2585
Fast 3D Wave-CAIPI Susceptibility Weighted Imaging and SPACE FLAIR for Comprehensive Evaluation of Demyelinating Lesions in Multiple Sclerosis1Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 2Department of Radiology, Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA, United States, 3Department of Radiology, Siriraj Hospital, Bangkok, Thailand, 4Department of Neurology, Massachusetts General Hospital, Boston, MA, United States, 5Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 6Siemens Healthcare GmbH, Erlangen, Germany, 7Siemens Medical Solutions Inc., Boston, MA, United States
Synopsis
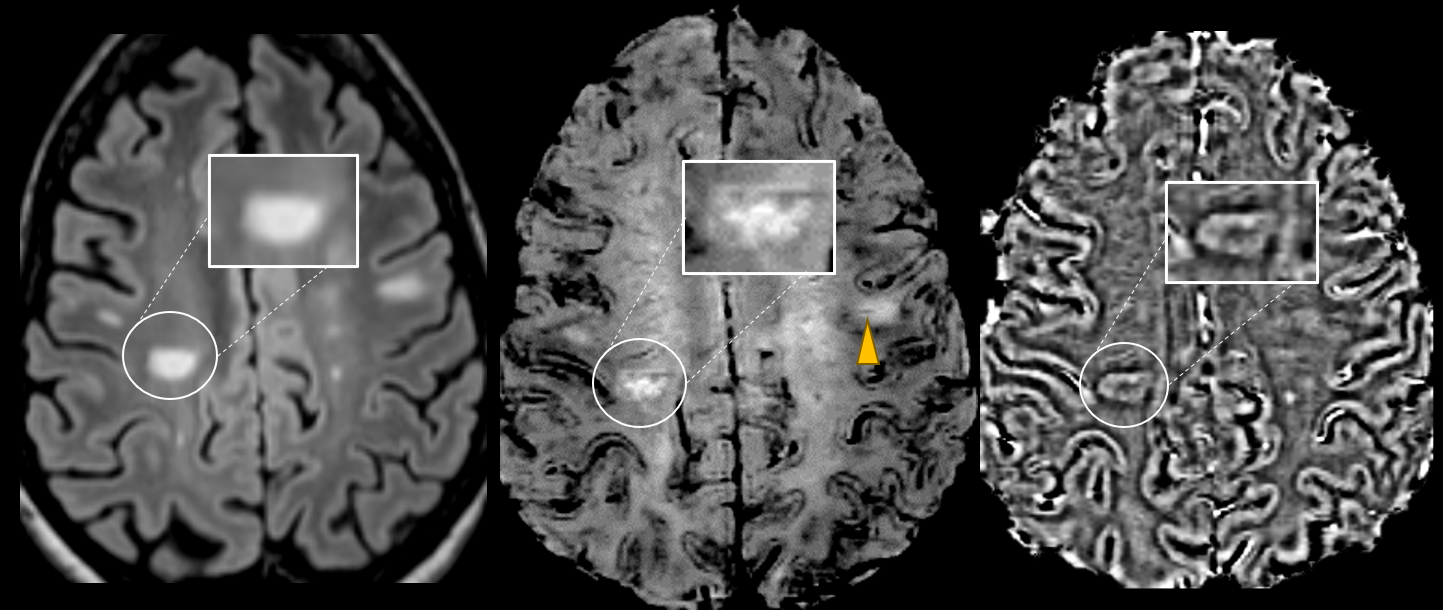
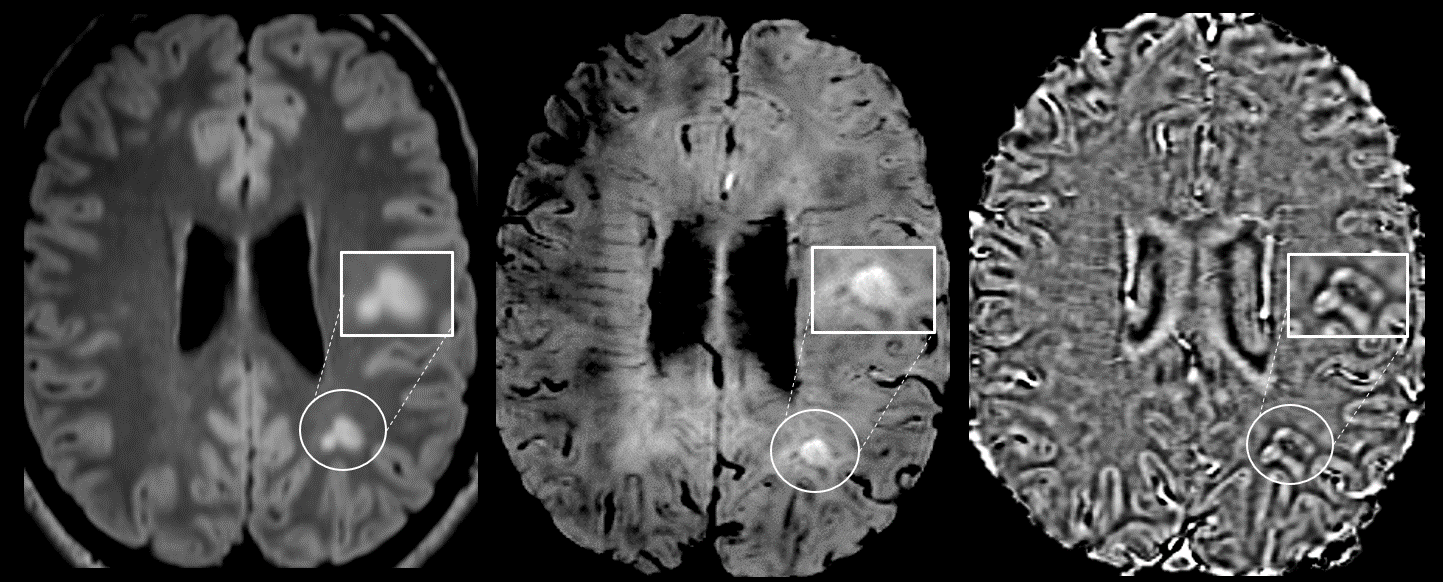
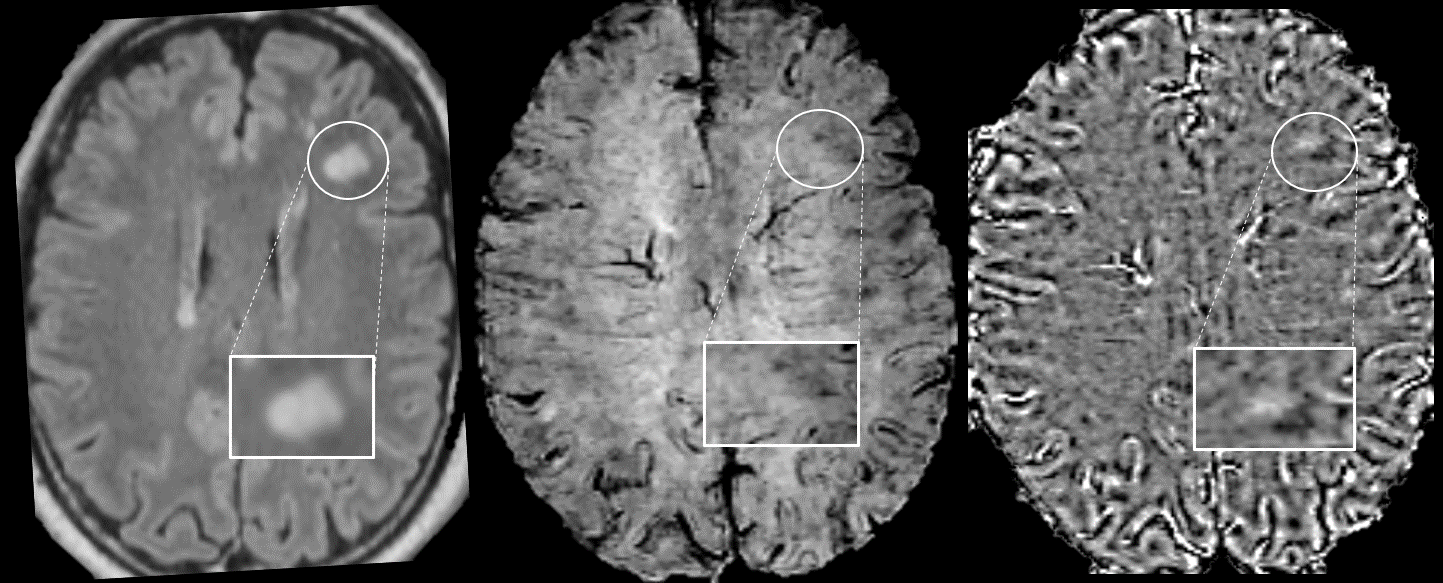
The central vein sign (CVS) and paramagnetic rims are imaging signs specific for demyelinating lesions in multiple sclerosis (MS) that can be detected using high-resolution susceptibility-weighted imaging (SWI) and FLAIR sequences. We developed an optimized protocol for fast, comprehensive evaluation of demyelinating lesions including highly accelerated Wave-CAIPI SWI and FLAIR. In 65 patients undergoing evaluation for demyelinating disease, we found that 72% of MS and CIS patients had at least one CVS, and 45% showed at least one paramagnetic rim. The application of highly accelerated Wave-SWI and Wave-FLAIR may improve the characterization of MS lesions in clinically feasible acquisition times.
