2771
Effect of Injection Rates in Free-Breathing Gadoxetic Acid-Enhanced MRI with K-Space Weighted Image Contrast Reconstruction.1Center of Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan, 2Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 3MR Clinical Science, Philips Japan, Tokyo, Japan
Synopsis
We prospectively evaluated the effect of injection rates on TIC analysis in free-breathing gadoxetic acid-enhanced MRI using radial sampling with KWIC reconstruction with different injection rate of 1, 2, and 3 mL/s in 48 patients. Time intensity curve analysis was performed and compared among the three injection rate groups. Time to peak in abdominal aorta was significantly shorter with higher injection rates, and the other parameters regarding portal vein, inferior vena cava, and liver parenchyma were not affected by the injection rates. Higher injection rate is recommended for the better discrimination on arterial input data.
Introduction
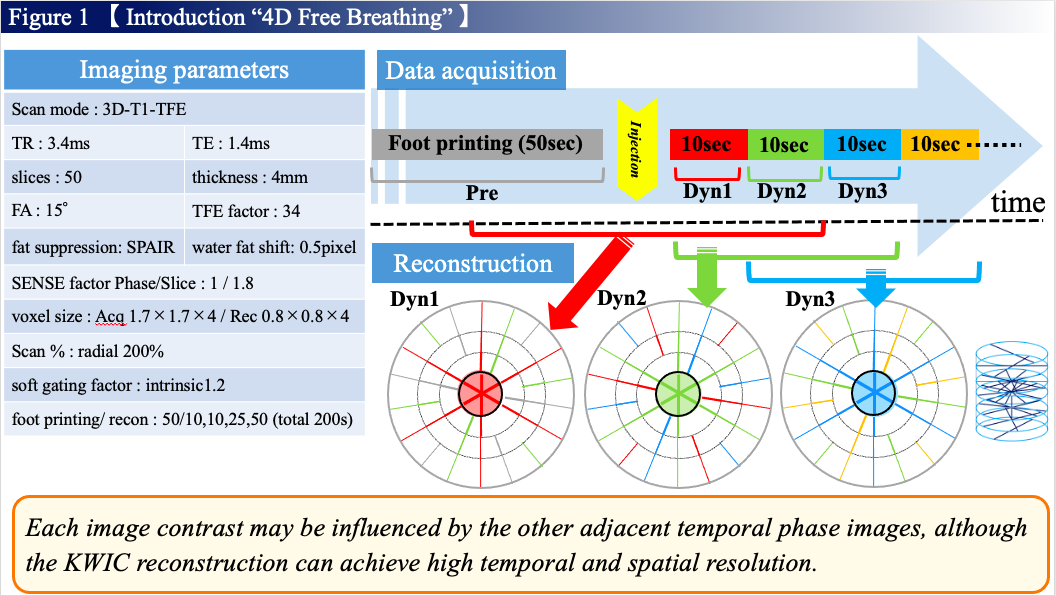
Advent of motion correction sequences using radial sampling, such as stack of stars, has enabled dynamic examination of the upper abdomen even in patients who have difficulty in holding their breath1,2. However, the image quality deteriorates due to undersampling of the number of data acquisitions when acquisition duration is relatively short. The k-space weighted image contrast (KWIC) reconstruction is used to guarantee the number of radial samplings, which improves the signal-to-noise ratio (SNR) by keeping short acquisition duration3. In this technique, the central region of k-space is filled with target phase data, and outside the central region of k-space is continuously filled with other phase data to improve temporal resolution while maintaining the SNR4. Although the KWIC reconstruction can achieve high temporal and spatial resolution, the image contrast may be