2765
Distinction of early fibrosis stages in patients with chronic hepatitis B using intra voxel incoherent motion MR imaging1Guangdong Hospital of Traditional Chinese Medicine, Zhuhai, China, 2MR Research, GE Healthcare, Beijing, China, Beijing, China
Synopsis
The purpose was to evaluate the feasibility of IVIM variables in distinction of patients with early liver fibrosis stages(F1-2). Eight volunteers and 21 patients suspected chronic hepatitis B with fibrosis stage F1 or F2 were recruited. Correlations between all IVIM and DWI variables and ALT, AST, GGT values were analyzed. Two-segment mono-exponential model derived Dslow,TM was statistically different between volunteers and F1 patients(p< 0.05) with AUC of 0.740. The correlation between bi-exponential model derived Dslow,B and GGT was fair(r =0.513, p < 0.05).
Introduction
Early detection and hepatic fibrosis staging is important for determination on treatments such as antifibrotic therapy or invasive surgery by the removal offending lesions. Moreover, the progression of early fibrosis is potentially reversible[1]. Although liver biopsy is still regarded as the gold standard for the evaluation of liver fibrosis, invasiveness and complications such as hemorrhage and infection are major issues. It is necessary to discover noninvasive methods for diagnosis and staging early liver fibrosis status. IVIM parameters of Dfast,B, Dslow,B and f computed based on the bi-exponential model have been proved to be correlated with liver fibrosis stages[2-4]. Our objective was to evaluate IVIM parameters for the distinction of early fibrosis stages(F1-2) and to examine the potential correlation between IVIM and liver function.Methods
This prospective study was approved by the institutional ethical committee. 21 suspected CHB patients with liver fibrosis stage(F1 or F2) confirmed by liver biopsy and 8 healthy controls were recruited. Three ROIs of 80-100mm2 were placed on S6 of right liver while avoiding large vessels. Conventional apparent diffusion coefficient (ADC) and perfusion fraction(f), pseudo diffusion coefficient(Dfast), diffusion coefficient (Dslow) using two-segment mono-exponential and bi-exponential models to analyze IVIM diffusion images with 12 b values(0, 25, 50, 75, 100, 150, 200, 300, 400, 500, 600 and 800s/mm2) were calculated and compared using independent t test when data were in the normal distribution. Partial correlation of measurements and ALT, AST, GGT were analyzed after controlling gender and age.Results
