2892
High-resolution 3T post-contrast whole-heart coronary MRA with image-based navigation: stenosis identification compared to CTA.1Peking union medical college hospital, Beijing, China, 2School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 4Siemens Healthcare GmbH, Erlangen, Germany, 5Siemens Healthcare Limited, London, United Kingdom
Synopsis
This study sought to evaluate the clinical feasibility, image quality and diagnostic accuracy of a prototype 3T post-contrast high-resolution whole-heart coronary MR angiography (CMRA) sequence with image-navigator (iNAV) based motion correction and 100% respiratory scan efficiency integrated into clinical cardiac MR scan before LGE imaging. The results showed CMRA imaging completed on average in 5.2minutes with promising image quality. CMRA showed good inter-modality agreement compared to computed tomography angiography (CTA) and high negative predictive value (NPV), which allows effective exclusion of coronary artery disease.
Purpose:
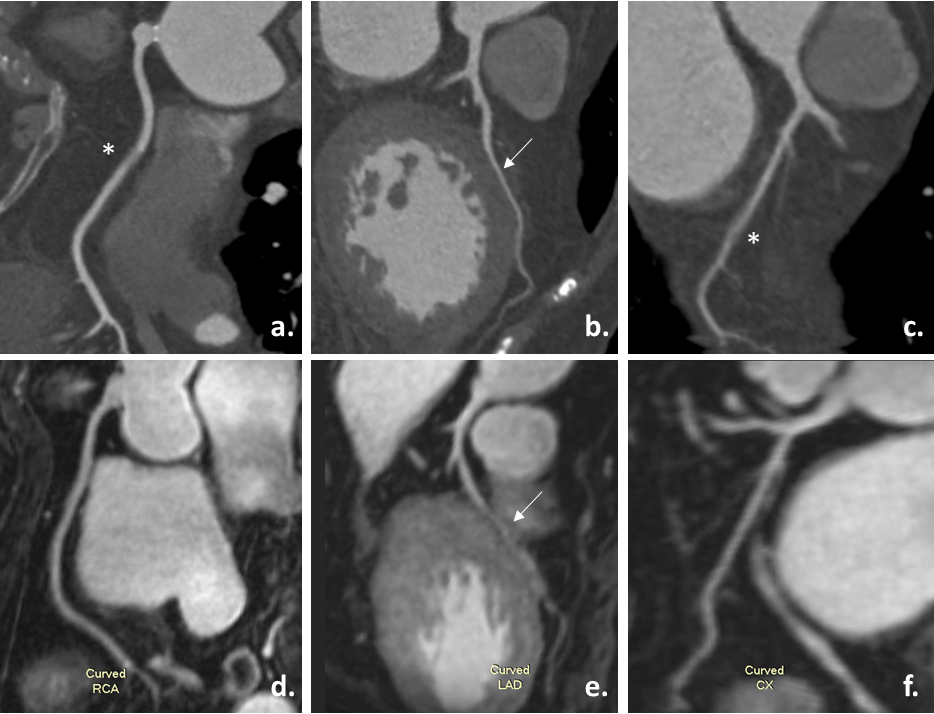
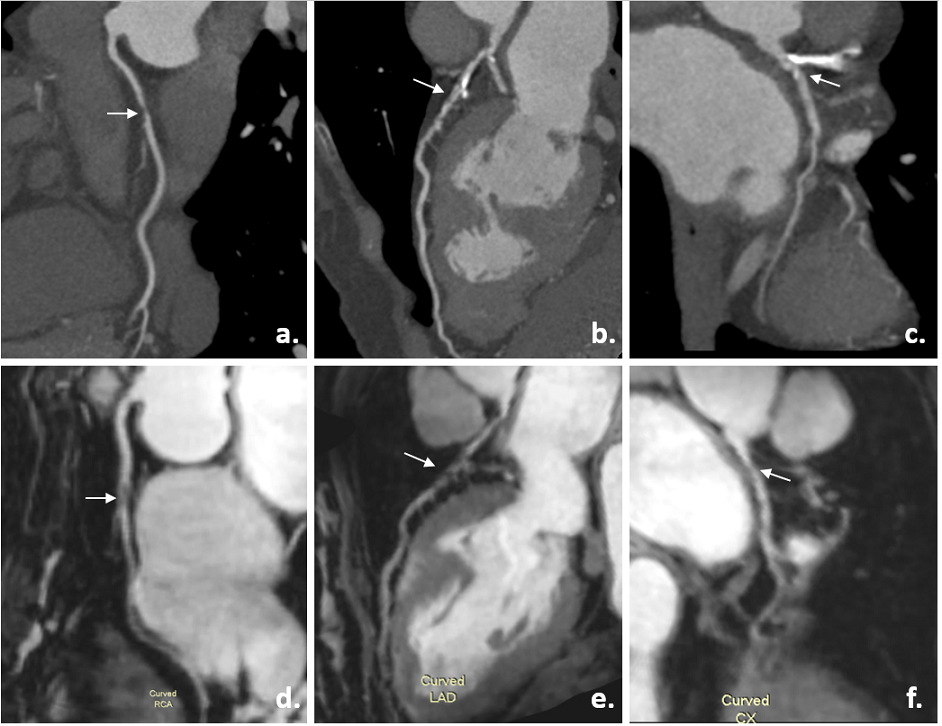
This study sought to evaluate the image quality and diagnostic accuracy of a prototype 3T post-contrast high-resolution whole-heart coronary MR angiography (MRA) sequence with image-based navigation (iNAV) [1], non-rigid motion correction [2] and 100% respiratory scan efficiency integrated into routine cardiac MR (CMR) exam before late gadolinium enhancement (LGE), with coronary CT angiography (CTA) as the reference standard.Methods:
Twenty-three consecutive patients clinically referred to a comprehensive cardiac MR examination were included. All the patients were imaged on a 3T MRI scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) and coronary CTA was performed within 30 days following clinical routine. Free-breathing whole heart coronary MRA was acquired after the injection of contrast agent (gadopentetate dimeglumine, 0.15mmol/kg) using a prototypeT2-prepared FLASH 3D 2-point Dixon sequence with iNAV, non-rigid motion-correction and iterative SENSE reconstruction with variable density spiral like Cartesian acquisition [3-4]. The key imaging parameters were TR/TE = 4.9/1.4 msec, flip angle =15°, bandwidth = 967 Hz/pixel and voxel size = 1.05mm x 1.05 mm x 1.00 mm, Acceleration factor=5.8. Acquisition time was recorded. Subjective image quality of coronary MRA and >50% vessel stenosis were evaluated based on AHA-17 segment model. Image quality was rated on a 4-point scale: 4, excellent (vessel well depicted with sharply defined borders); 3, good (vessel adequately visualized with blurred border); 2, fair (vessel visible but very low confidence in diagnosis with moderately blurred border); 1, poor (vessel barely seen or obscured by artifacts or noise, of non-diagnostic quality). Inter-modality agreement between coronary MRA and CTA was assessed using intraclass correlation coefficient (ICC) with the level of agreement as follows: poor, ICC < 0.20; fair, ICC = 0.21 to 0.40; moderate, ICC =0.41 to 0.60; good, ICC=0.61 to 0.80; and excellent, ICC > 0.80. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of MRA for identifying >50% coronary stenosis were calculated, using coronary CTA as the reference standard.Results:
All 23 patients (11male, 52±17 years) completed coronary MRA in an average time of 5.2±1.4 minutes with no additional delay for routine LGE imaging. A total of 274 coronary segments were visible and graded 4, 3, 2 and 1 in 120 (43.8%), 95 (34.7%), 44 (16.0%) and 15 (5.5%) segments, respectively. Four (17.4%) patients and 7 (10.1%) vessels had >50% stenosis according to CTA. The ICC between MRA and CTA on patient, vessel, and segment-based level is 0.76, 0.79 and 0.63. Using CTA as reference standard, the sensitivity, specificity, PPV and NPV of MRA for the detection of >50% stenosis were 100%, 89.5%, 66.7%, and 100% on per-patient basis and 100%, 90.3%, 53.8%, and 100% on per-vessel basis.Discussion/Conclusion:
Post-contrast whole-heart coronary MRA with iNAV based non-rigid motion compensated reconstruction showed promising image quality and shortened scan time, enabling its integration in a clinical cardiac MR imaging protocol before LGE. For the detection of significant coronary stenosis, MRA showed good inter-modality agreement compared to CTA. Using CTA as reference standard, MRA had high sensitivity and NPV, which allows the effective exclusion of coronary artery disease.Acknowledgements
No acknowledgement found.References
1. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012 Feb;67(2):437-45. 2.
2. Cruz G, Atkinson D, Henningsson M, Botnar RM, Prieto C. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2017 May;77(5):1894-1908. 3.
3. Prieto C, Doneva M, Usman M, Henningsson M, Greil G, Schaeffter T, Botnar RM. Highly efficient respiratory motion compensated free-breathing coronary mra using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015 Mar;41(3):738-46.
4. Bustin A, Rashid I, Cruz G, Hajhosseiny R, Correia T, Neji R, Rajani R, Ismail TF, Botnar RM, Prieto C. 3D whole-heart isotropic sub-millimeter resolution coronary magnetic resonance angiography with non-rigid motion-compensated PROST. J Cardiovasc Magn Reson. 2020 Apr 16;22(1):24.
Figures