influenced by the other adjacent temporal phase images. Understanding hemodynamics is essential for the accurate diagnosis and perfusion analysis of the liver. We hypothesized that contamination of the enhancement with contrast agent on the adjacent temporal phase data in KWIC reconstruction may affect time intensity curve (TIC) analysis in hepatic examination. The purpose of this study was to investigate the effect of injection rates on TIC analysis in free-breathing gadoxetic acid-enhanced MRI using radial sampling with KWIC reconstruction.Methods
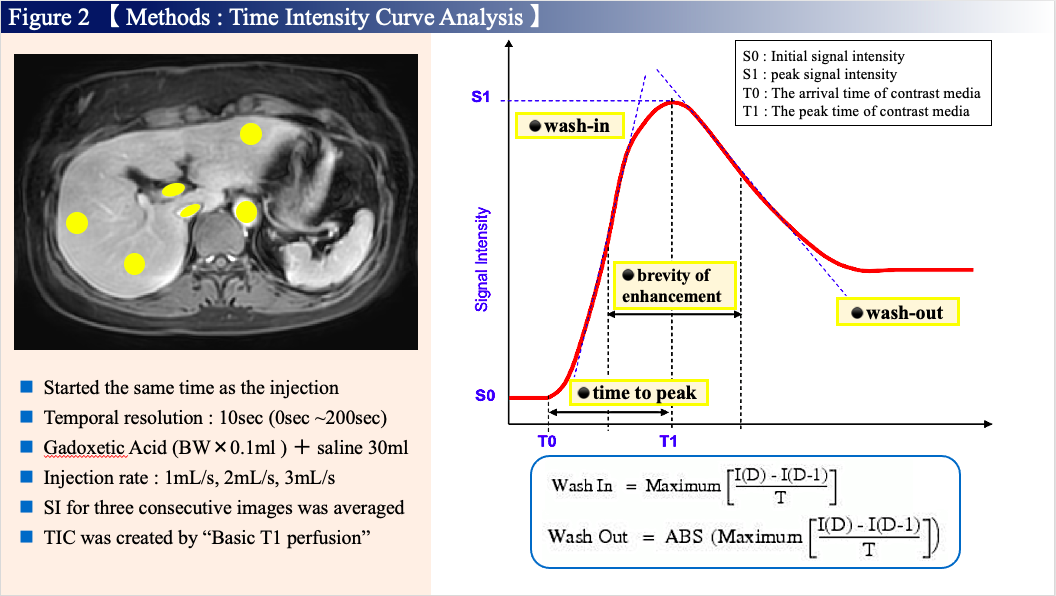
Free-breathing gadoxetic acid-enhanced MRI with variable-density golden angle stack of stars (4D FreeBreathing, Philips Medical Systems; Figure 1) was obtained in patients who were suspected of having liver metastases between January 2020 and November 2020. Forty-eight patients were prospectively divided into three groups according to the injection rate (1 mL/s [n=14], 2 mL/s [n=15], and 3mL/s [n=19]). 4D Free Breathing sequence was continuously scanned during 200 seconds after the initiation of gadoxetic acid injection at a 3T MR scanner (Ingenia 3.0, Philips Medical Systems). Foot printing was conducted in 50 seconds, temporal resolution after injection of gadoxetic acid was conducted in 10 seconds, and 14 phase images were consequently acquired in each patient. From the obtained images, the region of interests was placed to measure signal intensities on abdominal aorta, portal vein, inferior vena cava, and liver parenchyma in each phase. The signal intensities were measured for three consecutive level images and averaged for the following analyses.Time intensity curve (TIC) was created by relative enhancement between precontrast and postcontrast images using the commercial software (Basic T1 Perfusion, Philips Medical Systems). Time to peak (TTP), brevity of enhancement (BE), wash-in, and wash-out were calculated from the TIC analyses (Figure 2). The TTP differences between abdominal aorta and portal vein, and between portal vein and liver parenchyma was also calculated to compare the time-phase discrimination. The calculated parameters obtained from the TIC analyses were compared among the three injection rate groups using the Kruskal-Wallis H-test, and post-hoc pairwise comparison was performed using the Steel-Dwass test for statistically significant parameters. Spearman correlation coefficients were determined between the calculated parameters and the injection rates. For all statistical analyses, P values less than 0.05 were considered as statistically significant.Results
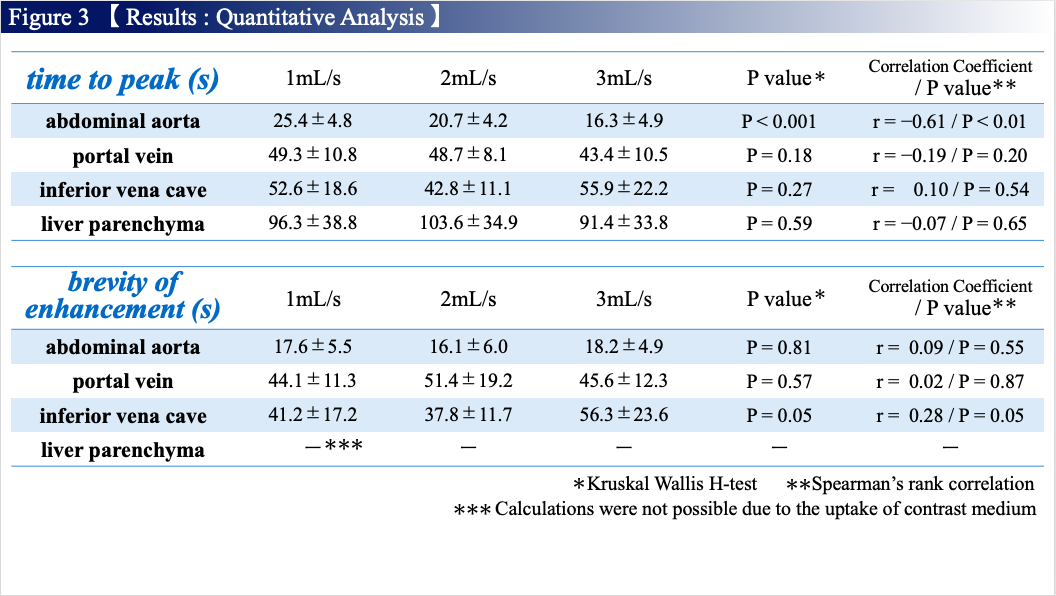
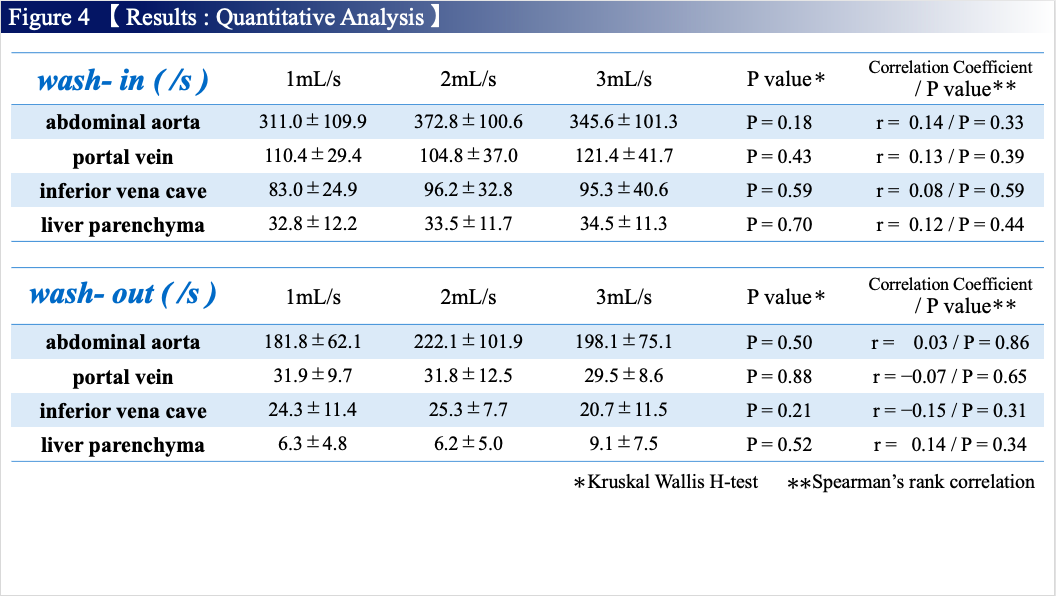
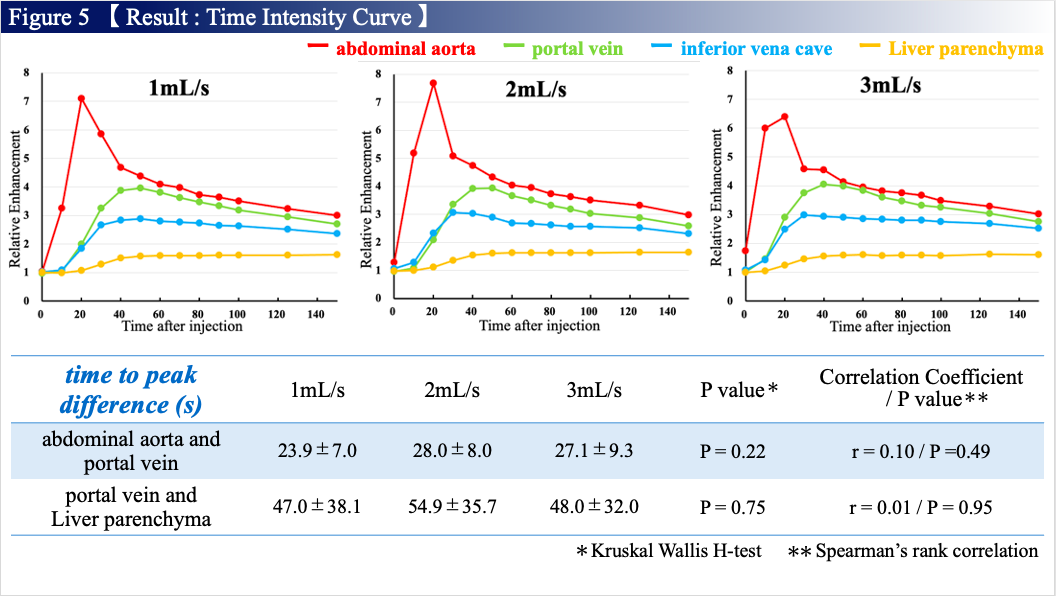
There were no significant differences among the three groups regarding age, sex, weight, and BMI (P=0.92, 0.36, 0.97, and 0.62, respectively). The TTP on abdominal aorta was significantly shorter with higher injection rates (P< 0.001) with strong correlation (r= -0.61, P< 0.001): the TTP in the 3 mL/s group was significantly shorter compared with those in the 2 mL/s group (P= 0.01) and 1 mL/s group (P< 0.01), whereas no significant difference was observed between the 1 mL/s and 2 mL/s groups (P= 0.43). The other parameters including the TTP except for abdominal aorta, BE, wash-in, and wash-out showed no significant differences and correlations among the three groups (Figure 3 and 4). In the time-phase discrimination, no significant differences were also observed regarding the time to peak differences between abdominal aorta and portal vein, and between portal vein and liver parenchyma among the three groups (Figure 5).Discussion
