2755
Portal Venous Hemodynamics with an abdominal 4D-flow MR imaging in patients with and without chronic liver disease1Radiology, Kawasaki Medical School, Okayama, Japan, 2Phillips Japan, Tokyo, Japan, 3Kawasaki Medical School, Okayama, Japan
Synopsis
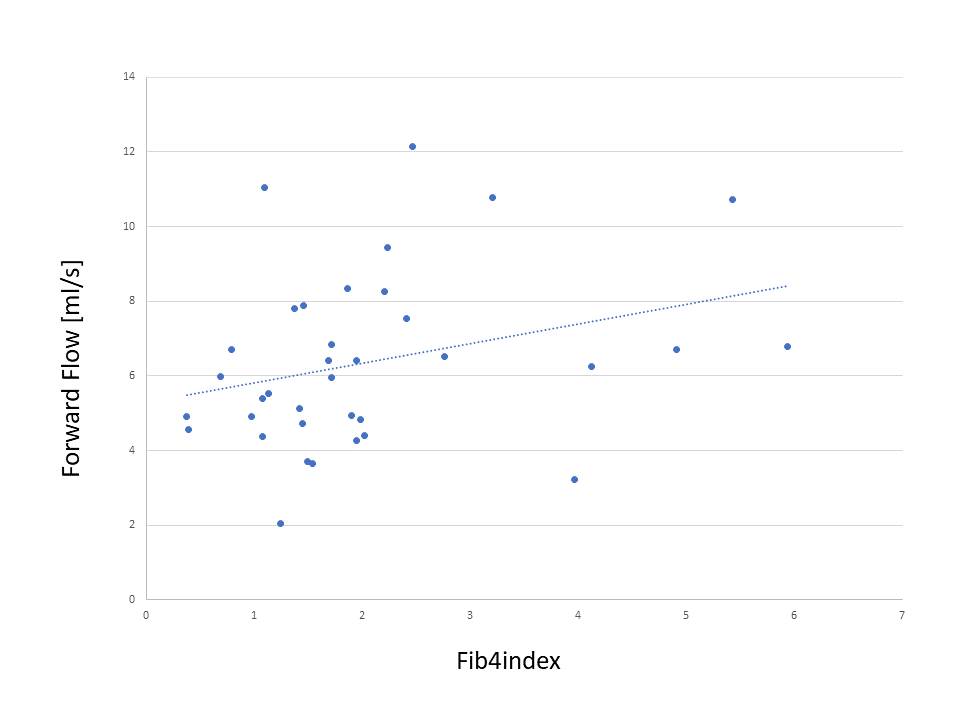
For the early diagnosis of portal hypertension, the relationship between portal venous hemodynamic changes and degree of liver fibrosis was evaluated using abdominal 4D-flow MR imaging. Flow quantification was performed in the middle part of the portal trunk. The forward flow was significantly correlated with Fib-4 index. In the comparison between the three groups divided by the degree of fibrosis, only the average velocity was significantly different. As the liver fibrosis progressed, the forward flow of the portal vein increased. The average velocity of the portal vein may be useful for early diagnosis of liver fibrosis.
