2766
ROI-based intravoxel incoherent motion (IVIM) shows good diagnostic performance on fibrosis severity of patients with chronic hepatitis B
Jiang jinghua1, Weiyin Vivian LIu2, Huang Lesheng1, Liu Tianzhu1, Li Hongyi 1, Chen Jun 1, Zhang Wanchun 1, He Tao 1, and Tang Jiahui 1
1Department of Radiology, Guangdong Hospital of Traditional Chinese Medicine, Zhuhai,519000, China, zhuhai, China, 2MR Reaearch,GE healthcare, Beijing,China, China
1Department of Radiology, Guangdong Hospital of Traditional Chinese Medicine, Zhuhai,519000, China, zhuhai, China, 2MR Reaearch,GE healthcare, Beijing,China, China
Synopsis
IVIM, as a noninvasive tool, has good diagnostic performance in the detection and staging grading of liver fibrosis
Introduction
Liver fibrosis is characterized by excessive accumulation of extracellular matrix (mainly type I collagen). It is a common pathological feature of chronic liver diseases caused by various etiologies, and can develop into liver dysfunction, portal hypertension, and even hepatocellular carcinoma, thus increasing incidence rate and mortality. Early or mid-term liver fibrosis is considered reversible, as long as timely drug intervention and anti-fibrosis treatment. Therefore, early detection and accurate staging of liver fibrosis is of great clinical significance for making correct treatment decisions and evaluating the prognosis of patients. Liver biopsy is the standard reference index for the diagnosis and staging of liver fibrosis; however, it is an invasive examination, and the risk and complications cannot be ignored. Some studies have shown that IVIM, as a noninvasive examination tool, has good diagnostic performance for the detection and staging of liver fibrosis [1].Materials and methods
This study was approved by the Institutional Review Board of our hospital. Six CHB patients with liver biopsy fibrosis S1(fibrosis stage) and G2 (inflammation grade) results confirmed by liver biopsy were recruited. Three ROIs (regionsarea of interest) range from 80 to 100 mm2 were placed on S6 and S7 of right liver while avoiding obvious vessels. The data of ROI 1, ROI 2, ROI 3 and ROI-AVE were analyzed to study whether there was correlation between them. Apparent diffusion coefficient (ADC) of single b value 800 s/mm2, ADC of single index standard , perfusion fraction (f), pseudo-diffusion coefficient (Dfast), diffusion coefficient (Dslow) of IVIM diffusion imaging with 12 b values (0, 25, 50, 75, 100, 150, 200, 300, 400, 500, 600 and 800 s/mm2) were measured for three ROIs and averaged as ROI-AVE using based on both dobble order single and two-segment bi-exponential models and ADC for patients . There were calculated by SPSS21.0 with correlation (Partial correlation) were analyzed using SPSS21.0 with by after controlling patients’ sexgender and age. The potential correlation between singal 800s/mm2DWI-based ADC and IVIM parameters (ADC, Standand Dslow, Dfast, f using single and bi-exponential model) and liver function lab indexes (GGT, AlT, AST, AST/ALT, AFU) [MOU1] were assessed for the CHB patients.Result