The TIC analyses in the present study demonstrated that the injection rate influenced the arterial input data in free-breathing gadoxetic acid-enhanced MRI using radial sampling with KWIC reconstruction, although the other parameters related to the portal vein, inferior vena cava, and liver parenchyma were not affected. These results indicate that contamination of the enhancement with contrast agent on the adjacent temporal phase data may affect arterial input data alone in radial samplingwith KWIC reconstruction. Higher injection rate may lead to accurate diagnosis of hypervascular liver lesions and perfusion analysis in 4D Free Breathing sequence.Conclusion
Higher injection rate achieved shorter time to peak on abdominal aorta with stable values for the other parameters regarding portal vein, inferior vena cava, and liver parenchyma in free-breathing gadoxetic acid-enhanced MRI usingradial sampling with KWIC reconstruction.Acknowledgements
I would like to thank MRI staffs in Center of Radiology and Radiation Oncology for help with data collection and useful discussions.References
1. Kim KW, Lee JM, Jeon YS, et al. Free-breathing dynamic contrast-enhanced MRI of the abdomen and chest using a radial gradient echo sequence with K-space weighted image contrast (KWIC). Eur Radiol 2013 May;23(5):1352-60.
2. Fujinaga Y, Ohya A, Tokoro H, et al. Radial volumetric imaging breath-hold examination (VIBE) with k-space weighted image contrast (KWIC) for dynamic gadoxetic acid (Gd-EOB-DTPA)-enhanced MRI of the liver: advantages over Cartesian VIBE in the arterial phase. Eur Radiol 2014 Jun;24(6):1290-9.
3. Song HK, Dougherty L. Dynamic MRI With Projection Reconstruction and KWIC Processing for Simultaneous High Spatial and Temporal Resolution. Magn Reson Med 2004 Oct;52(4):815-24.
4. Lin W, Guo J, Rosen MA, et al. Respiratory Motion-Compensated Radial Dynamic Contrast- Enhanced (DCE)-MRI of Chest and Abdominal Lesions. Magn Reson Med 2008 Nov;60(5):1135-46.
Figures