3Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China., Shenzhen, China
Synopsis
this study demonstrated the feasibility of CE-CMRA for detection of myocardial hyperemia in patients with suspected acute myocarditis. Furthermore, this approach could serve as a helpful supplementary tool to assess coronary artery significant stenosis. The results of the present study suggested that CE-CMRA may potentially improve accuracy of evaluating the original Lake Louise Criteria to identify acute myocarditis in combination with T2-STIR and LGE imaging.
Introduction
Acute myocarditis (AM) is most frequently triggered by acute viral infection, causing sudden cardiac deaths in young adults older than 40 years and dilated cardiomyopathy (3). Endomyocardial biopsy is considered as the gold standard for the diagnosis of myocarditis. However, this is not routinely performed in clinical practices due to its invasiveness and possible sampling errors (7). Recently, cardiac magnetic resonance (CMR) has become the primary tool for diagnosing myocarditis. In 2009, the Lake Louise Criteria (LLC) proposed that myocardial edema, hyperemia, and necrosis in patients with suspected myocarditis could be detected using T2-weighted, early gadolinium enhancement, and late gadolinium enhancement (LGE) imaging (8). A major drawback of early gadolinium enhancement ratio (EGER) technique with T1-FSE pulse sequences is that the image quality may be affected or even be non-diagnostic due to motion artifacts.Contrast-enhanced whole-heart coronary magnetic resonance angiography (CE WH-CMRA) at 3T using a fast low-angle shot (FLASH) sequence was introduced to detect coronary artery stenosis in approximately 10 min, and contrast-enhanced whole-heart coronary magnetic resonance angiography has the potential to detect experimentally induced myocardial hyperemia in participants with acute myocarditis. So far, there is no research focusing on the detection of myocardial hyperemia in patients with acute myocarditis by using CE-CMRA. Thus, the purpose of this study was to assess the value of the CE-CMRA in the diagnosis of acute myocarditis.
Method
Methods: Between March 2018 and July 2020, according to the diagnostic criteria by the European Society of Cardiology, a total number of 31 patients with clinically suspected acute myocarditis were prospectively recruited in this study. Cardiac MRI was performed with a 3T MR system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) using an 18-channel body matrix coil. The R-wave acquired from a 3-lead wireless vectorcardiogram was used to trigger the data acquisition.The acquisition sequences included: 1.Myocardial edema was evaluated using a breath-hold, black-blood, T2-weighted triple inversion-recovery sequence acquired in 4-chamber long-axis and short-axis orientations before contrast media application using the following parameters: FOV 340 cm, TR 800ms, TE 44 ms, TI 160 ms, matrix256x 256, slice thickness 8 mm. 2.reath-hold SSFP cine images were acquired for cardiac function in a standard manner (short axis, two chamber and four chamber views) with the following °flip angle 80°, matrix256x 256, slice thickness 8 mm. 3.Detection of inflammation-induced myocardial hyperemia was performed using a prospective navigator-gated, ECG-triggered, fat-saturated, inversion recovery-prepared, segmented, three-dimensional FLASH sequence with slow infusion of 0.2mmol/kg body weight of Gadobenate dimeglumine at a rate of 0.3 ml/s, immediately followed by 15 ml saline given at the same rate. Data acquisition began 60s after the initialization of contrast agent administration. The imaging parameters were TR 320 ms, TE 1.4 ms, flip angle 20°, matrix 256 x 256, FOV 220 x 330 mm2, acquired voxel size = 1.3 x1.3x 1.8 mm3 and interpolated to 0.65 x 0.65 x 0.9 mm3, readout bandwidth= 610 Hz/pixel, acceleration factor=2, Non-selective inversion recovery pulse was used to suppress background tissue (TI = 200 ms). 4. Late gadolinium enhancement (LGE) images for the assessment of myocardial necrosis were obtained by using a 2D phase-sensitive inversion-recovery (PSIR) gradient-echo pulse sequence after gadolinium injection (10 to 15 min) in 4-chamber, 2-chamber, and short-axis views covering the entire LV myocardium. The following parameters were used: FOV 350x350 mm, slice thickness 8 mm, 20% gap between each slice, TR 750 ms, TE 1.55, acquisition matrix 256x256. The inversion time was optimized in order to nullify the signal from normal myocardium (TI = 250-400 ms, decided by TI scout).
The myocardial involvement region showing high signal intensity visualized on CE-CMRA and LGE images were compared and the corresponding areas were analyzed using Wilcoxon signed rank sum test.
Results and Disscussion
Results: The final population included 31 patients. The acquisition time of contrast-enhanced CMRA was 8.0±1.3 min. 203 myocardial involvement (MI) segments were detected in CE-CMRA sequence and 182 MI segments were found in 2D LGE images. The volume of the largest myocardial lesions for CE-CMRA were significantly larger than those for 2D-LGE (5.7±3.4 cm3 versus 4.1±2.5cm3; P<0.001).The results of the present study showed the CE-CMRA could detect more the segmental myocardial involvement than T2-STIR and LGE imaging, and allow direct visualization of nonischemic pattern of distribution. The main reasons can be summarized as follows. Firstly, the CE-CMRA images acquired by FLASH sequence had higher spatial resolution with voxel size decreased by 3-fold than the T2-STIR and LGE techniques. Secondly, compared with two-dimensional techniques (T2-STIR and 2D-LGE), the 3D FLASH pulse sequence could provide thinner sections without interslice gaps that allowed multiplanar reformation in any projection, yielding the special cardiac anatomic overview. Thirdly, a contrast agent Gd-BOPTA, shorten the T1 relaxation rate, have been used to improve SNR and contrast-to-noise ratio (CNR).
Conclusion.