INTRODUCTION
INTRODUCTION: Portal hypertension is most often caused by liver cirrhosis and has serious clinical symptoms related to prognosis such as gastrointestinal varices, encephalopathy, ascites, and splenomegaly. Diagnosis may be made by anatomically identifying the dilated collateral circulation by CT or MRI. However, this is a finding of advanced portal hypertension. Although Doppler ultrasonography is widely used, it has limited inter-observer reproducibility. There is currently no established method for early diagnosis of portal hypertension. Recently, abdominal 4D-flow MR imaging has been developed, and it has become possible to perform hemodynamic analysis1-4. The purpose of this study was to evaluate the relationship between portal venous hemodynamic changes and degree of liver fibrosis for the early diagnosis of portal hypertension.METHODS
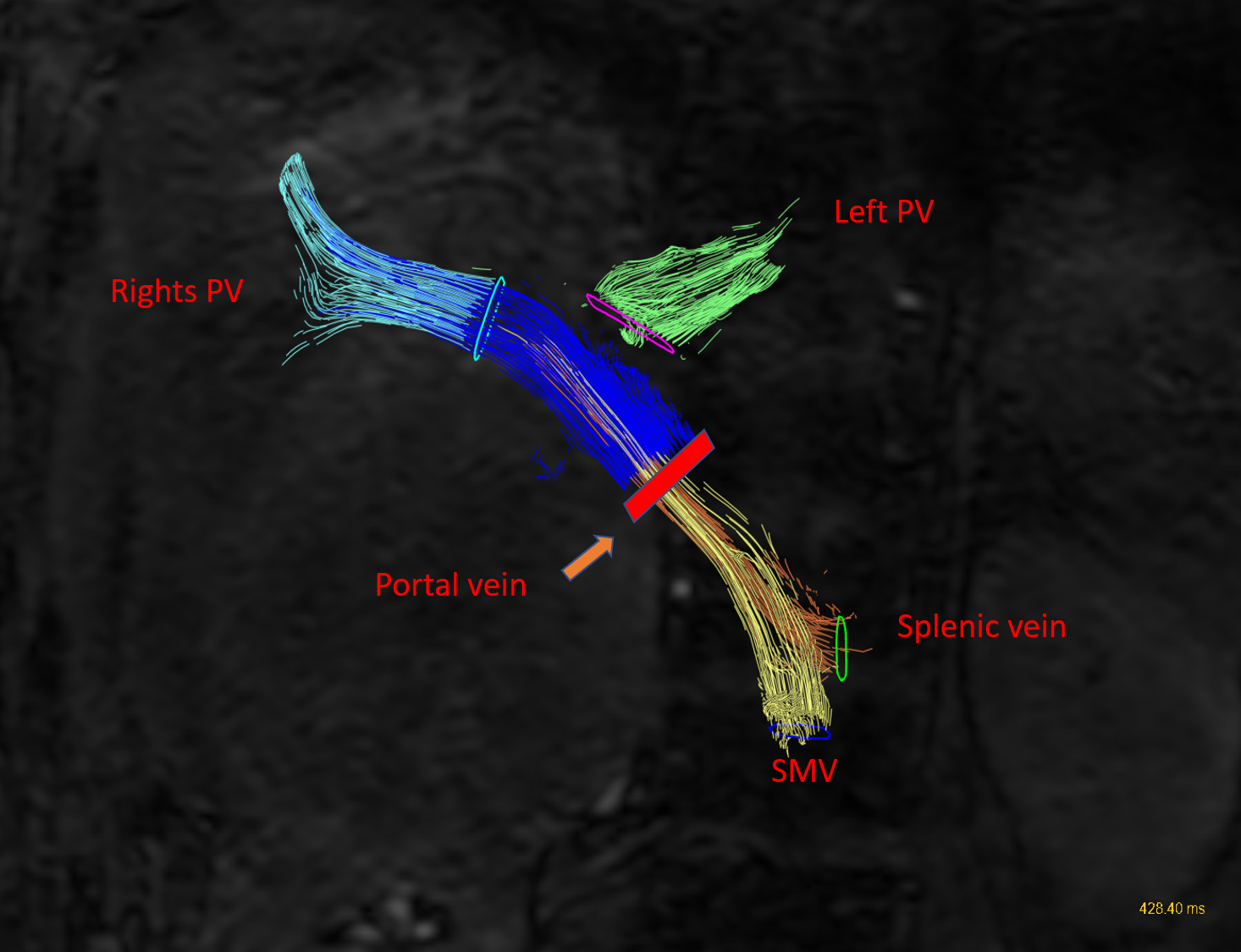
A total of 37 patients with (n=20) and without (n=17) chronic liver disease underwent an abdominal 4D-flow MR imaging between November 2019 and March 2020 were investigated. Flow quantification using 4D-flow MR imaging was performed in the middle part of the portal trunk. Quantitative values such as the area (mm2), the net flow (ml/s), the forward flow (ml/s), the backward flow (ml/s), the backward flow rate (%), the average velocity (cm/s), the average wall shear stress magnitude (N/m2), and the average axial wall shear stress (N/m2) were compared with fib-4 index to evaluate the relationship with the degree of liver fibrosis. The threshold values of Fib-4 score 1.3 and 2.67 were used to divide into the three groups (group A: Fib-4 score < 1.3, group B: Fib-4 score 1.30–2.67, group C: Fib-4 score > 2.67). Then, comparison between groups was performed. Statistical analysis was performed using Spearman's rank Correlation Coefficient, Kruskal-Wallis test, and Mann-Whitney U test.RESULTS
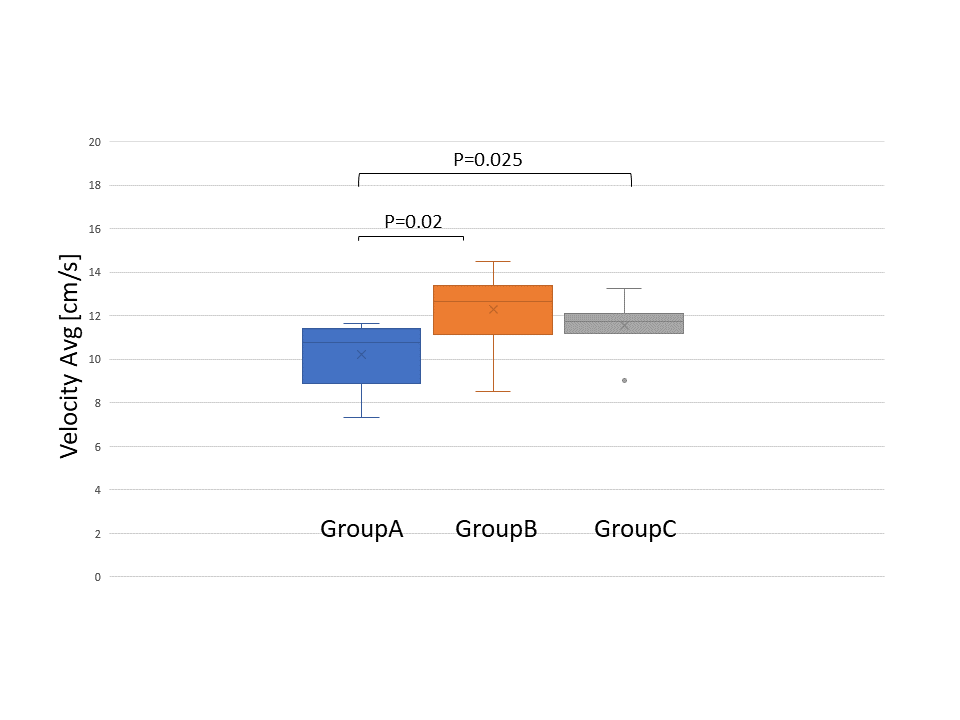
