2654
Reduction of contrast agent dose in cardiovascular MR angiography using deep learning
Javier Montalt-Tordera1, Michael Quail1, Jennifer Anne Steeden1, and Vivek Muthurangu1
1Centre for Cardiovascular Imaging, UCL Institute of Cardiovascular Science, University College London, London, United Kingdom
1Centre for Cardiovascular Imaging, UCL Institute of Cardiovascular Science, University College London, London, United Kingdom
Synopsis
Contrast-enhanced MR angiography (CE-MRA) is often used in cardiovascular MRI, but contrast agents can have adverse effects. This work proposes to use deep learning to reduce contrast dose by 80%. A deep neural network was trained to enhance low-dose images using a synthetically generated dataset and validated with both synthetic and real low-dose images. The method was assessed for image quality, diagnostic accuracy and confidence and accuracy of vessel measurements. Enhanced low-dose images were found to be comparable to reference high-dose data. Therefore, the method could enable a reduction in contrast dose for CMR.
Introduction
Gadolinium contrast-enhanced magnetic resonance angiography (CE-MRA) is commonly used to assess thoracic vascular structures 1, but the use of gadolinium carries a risk of adverse effects and is relatively costly 2,3. Dose reduction would be beneficial but results in poorer vessel depiction. This work proposes to use deep learning to enhance low-dose images in a postprocessing step, as previously suggested for brain MRA 4. In this work a library of reference high-dose images was used to simulate low-dose angiograms (20% of normal dose) and the resulting pairs were used to train a deep neural network. The network was then validated in 40 prospectively acquired low-dose images.Methods
Preparation of training data. Cardiovascular CE-MRA images were collected retrospectively from 1,173 patients who had been previously scanned at our institution. Each examination contained a pre-contrast image and a post-contrast image acquired with a high dose (HD-MRA). For each patient, a corresponding low-dose MRA (LD-MRA) with reduced blood signal intensity was synthesized by subtracting the pre-contrast image from the post-contrast image, multiplying by a factor R and adding back to the pre-contrast image (Figure 1B). The scaling factor R was derived from the prospective dataset (LD-MRA and HD-MRA images from 40 patients, see below for details) by comparing signal intensities in contrast-enhancing tissue for both low-dose and high-dose data (Figure 1A). The factor R was approximately normally distributed with mean 0.331 and variance 5.84 × 10−3.Network architecture, training and validation. A residual U-Net 5 was trained to map from LD-MRA to HD-MRA by minimizing the L2-loss, using Adam with an initial learning rate of 10−3. A 90:10 train-validation split was used. Network performance was evaluated using structural similarity index (SSIM) and peak signal-to-noise ratio (PSNR). Images enhanced with the neural network are referred to as enhanced low-dose MRA (ELD-MRA).
Prospective clinical study. 40 children and adults who were undergoing a clinically indicated CE-MRA were recruited for this study. MRA images were collected using a routine Cartesian gradient echo (GRE) sequence. For each patient, the contrast dose was split in two in order to collect an LD-MRA angiogram (20% of the dose) followed by an HD-MRA angiogram (remaining 80%). The full dose was 0.2 mmol/kg body weight of gadoteric acid (Dotarem®, Guerbet, Villepinte, France) up to 10 mmol.