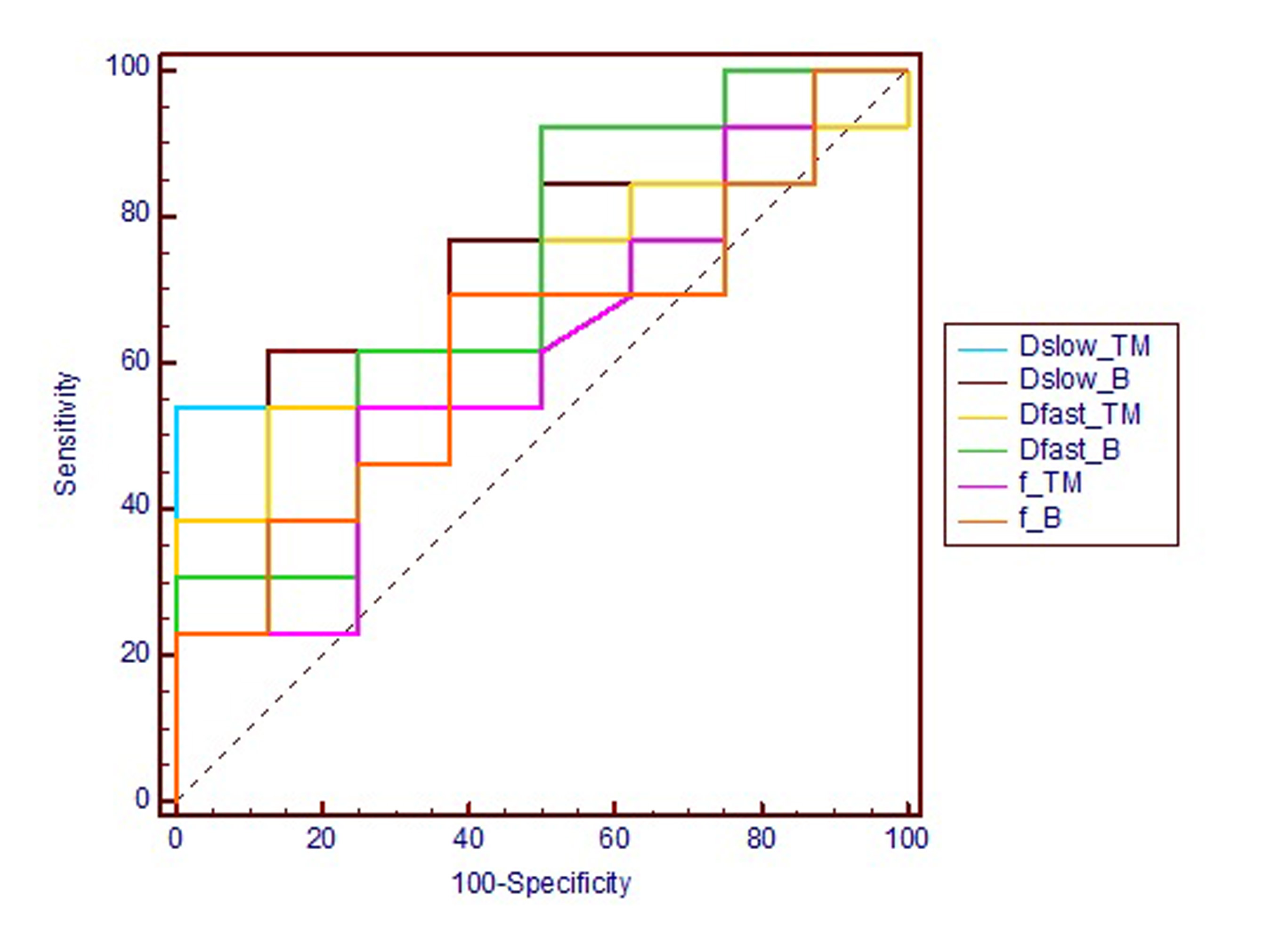
Dslow,TM(two-segment mono-exponential model) was statistically different between volunteers and F1 patients(Fig.1, 0.0113 vs 0.00885, p< 0.05). ROC curves of IVIM parameters were shown in Fig.2 and the AUC of Dslow,TM,Dslow,B,Dfast,TM,Dfast,B and f,TM,f,B were 0.740, 0.712, 0.683, 0.712 and 0.611, 0.625, respectively. No differences were found between F1 and F2 patients with any IVIM parameters and ADC. In control group, a fair correlation was found between Dslow,B(bi-exponential model) with GGT (r =0.513, p < 0.05).Discussion
Our study showed Dslow has good performance of distinguishing patients with early fibrosis stages from healthy controls, which was consistent with previous study[2]. Different IVIM parameters such as Dfast[5, 6], Dslow[2] and f[7] associated hepatic fibrosis stages were found. The meta-analysis study of Bin Song et al. showed that IVIM is a good diagnostic tool in detecting and staging although the parameter differs[4]. Dslow,B was correlated with GGT in patients. Measurements of circulating GGT activity is widely used for the diagnosis of liver and obstructive biliary diseases. Thus, Dslow,B, one of IVIM parameters was an alternative method to reflect liver function.Conclusion
IVIM has potential to detect early fibrosis stages(F1-2) as a noninvasive tool. Although IVIM Dslow was correlated with GGT in patients, the level of liver function could not be determined directly and it is necessary to further explore the combination of various images in assessment of liver function.Acknowledgements
No acknowledgement found.References
1. Marcellin, P., et al., Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. The Lancet, 2013. 381(9865): p. 468-475. 2. Fu, F., et al., Non-invasive assessment of hepatic fibrosis: comparison of MR elastography to transient elastography and intravoxel incoherent motion diffusion-weighted MRI. Abdom Radiol (NY), 2020. 45(1): p. 73-82.
3. Franca, M., et al., Evaluation of fibrosis and inflammation in diffuse liver diseases using intravoxel incoherent motion diffusion-weighted MR imaging. Abdom Radiol (NY), 2017. 42(2): p. 468-477.
4. Zheng Ye, Bin Song, et al. Value of intravoxel incoherent motion in detecting and staging liver fibrosis: A meta-analysis. World J Gastroenterol. 2020 June 21; 26(23): 3304-3317.
5. Ichikawa, S., et al., MRI-based staging of hepatic fibrosis: Comparison of intravoxel incoherent motion diffusion-weighted imaging with magnetic resonance elastography. J Magn Reson Imaging, 2015. 42(1): p. 204-10.