ROI1/ ROI2,ROI1/ ROI3,ROI2/ ROI3,>0.05,There was no correlation between ROI1, ROI2 and ROI3.ROI1/ ROIAVG ROI2/ ROIAVG ROI3/ ROIAVG>0.05,There was no correlation between them.So ROI1, ROI2, ROI3 and ROIAVG had no effect on IVIM and ADC.The correlations between the standard ADC in S6 (ROI1, ROI2, ROI3 and ROIAVE) of right liver with AFU (P =0.012), Dslow with AST(P =0.015) and AFU(P =0.007), Dfast with AST(P =0.044). No significant correlation was found between the remaining IVIM parameters and laboratory indexes.Discussion:
This study was aimed to investigate showed the correlation between IVIM model parameters and common laboratory indicators of CHB in patients with inflammation grade 2 and fibrosis stage 1. The collected data showed that there was no correlation between ROI1, ROI2, ROI3 , ROIAVG and IVIM . In this our study, the correlation between ROI-AVE and AFU of Dslow (dobble order bi-exponential model) is more obvious than the single b-value ADC.This correlation between IVIM-based parameters and common laboratory indicators of CHB in patients with inflammation grade 2 and fibrosis stage 1 that average ROI-based measurements is a more reliable discrimination ability of CHB diagnosis. AFU has a diagnostic value in patients with liver cirrhosis and acute hepatitis, especially severe hepatitis. Serum AFU mainly existed in liver tissue., and Serum AFU its level would increase when hepatocytes was damaged. The single b-value ADC measurement can be used to detect liver fibrosis, but can not be used to reliably distinguish the intermediate stages of fibrosis [2]. In addition, In this study, the correlation between ROI-AVE-based and AST of Dslow and AST is also higher (dobble order single exponential model) than that of Dfast(dobble order bi-exponential model).[MOU4] The increase of AST reflects the damage of liver tissue, which AST is an important indicator of hepatitis progression and increases in reflection of .the damage of liver tissue. In this study, the correlation between ROI-AVE and AST of Dslow(dobble order single exponential model) than that of Dfast(dobble order bi-exponential model). The data sample size of this study should be expanded to is small, it is difficult to exclude the contingency, which is not enough to prove, but and to confirm the current observation can not consider thatof there is correlation between IVIM model parameters and common laboratory indicators of CHB in patients with inflammation grade 2 and fibrosis stage 1.Conclusion
IVIM, as a noninvasive tool, has good diagnostic performance in the detection and staging grading of liver fibrosis. However, the biochemical test is a more common diagnostic method in clinical detection of liver fibrosisdiagnosis and, the correlation between the twoboth approaches still needs to expand be examined the relevant sample size, improve and practice standardized IVIM scheme.Acknowledgements
No acknowledgement found.References
liver.pdf>. 2. Sandrasegaran, K., et al., Value of diffusion-weighted MRI for assessing liver fibrosis and cirrhosis. AJR Am J Roentgenol, 2009. 193(6): p. 1556-60.Figures
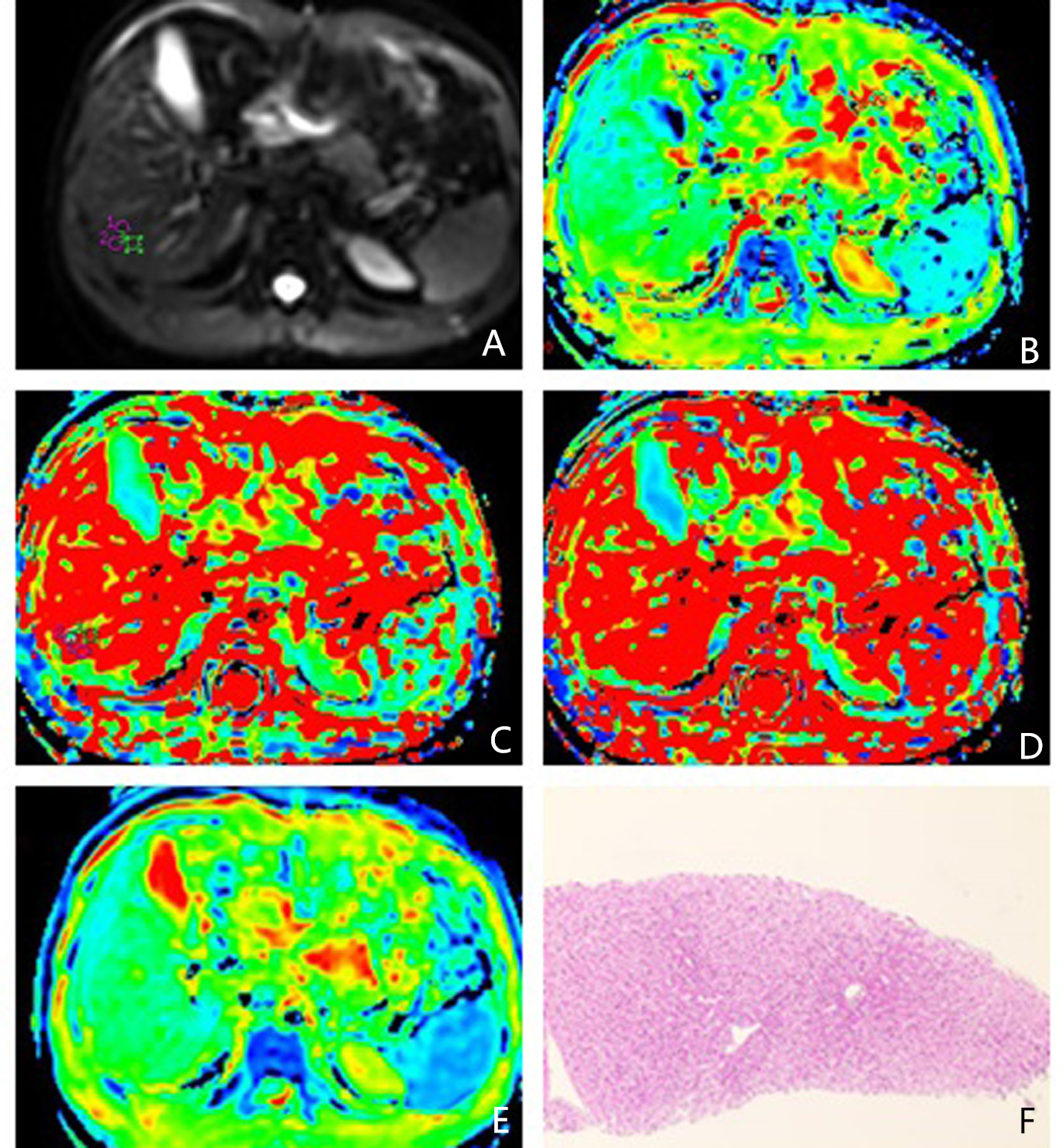
Table 2 Figure 1 Representative images of one case. (A) DWI; (B) Slow ADCBi; (C) Fast ADCMono;(D)Fast ADCBi; (E)Slow ADCMono ;(F)Pathological specimens of patients with S1 and G2
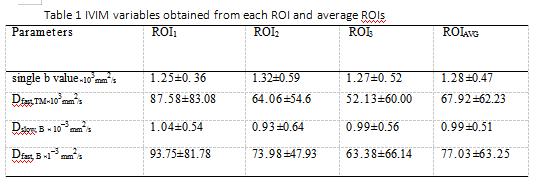
Table 1 IVIM variables obtained from each ROI and average ROIs