Validation on prospective data. Real low-dose images from the prospective study were enhanced using the proposed method. Image quality was evaluated for LD, ELD and HD-MRA in terms of signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR) and edge sharpness (ES), which were computed as previously described 6. In addition, perceptual quality was rated on a Likert scale (1 = non-diagnostic, 2 = poor, 3 = adequate, 4 = good, 5 = excellent) in two categories: sharpness and contrast. To assess diagnostic accuracy and confidence, two CMR specialists were asked to identify the presence of the following conditions: aortic coarctation, aortic dilatation, abnormal arch anatomy and stenosis of main, left or right pulmonary arteries. In each case, they rated the likelihood that the abnormality is present on a 5-point Likert scale (1 = Definitely not present, 2 = Probably not present, 3 = Unclear, 4 = Probably present, 5 = Definitely present). Sensitivity, specificity and confidence were then calculated as previously described 7. Finally, diameters of the ascending/descending aorta and main/left/right pulmonary arteries were measured from cross-sectional images of the corresponding vessel. SSIM, PSNR, SNR, CNR and edge sharpness were compared using one-way repeated measures ANOVA and post hoc t-tests with Holm correction. Likert data was compared using Friedman’s test and post hoc Wilcoxon signed-rank tests with Holm correction. Diagnostic accuracy was compared using McNemar’s test and vessel diameters were compared using Bland-Altman analysis.
Results
The proposed method achieved a validation SSIM of 0.914 and a PSNR of 35.2, compared to 0.852 and 25.3 for synthetic low-dose images, a difference which was statistically significant (p < 0.001). In the prospective data, image quality was significantly better for enhanced images than low-dose images across all metrics (p < 0.001), and comparable to high-dose image quality (Figure 2). Diagnostic accuracy was comparable between groups, with no statistically significant differences (Figure 3A). Diagnostic confidence was significantly higher for enhanced images than low-dose images (p < 0.01) and comparable to high-dose images (Figure 3B). Vessel diameters were found to agree well in all groups, with no statistically significant differences and low bias and limits of agreement (Figure 4). Figure 5 shows examples of low-dose, enhanced and high-dose images from the prospective patient population.Discussion
This work presents a deep learning method to reduce contrast dose in cardiovascular CE-MRA by 80% without compromising image quality or clinical utility. The quality of low-dose images enhanced using this method was superior to that of low-dose images and comparable to high-dose images. The same was true of diagnostic confidence. Results also indicate that reliable vessel measurements can be extracted from enhanced images. Data on diagnostic accuracy are encouraging, although too sparse to draw definitive conclusions. Therefore, we think the technique is a promising way to limit contrast agent dose in cardiovascular CE-MRA, with associated reduction in risk of adverse effects and cost.Acknowledgements
No acknowledgement found.References
- Schneider G, Ahlhelm F, Seidel R, et al. Contrast-enhanced cardiovascular magnetic resonance imaging. Top Magn Reson Imaging. 2003;14(5):386-402. doi:10.1097/00002142-200310000-00005
- Kuo PH, Kanal E, Abu-Alfa AK, Cowper SE. Gadolinium-based MR contrast agents and nephrogenic systemic fibrosis. Radiology. 2007;242(3):647-649. doi:10.1148/radiol.2423061640
- Gulani V, Calamante F, Shellock FG, Kanal E, Reeder SB. Gadolinium deposition in the brain: summary of evidence and recommendations. Lancet Neurol. 2017;16(7):564-570. doi:10.1016/S1474-4422(17)30158-8
- Gong E, Pauly JM, Wintermark M, Zaharchuk G. Deep learning enables reduced gadolinium dose for contrast-enhanced brain MRI. J Magn Reson Imaging. 2018;48(2):330-340. doi:10.1002/jmri.259705.
- Jin KH, McCann MT, Froustey E, Unser M. Deep convolutional neural network for inverse problems in imaging. IEEE Trans Image Process. 2017;26(9):4509-4522. doi:10.1109/TIP.2017.27130996.
- Steeden JA, Atkinson D, Hansen MS, Taylor AM, Muthurangu V. Rapid flow assessment of congenital heart disease with high-spatiotemporal-resolution gated spiral phase-contrast MR imaging. Radiology. 2011;260(1):79-87. doi:10.1148/radiol.111018447.
