2893
Non-contrast, high spatial resolution coronary magnetic resonance angiography versus coronary computed tomography angiography1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Department of Radiology, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 3MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
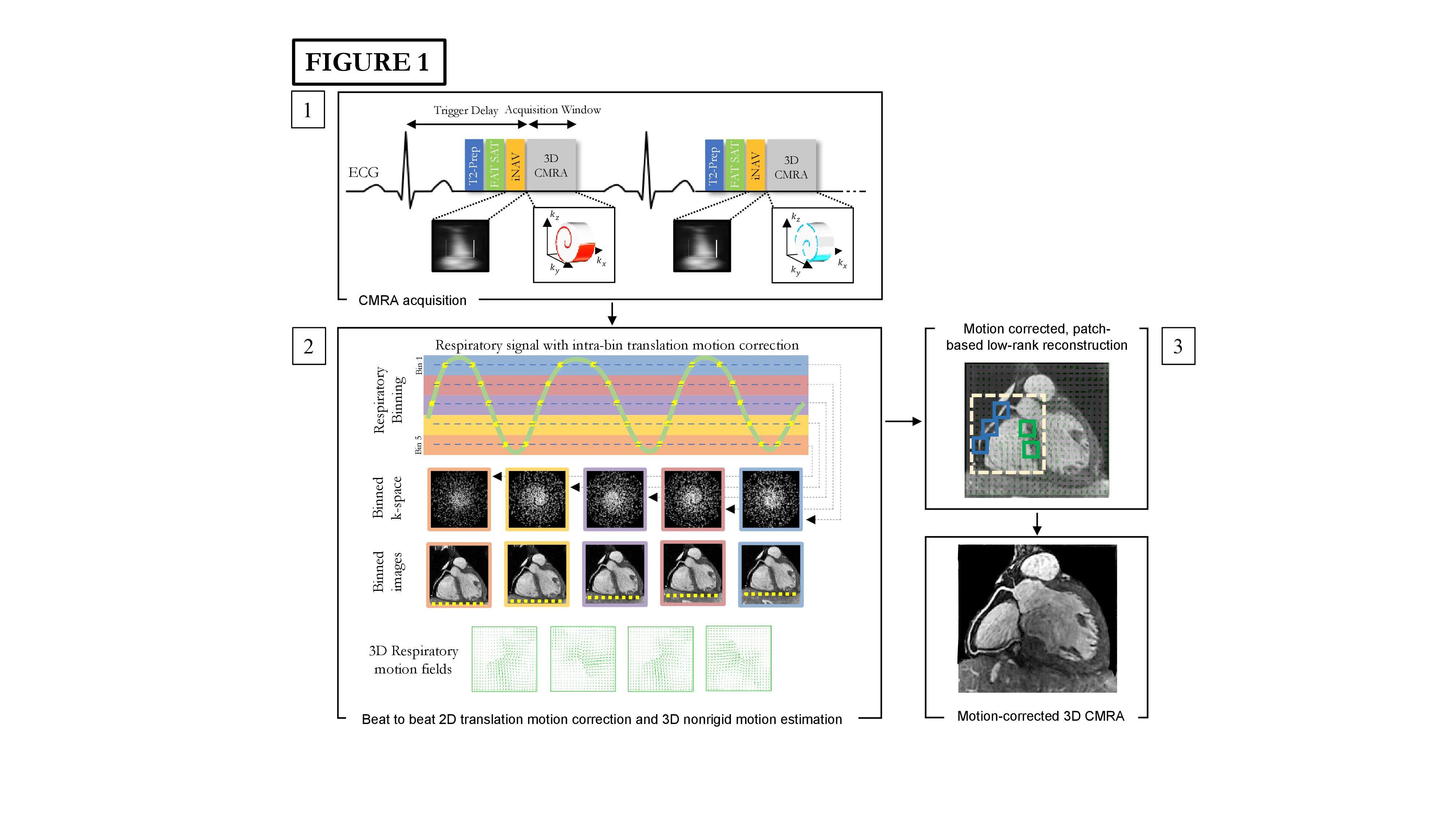
Conventional coronary magnetic resonance angiography (CMRA) is limited by long and unpredictable acquisition-times, low spatial resolution and motion related image quality degradation. To overcome these challenges, we have proposed a highly undersampled acquisition with image-based navigators and non-rigid motion correction to enable high resolution (0.9mm3) CMRA with ≈11min acquisition time. In 30 patients with suspected coronary artery disease (CAD) who also underwent a coronary computed tomography angiography (CCTA), our CMRA framework achieved excellent image quality across all coronary artery segments, with a per patient sensitivity of 100%, specificity of 68% and negative predictive value of 100% for identifying/excluding significant CAD.
