2774
Utility of compressed sensing VIBE for hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI: comparison with conventional VIBE
Hirokazu Otsuka1, Yoshihiko Fukukura2, Takashi Iwanaga1, Yuichi Kumagae2, Yasumasa Saigo1, Hiroshi Imai3, and Takashi Yoshiura2
1Kagoshima University Hospital, Kagoshima, Japan, 2Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan, 3Siemens Healthcare K.K., Tokyo, Japan
1Kagoshima University Hospital, Kagoshima, Japan, 2Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan, 3Siemens Healthcare K.K., Tokyo, Japan
Synopsis
This study focused on the feasibility of volumetric-interpolated breath-hold examination (VIBE) using compressed sensing (CS) acceleration (CS-VIBE) for the hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI in comparison with conventional VIBE. Our results showed a significantly higher signal-to-noise ratio and contrast-to-noise ratio (CNR) in CS-VIBE than in conventional VIBE. CS-VIBE showed a significantly higher CNR than conventional VIBE, even when decreasing a slice thickness from 1.5 mm to 1.1 mm of CS-VIBE. These results suggested CS-VIBE could replace conventional VIBE with superior CNR and spatial resolution.
Introduction
Gd-EOB-DTPA-enhanced MRI represents an essential part in the assessment of the identification and characterization of hepatic lesions. The hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI is commonly acquired with a sequence of a single breath-hold of approximately 20 s using fat-suppressed three-dimensional gradient-echo T1-weighted imaging, such as T1-weighted volumetric interpolated breath-hold examination (VIBE) sequence. A prototype of T1-weighted VIBE sequence has been developed, which supports compressed sensing (CS-VIBE). Compressed sensing (CS) enables accelerated MRI acquisition by nonlinear iterative reconstruction of sparsely under-sampled k-space data (1-3), and has shown the ability to significantly reduce scan time or increase spatial resolution with no increase in scan time. However, the feasibility of CS-VIBE sequence for the hepatobiliary phase of Gd-EOB-DTPA enhanced MRI has not been elucidated. Therefore, the purpose of this study was to evaluate the feasibility of CS-VIBE sequence for the hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI in comparison with conventional VIBE sequence.Methods
Our study population consisted of 43 patients (29 men, 14 women; mean age, 66 years; range, 16–88 years) with suspected liver lesions who prospectively underwent Gd-EOB-DTPA-enhanced MRI between June and November 2020. Breath-hold conventional and CS-VIBE were obtained 20 min after Gd-EOB-DTPA administration. Scan parameters of conventional VIBE were as follows: repetition time = 3.1 ms, echo time = 1.3 ms, flip angle = 15o, field of view = 350 × 280 mm, matrix = 320 × 169, slice thickness = 1.5 mm, slice number = 120, acceleration factor of CAIPIRINHA = 4, and acquisition time = 20 s. CS-VIBE was acquired with 2 different slice thicknesses (1.1 mm and 1.5 mm). The other scan parameters of CS-VIBE were kept the same for conventional VIBE, except for the acceleration factor of CS = 12 with 3 dynamic scans (temporal resolution for one phase = 4 s) and acquisition time = 18 s. Signal-to-noise ratio (SNR) of the liver (n=43) and contrast-to-noise ratio (CNR) of the malignant liver tumor (n=31) were calculated using circular or oval regions of interest (ROIs). The SNR and CNR were compared between conventional VIBE and CS-VIBE sequences using the paired t-test.Results
The SNR of the liver parenchyma was significantly higher in CS-VIBE with a slice thickness of 1.5 mm (14.8 ± 5.1) than in conventional VIBE with a slice thickness of 1.5 mm (12.8 ± 3.0) (P < 0.001) (Fig. 1). There was no significant difference in SNR of the liver parenchyma between conventional VIBE with a slice thickness of 1.5 mm (12.8 ± 3.0) and CS-VIBE with a slice thickness of 1.1 mm (13.5 ± 3.5) (P = 0.327). Conventional VIBE with a slice thickness of 1.5 mm (5.9 ± 2.3) showed a significantly lower CNR of the malignant liver tumors than CS-VIBE with a slice thickness of 1.1 mm (6.5 ± 2.6) (P = 0.008) or 1.5 mm (6.9 ± 2.9) (P < 0.001).Discussion
Previous researchers reported that CS achieved substantial scan time reduction while providing similar or superior SNR, CNR, and image quality (4). Compared with conventional VIBE, in our study, CS-VIBE provided superior SNR of the liver parenchyma and CNR of the malignant liver tumor with no increase in scan time on the hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI. Even when decreasing a slice thickness from 1.5 mm to 1.1 mm of CS-VIBE, the CNR of malignant liver tumor was significantly higher at CS-VIBE sequence.Conclusion
CS-VIBE achieved superior SNR and CNR when applied to the hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI, while simultaneously increasing spatial resolution and maintaining a similar scan acquisition time. Thus, CS-VIBE could replace conventional VIBE.Acknowledgements
No acknowledgement found.References
- Hollingsworth KG. Reducing acquisition time in clinical MRI by data undersampling and compressed sensing reconstruction. Phys Med Biol 2015;60:R297-R322.