- Steeden JA, Quail M, Gotschy A, et al. Rapid whole-heart CMR with single volume super-resolution. J Cardiovasc Magn Reson. 2020;22(1):56. doi:10.1186/s12968-020-00651-x
Figures
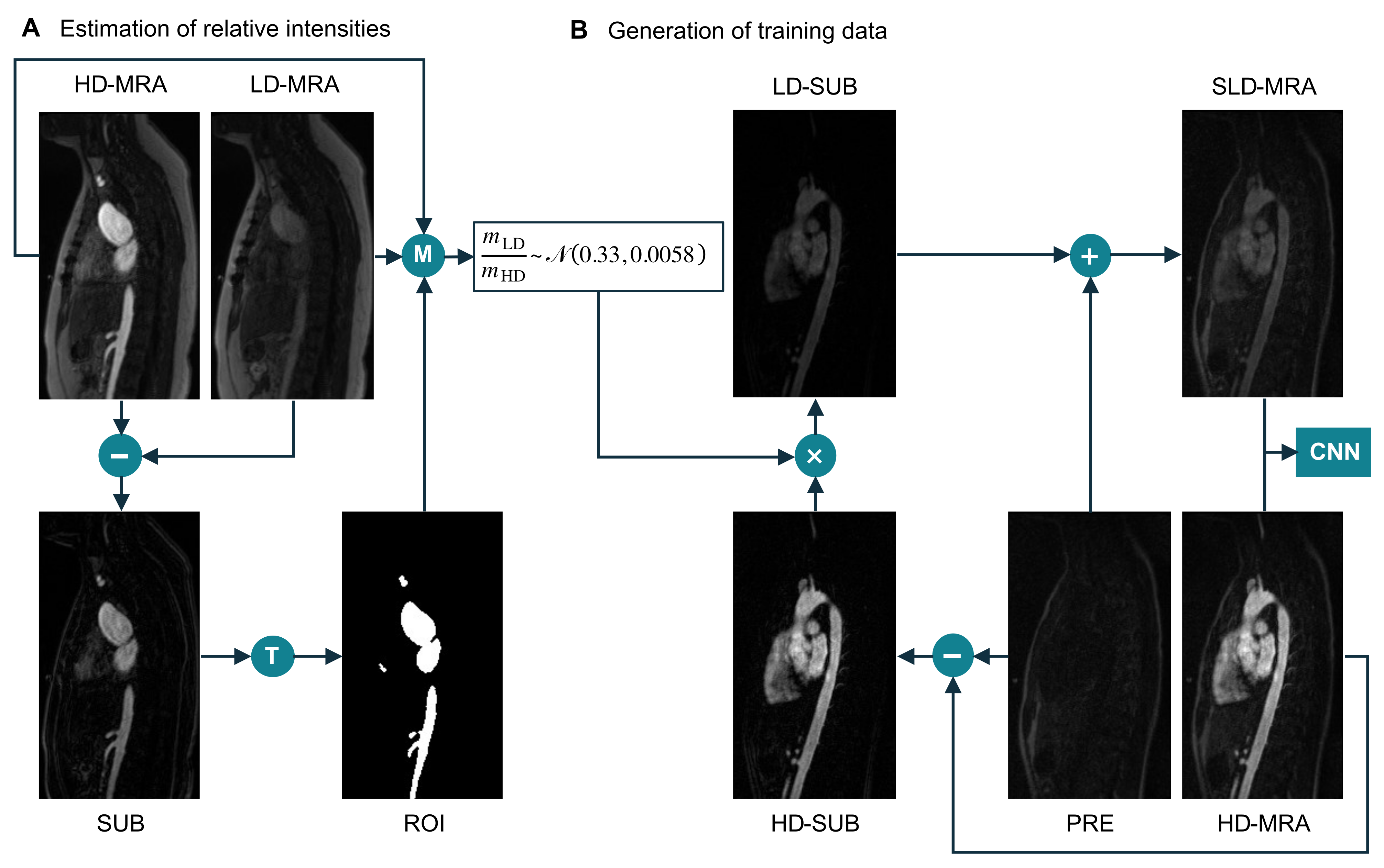
Figure 1. (A) Estimation of the intensity ratio between low-dose data (LD-MRA) and high-dose data (HD-MRA). T: thresholding followed by morphological opening. M: compute mean over ROI for both images. (B) Generation of synthetic low-dose (SLD-MRA) images, using the estimated intensity ratio, to be paired with the corresponding high-dose (HD-MRA) images for training.