As a result of univariate analysis, the forward flow was significantly correlated with Fib-4 index (p=0.042, rs=0.341). The other quantitative values were not significantly correlated with Fib-4 index. In the comparison between the three groups, only the average velocity was significantly different (p=0.005). Group A (mean 10.23 cm/s, range 7.32 to 11.66) was significantly different from group B (mean 12.27 cm/s, range 8.51 to 14.47) (p=0.02) and group C (mean 11.55 cm/s, range 9.04 to 13.24) (p=0.025), and there was no significant difference between group B and group C.DISCUSSION
These results would be clinically important to predict and detect early signs of liver fibrosis and portal hypertension in making the treatment strategy for chronic liver disease. Hyperdynamic syndrome and decreased intestinal vascular resistance caused by liver fibrosis are considered to be the mechanism of increased portal flow. The present results may need further validation in prospective studies with a larger number of patients.CONCLUSION
As the liver fibrosis progressed, the forward flow of the portal vein increased. The average velocity of the portal vein may be useful for early diagnosis of liver fibrosis.Acknowledgements
I would like to express the deepest appreciation to the members of this research team.References
REFERENCES:
1. Peter Bannas, Alejandro Roldán-Alzate, Kevin M Johnson, et al. Longitudinal Monitoring of Hepatic Blood Flow before and after TIPS by Using 4D-Flow MR Imaging. Radiology. 2016;281(2):574-582.
2. Hadrien Dyvorne , Ashley Knight-Greenfield, Guido Jajamovich. Abdominal 4D Flow MR Imaging in a Breath Hold: Combination of Spiral Sampling and Dynamic Compressed Sensing for Highly Accelerated Acquisition. Radiology. 2015;275(1):245–254.
3. Zoran Stankovic, Zoltan Csatari, Peter Deibert, et al. Normal and altered three-dimensional portal venous hemodynamics in patients with liver cirrhosis. Radiology. 2012;262(3):862–873.
4. Octavia Bane, Steven Peti, Mathilde Wagner, et al. Hemodynamic measurements with an abdominal 4D flow MRI sequence with spiral sampling and compressed sensing in patients with chronic liver disease. J Magn Reson Imaging. 2019;49(4):994-1005.
Figures