- Jaspan ON, Fleysher R, Lipton ML. Compressed sensing MRI: a review of the clinical literature. Br J Radiol 2015;88:201504878.
- Lustig M, Donoho D, Pauly JM. Sparse MRI: the application of compressed sensing for rapid MR imaging. Magn Reson Med 2007;58:1182-1195.
- Suh CH, Jung SC, Lee HB, et al. High-resolution magnetic resonance imaging using compressed sensing for intracranial and extracranial arteries: comparison with conventional parallel imaging. Korean J Radiol 2019;20:487-497.
Figures
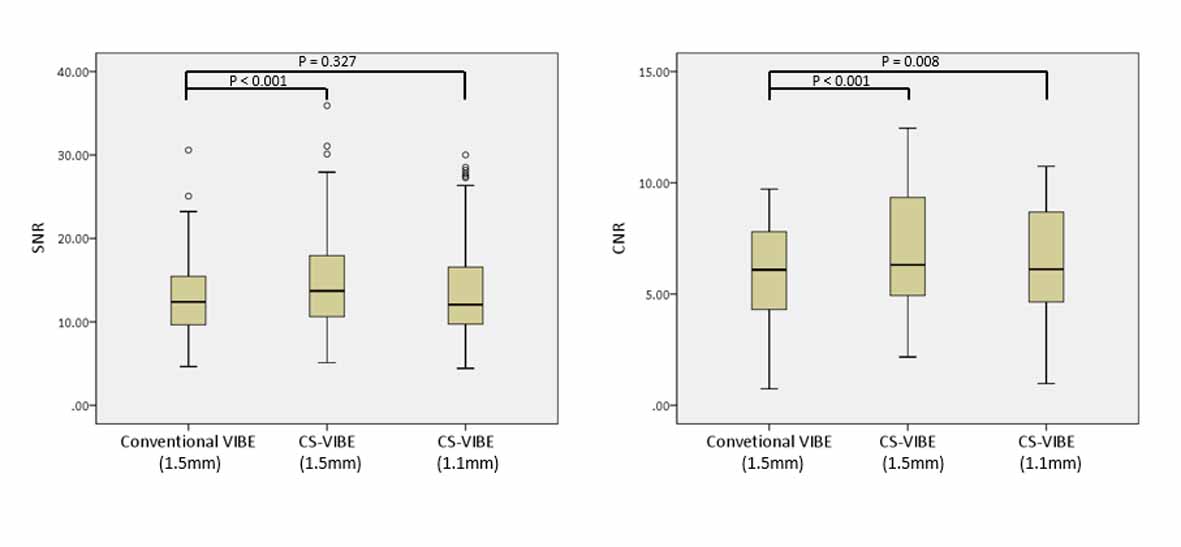
SNR and CNR between conventional VIBE and
CS-VIBE sequences