6. Wu, C.H., et al., Assessing hepatic fibrosis: comparing the intravoxel incoherent motion in MRI with acoustic radiation force impulse imaging in US. Eur Radiol, 2015. 25(12): p. 3552-9. 7. Chung, S.R., et al., Intravoxel incoherent motion MRI for liver fibrosis assessment: a pilot study. Acta Radiol, 2015. 56(12): p. 1428-36.
Figures
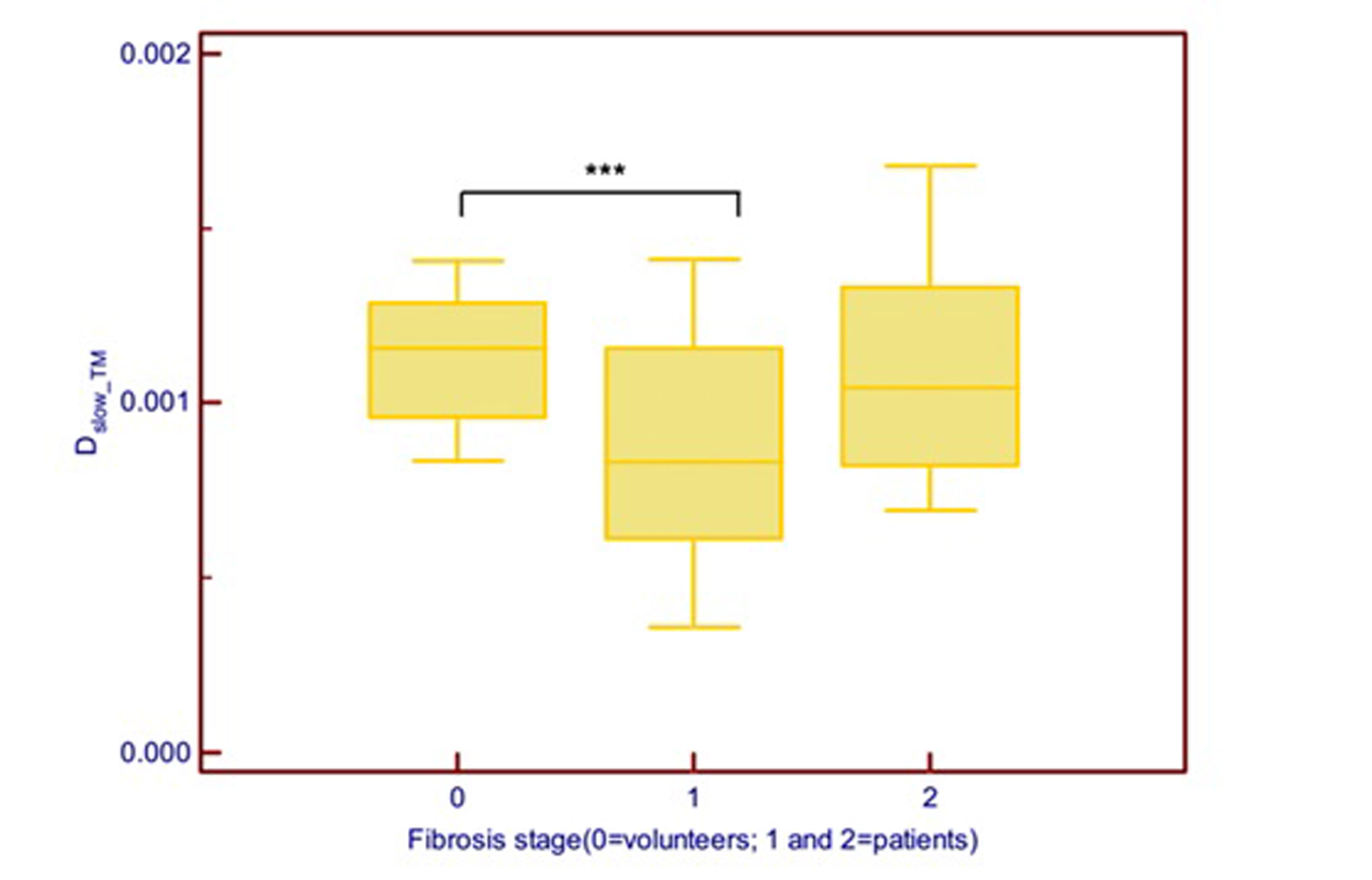
Figure 1. Box and whisker plots of IVIM parameter Dslow-TM.***There was significant difference between volunteers(stage 0) and F1 patients(0.00113 vs 0.000885, p<0.05). No difference was found between F1 and F2 patients.