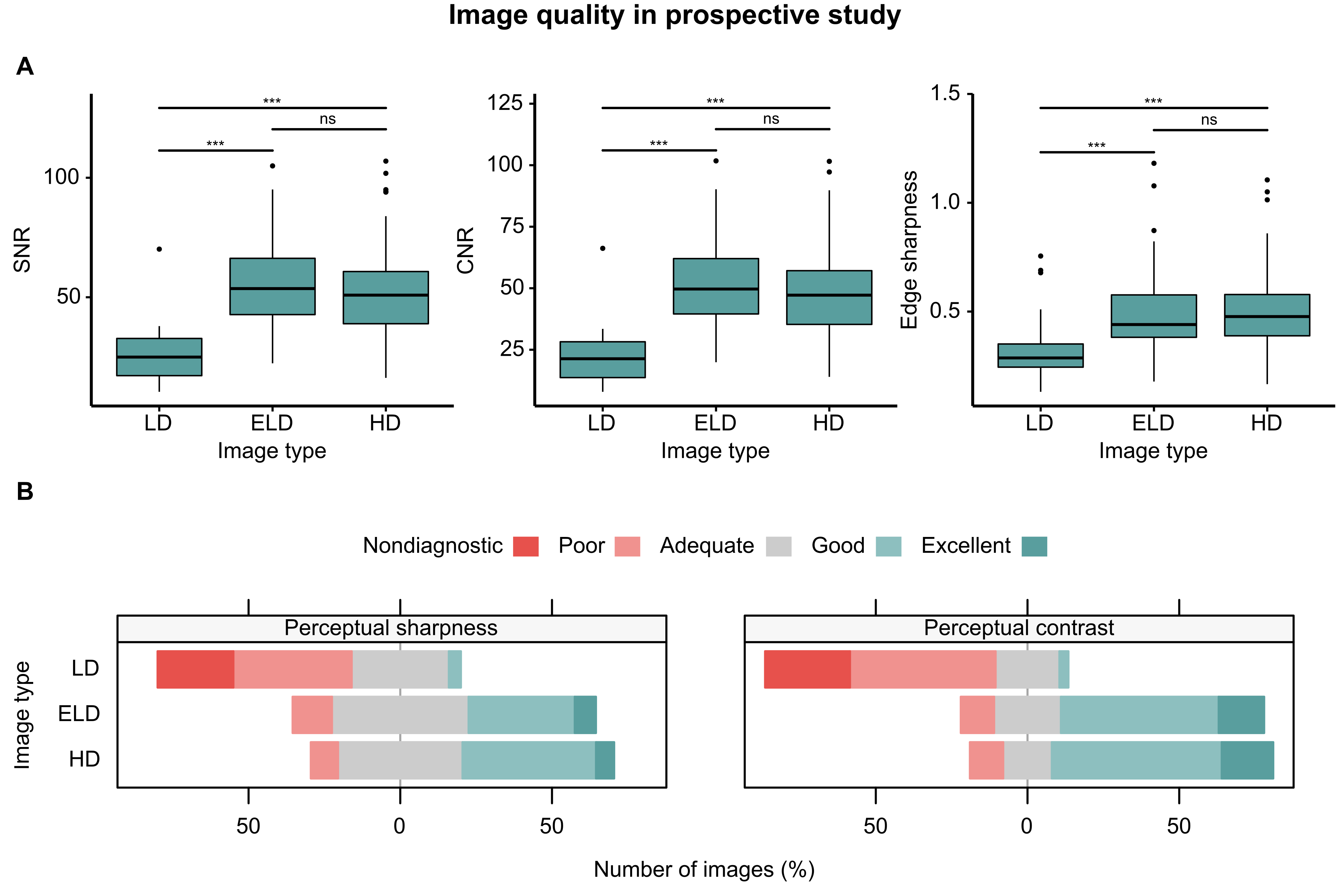
Figure 2. Image quality in prospective study. (A) Objective image quality metrics: signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR) and edge sharpness. (B) Perceptual image quality in terms of sharpness and contrast, as rated by a CMR specialist. ***: p < 0.001; ns: nonsignificant.