Introduction
The widespread clinical application of coronary magnetic resonance angiography (CMRA) for the assessment of coronary artery disease (CAD) remains limited due to low scan efficiency resulting in prolonged and unpredictable acquisition times; low spatial resolution and residual respiratory motion artefacts. To overcome these limitations, we have integrated highly undersampled acquisitions with image-based navigators and non-rigid motion correction to enable high resolution (0.9mm3) free-breathing, contrast-free 3D whole-heart CMRA with 100% respiratory scan efficiency in a clinically feasible and predictable acquisition time (Figure 1) (1). The objective of this study was to evaluate the diagnostic performance of this CMRA framework against the non-invasive anatomical reference standard of coronary computed tomography angiography (CCTA) for excluding significant CAD.Methods
Consecutive patients (n=30) with suspected CAD were recruited from the outpatient CCTA list and all scans were performed using a prototype CMRA sequence on a 1.5T MR scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) within an average of 14 days of the preceding CCTA scan. In the absence of contraindications, each patient was treated with intravenous metoprolol with a maximum dose of 30 mg aiming for a target heart rate (HR) < 65 bpm in order to maximize the diastolic acquisition window, reduce HR variability and cardiac motion artefacts. All patients were also treated with 800 micrograms of sublingual glyceryl trinitrate to promote coronary vasodilation. We compared the diagnostic accuracy of CMRA against CCTA for detecting a ≥50% reduction in luminal diameter. The CMRA scans were analyzed by two independent experts with Society for Cardiovascular Magnetic Resonance (SCMR) and European Association of Cardiovascular Imaging (EACVI) level III accreditation and more than 14 years and 5 years respectively of experience in clinical CMR who were blinded to the CCTA findings.Results
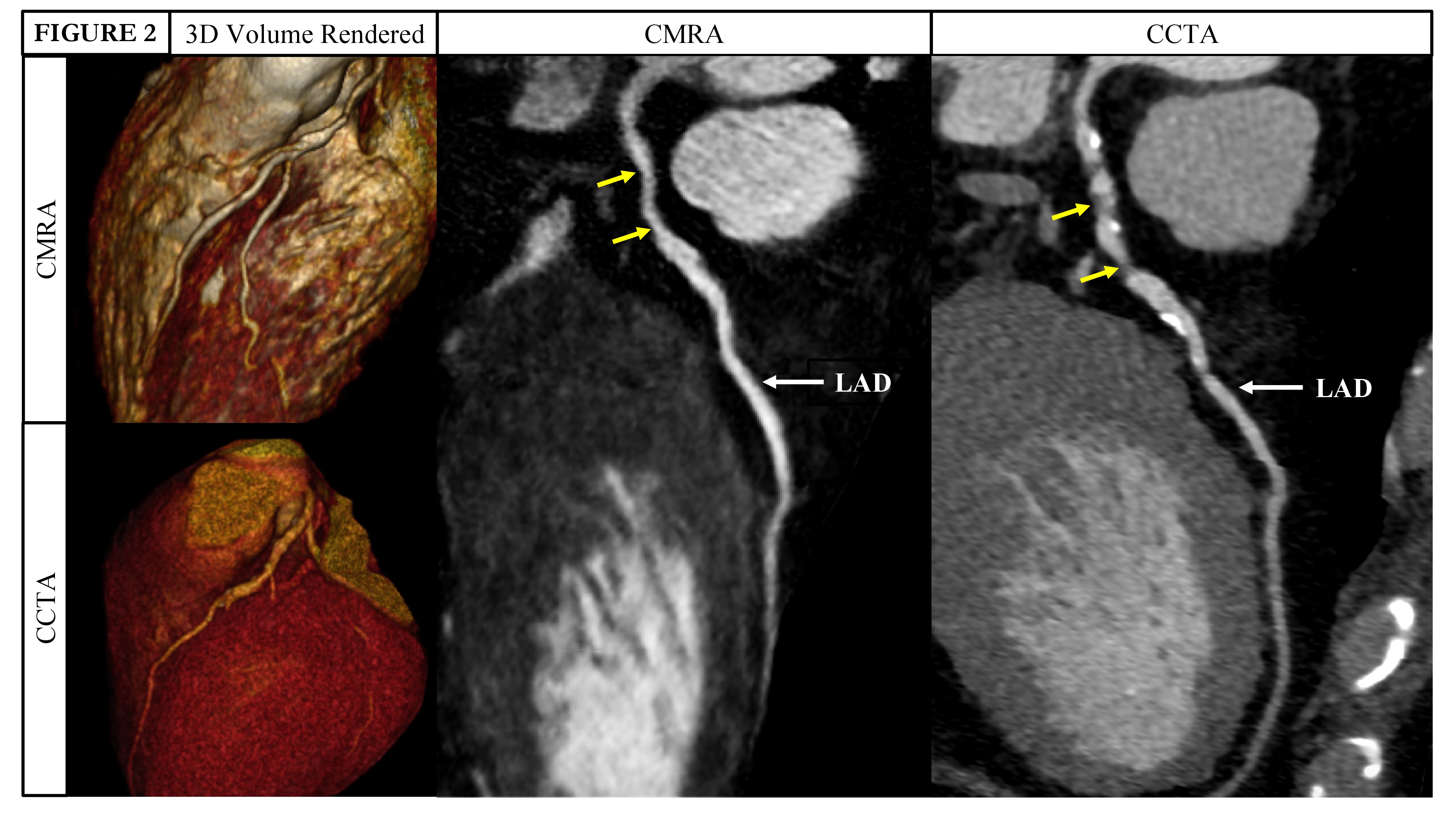
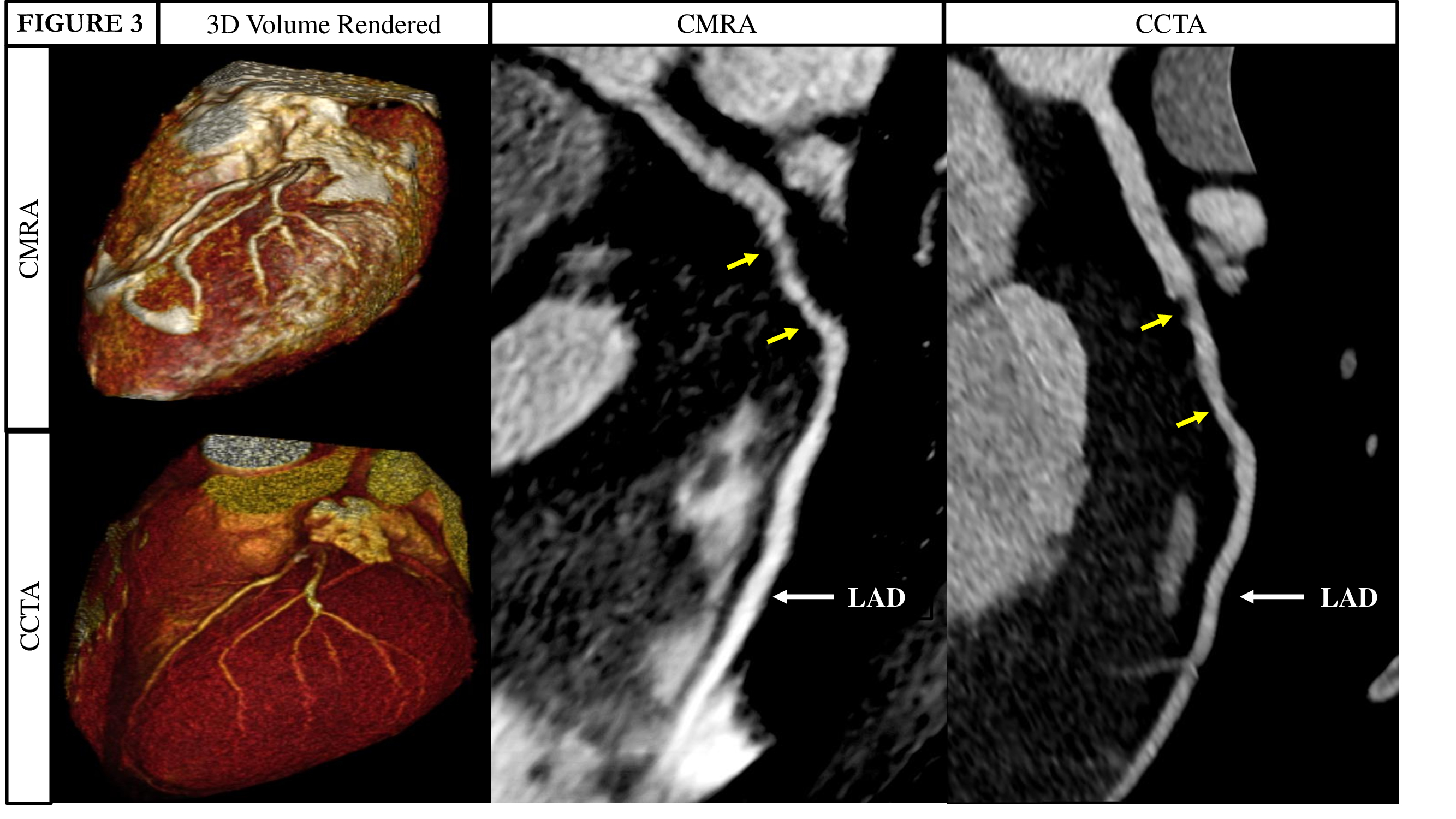
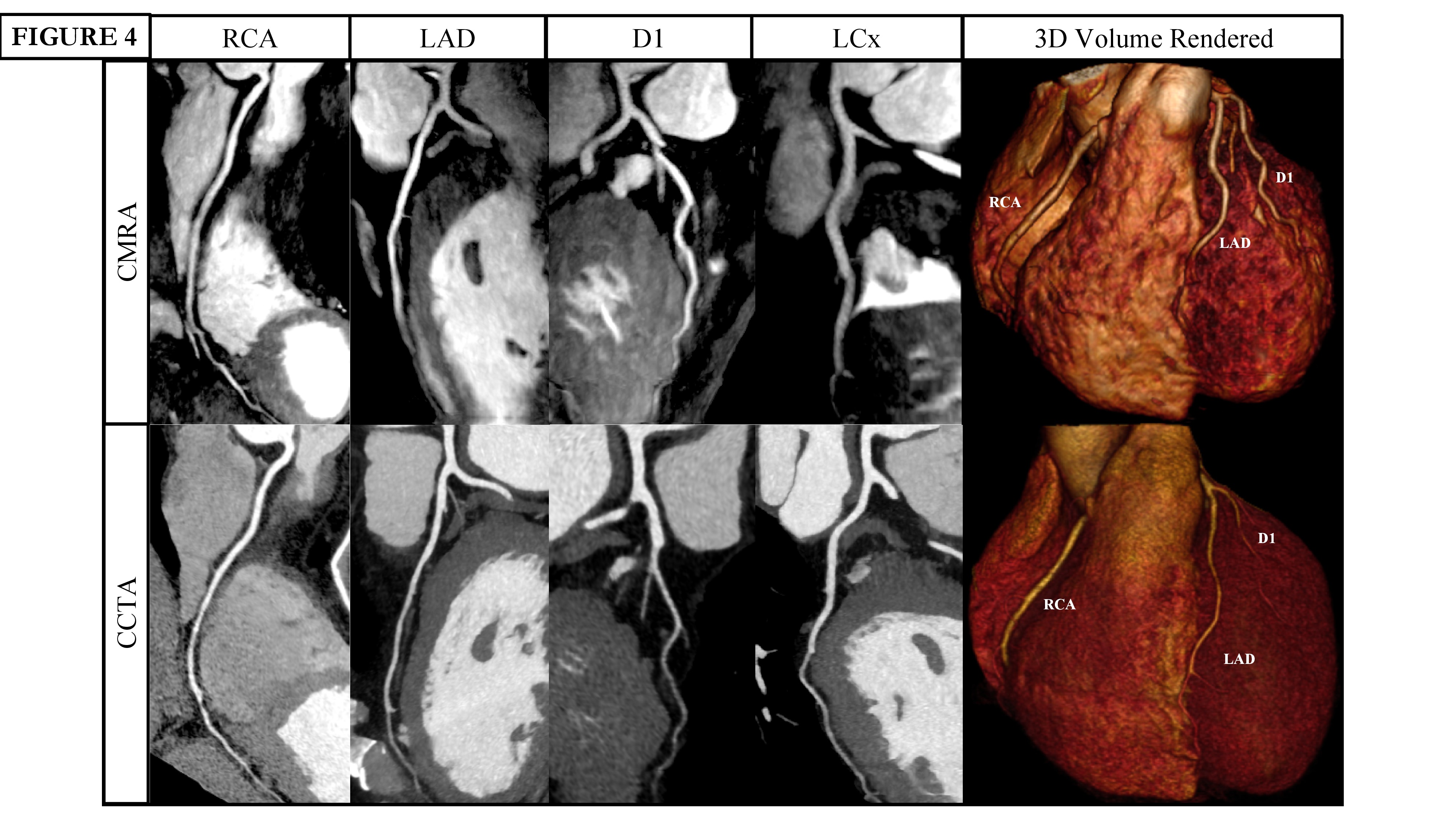
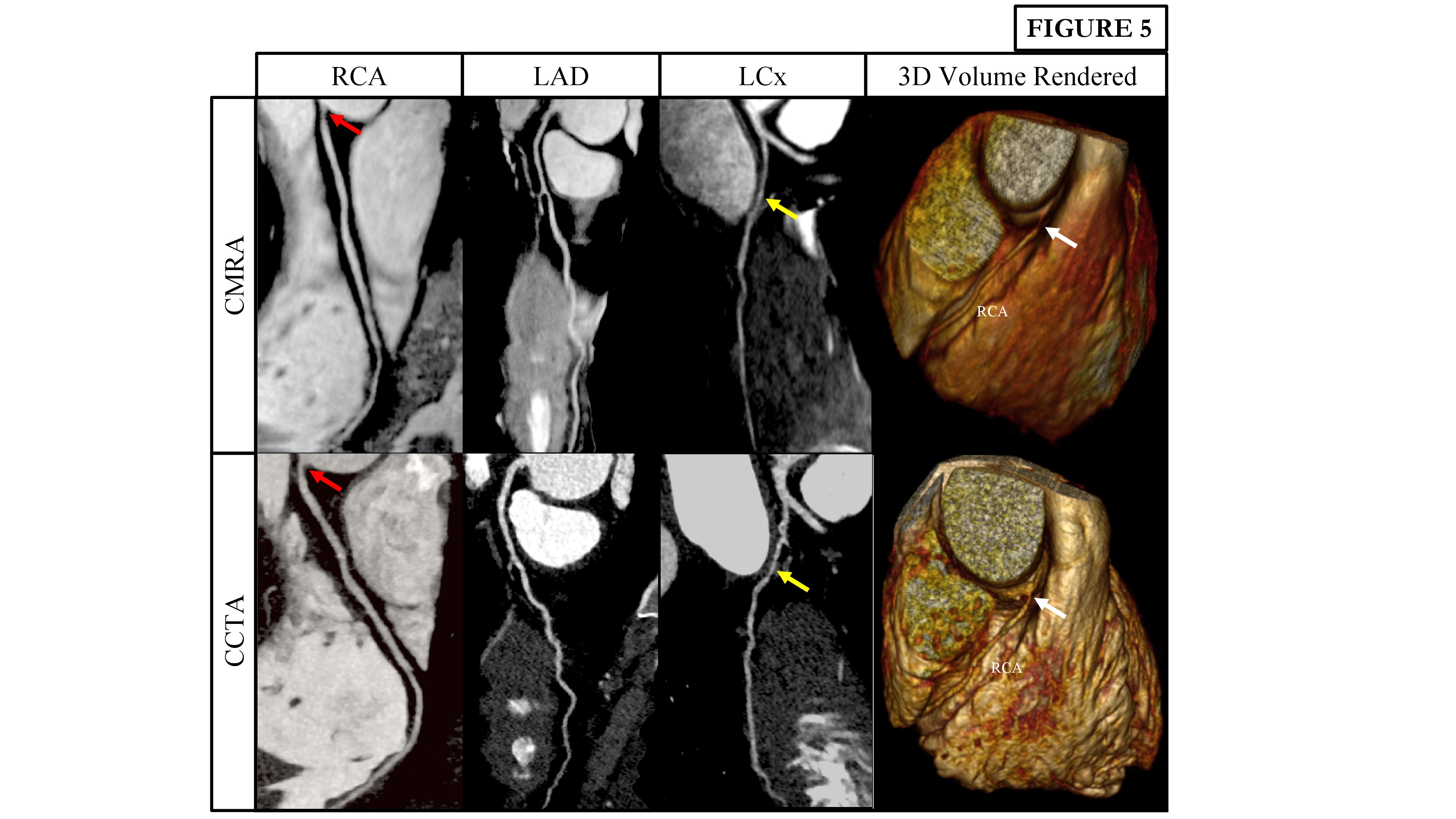