In conclusion, this study demonstrated the feasibility of CE-CMRA for detection of myocardial hyperemia in patients with suspected acute myocarditis. Furthermore, this approach could serve as a helpful supplementary tool to assess coronary artery significant stenosis. The results of the present study suggested that CE-CMRA may potentially improve accuracy of evaluating the original Lake Louise Criteria to identify acute myocarditis in combination with T2-STIR and LGE imaging.Acknowledgements
The authors thank the members of cardiac magnetic resonance team at Fujian Medical University Union Hospital.References
1. Luetkens JA, Doerner J, Thomas DK, Dabir D, Gieseke J, Sprinkart AM, et al. Acute myocarditis: multiparametric cardiac MR imaging. Radiology 2014;273:383–92.
2. Perfetti M, Malatesta G, Alvarez I, et al. A fast and effective method to assess myocardial hyperemia in acute myocarditis by magnetic resonance. Int J Cardiovasc Imaging 2014;30(3):629–637.
3. Yang Q, Li K, Liu X, et al. Contrast-enhanced whole-heart coronary magnetic resonance angiography at 3.0-T. A comparative study with X-ray angiography in a single center. J Am Coll Cardiol 2009;54:69 –76.
Figures
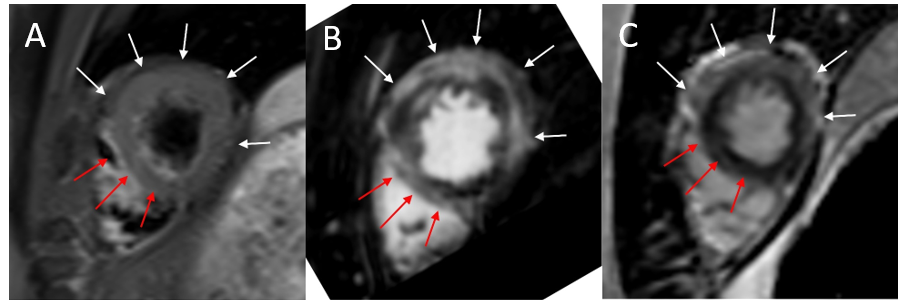
Cardiac MRI in a 24-year-old male patient with acute myocarditis. T2-STIR image in a short-axis view (A) showed a high signal in the septum wall (red arrows), no obvious increased signal in the anterior and lateral wall (white arrows). CE-CMRA reconstructed image in short axis view (B) and LGE image (C) detected remarkable high signal with largely corresponding area (arrows). Sharper delineated lesion border and more clear enhancement area (red arrows) were shown in the CE-CMRA reconstructed images.
T2-STIR image in a 4-chamber (D) showed an increased signal in the anterolateral wall (white arrows) with blur border, while lesion in septum wall (red arrows) was hard to confirm due to the affection by residual blood signal. CE-CMRA reconstructed image in 4-chamber view (E) clearly demonstrated high signal in both septal and anterolateral wall (arrows). LGE in 4-chamber view (F) showed obvious enhancement in the anterolateral wall (white arrows), while not clear in the septum wall (red arrows).
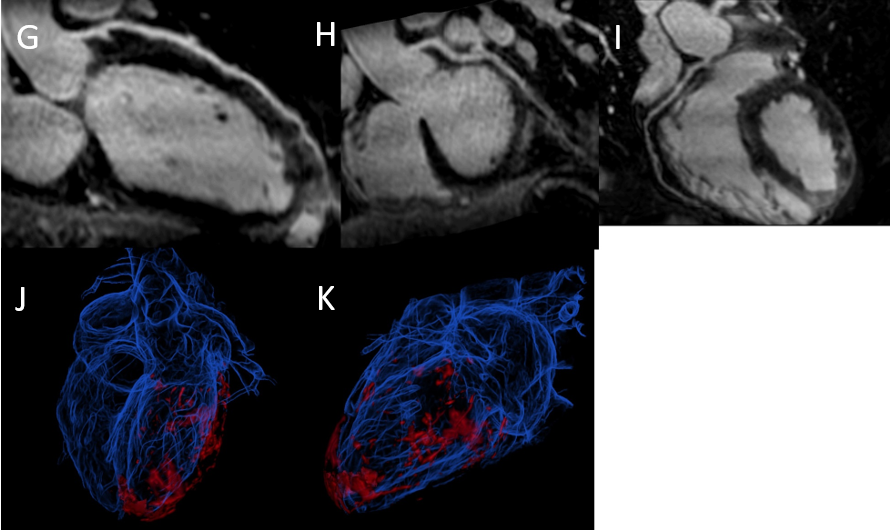
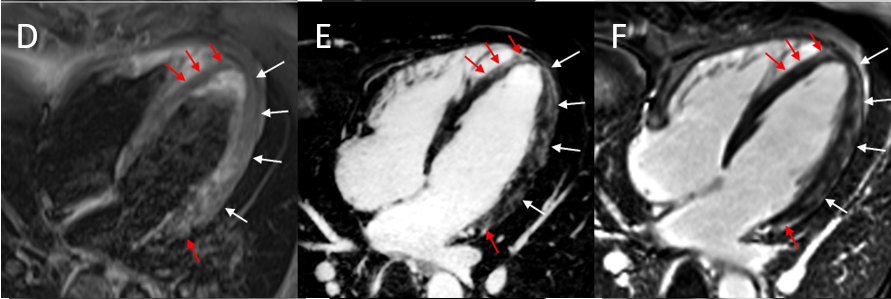
Curved multiplanar reconstruction depicted normal right coronary artery (G), left anterior descending artery (H), left circumflex artery (I).
Volume rendering image (J, K) with different orientation provided an overview of myocardial lesion marked in red.