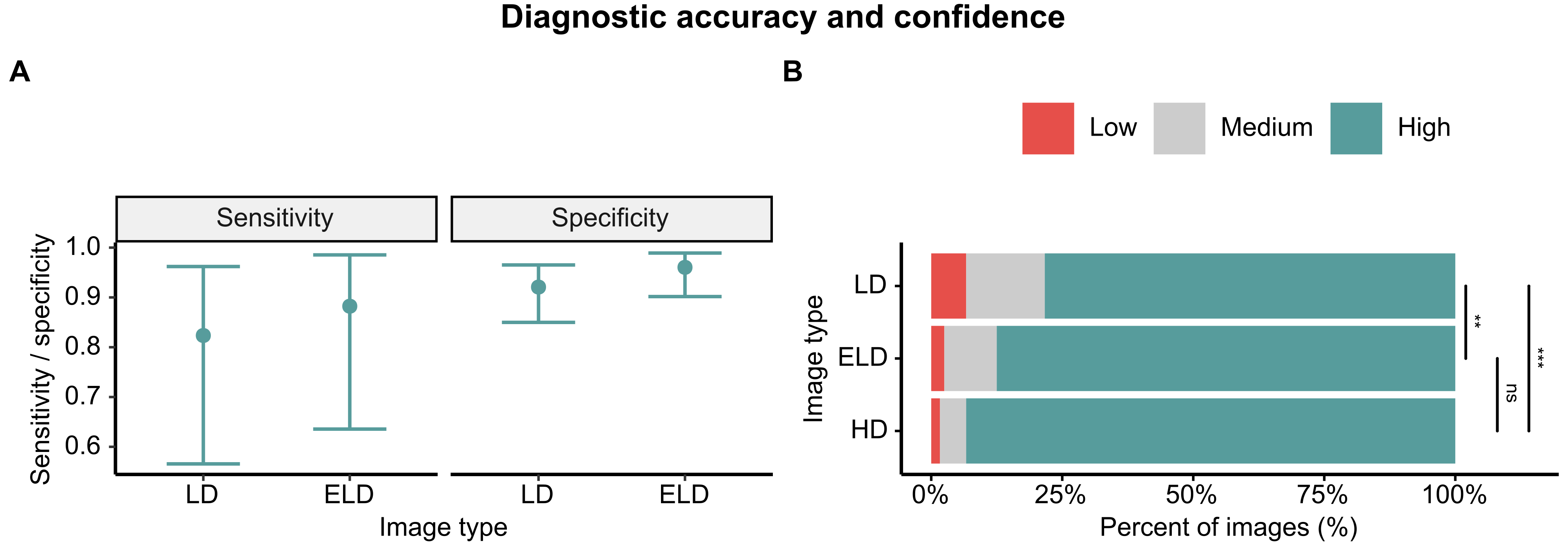
Figure 3. Diagnostic accuracy and confidence. (A) Sensitivity and specificity for the detection of lesions in LD and ELD-MRA images with 95% confidence intervals. (B) Confidence expressed in diagnosis based on LD, ELD and HD-MRA images. Confidence levels: low, “unclear if condition present”; medium, “condition probably (not) present”; high, “condition definitely (not) present”. **: p < 0.01, ***: p < 0.001, ns: nonsignificant.