All 30 recruited patients completed their CMRA scan in an average acquisition time of 11.0 ± 1.3 mins. Mean age was 57 ± 9 years, 21/30 (70%) were male and 8/30 (27%) had significant CAD on CCTA. CMRA obtained diagnostic image quality in 96%, 98%, 97% and 91% of all, proximal, middle and distal coronary segments respectively. Furthermore, 100%, 97%, 97% and 90% of left main stem, right coronary artery, left anterior descending and left circumflex artery segments respectively on CMRA were of diagnostic image quality. The sensitivity, specificity, positive predictive value, negative predictive value and diagnostic accuracy were as follows: per patient (100%, 68%, 53%, 100% and 77%), per vessel (82%, 85%, 43%, 97% and 84%) and per segment (81%, 94%, 46%, 99% and 93%) respectively. Representative examples of CMRA and CCTA of two patients with significant CAD are shown in figures 2 to 5.Conclusions
The high diagnostic image quality and diagnostic performance of CMRA compared against CCTA demonstrates the potential of CMRA as a robust and safe non-invasive alternative for excluding significant CAD.Acknowledgements
No acknowledgement found.References
1. Bustin A, Rashid I, Cruz G, et al. 3D whole-heart isotropic sub-millimeter resolution coronary magnetic resonance angiography with non-rigid motion-compensated PROST. J. Cardiovasc. Magn. Reson. 2020;22:https://doi.org/10.1186/s12968-020-00611-5.Figures