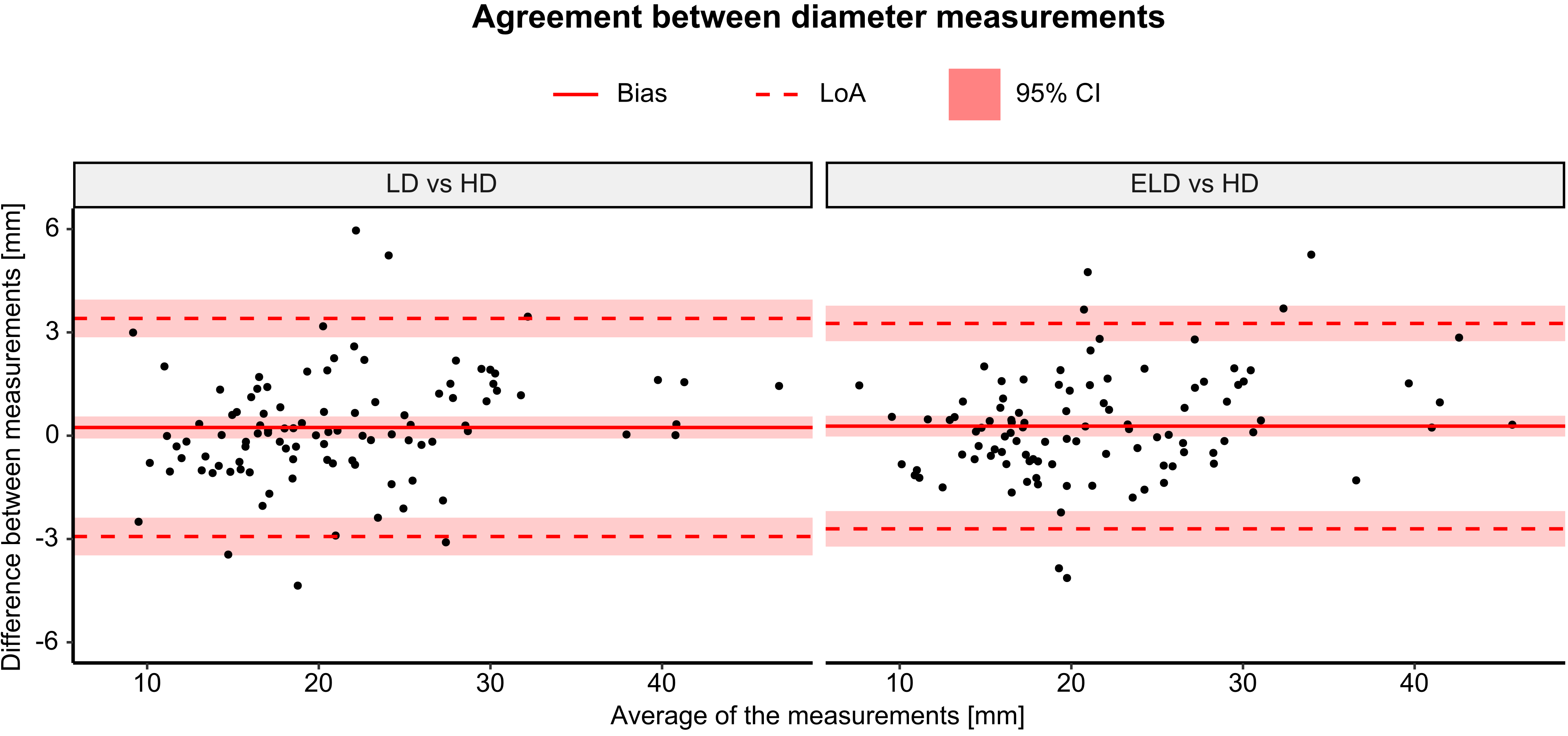
Figure 4. Bland-Altman plots of agreement between diameter measurements. LoA: limits of agreement; CI: confidence interval.
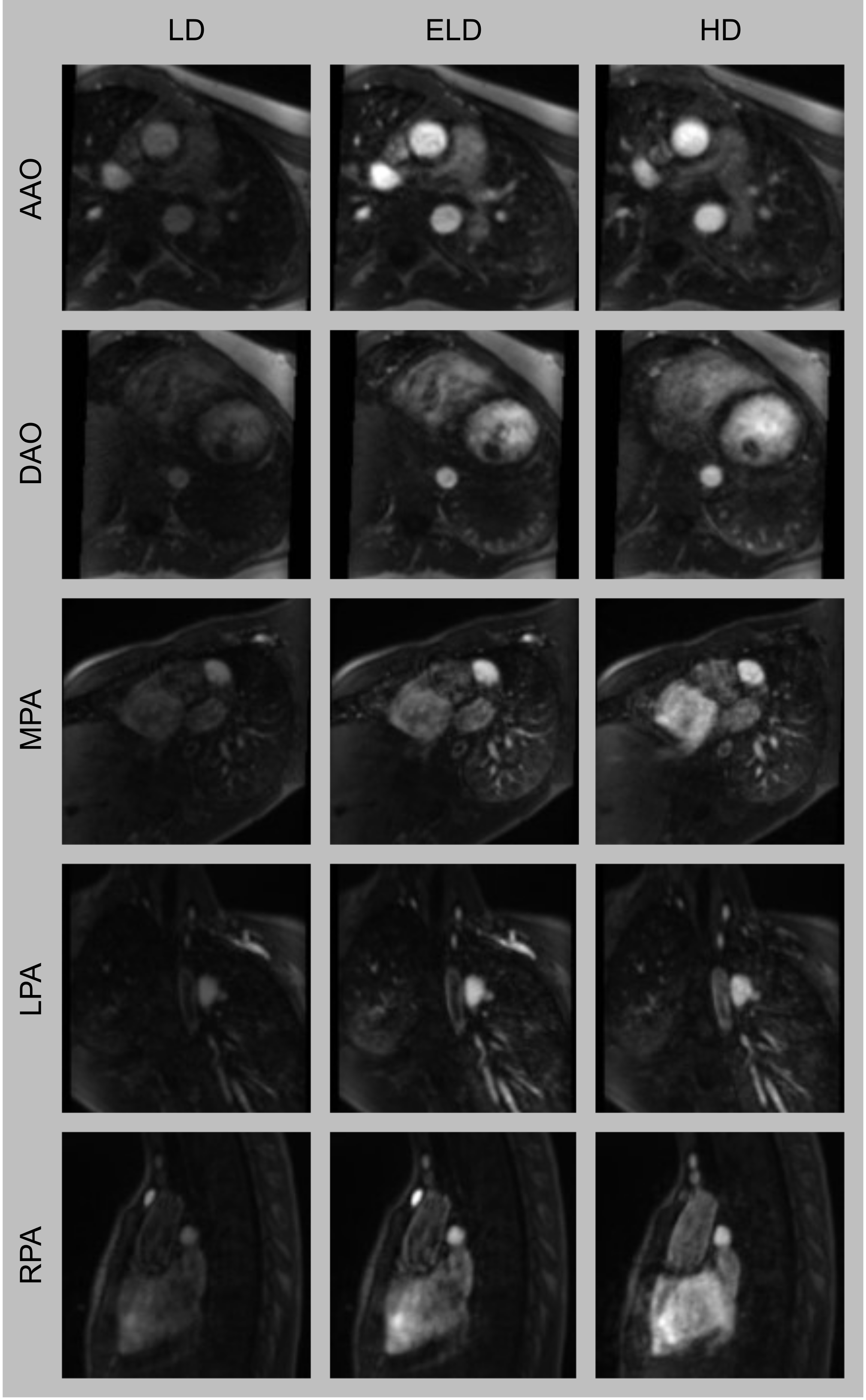
Figure 5. Representative images from the prospective study. Multiplanar reformats of the ascending aorta (AAO), descending aorta (DAO), main pulmonary artery (MPA), left pulmonary artery (LPA) and right pulmonary artery (RPA).