Introduction
Magnetic resonance imaging (MRI) is widely used to characterize demyelinating lesions in the brain and establish an earlier diagnosis of multiple sclerosis (MS). Previous studies have suggested that the central vein sign (CVS) is specific for multiple sclerosis (MS) and that paramagnetic rims seen in chronic active MS plaques are associated with more aggressive disease1,2. A major barrier to the more widespread use and assessment of these imaging signs is the long acquisition time associated with the high-resolution FLAIR and susceptibility-based MRI sequences used to identify the CVS and paramagnetic rim sign. The goal of this study was to assess the frequency of paramagnetic rims and CVS using highly accelerated 3D Wave-CAIPI susceptibility-weighted imaging (Wave-SWI) and FLAIR (Wave-FLAIR) sequences for the adjunct characterization of demyelinating lesions in MS within clinically feasible scan times.Methods
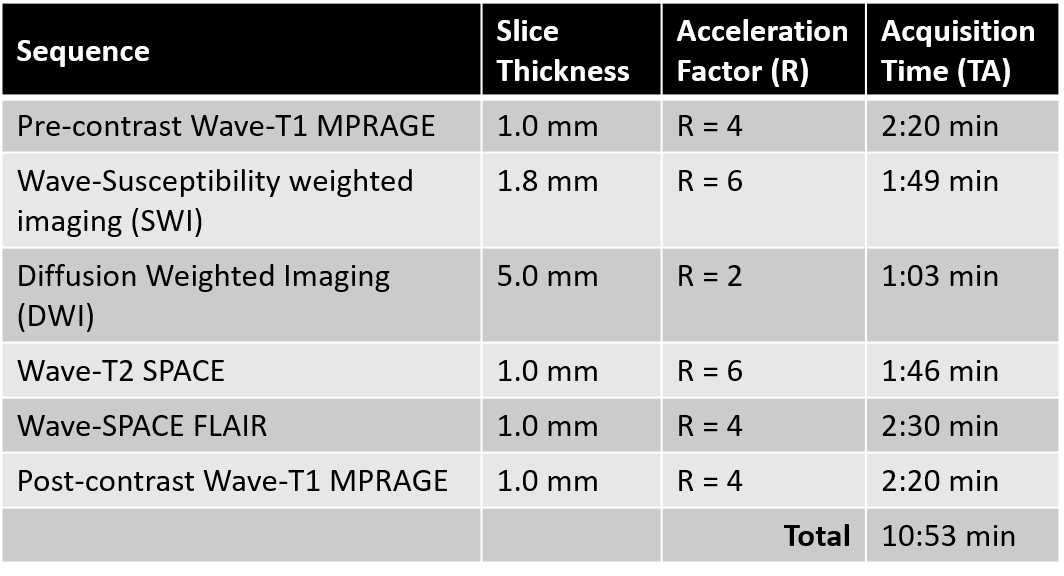
This study was approved by the IRB and was HIPAA compliant. 65 consecutive patients undergoing brain MRI for the clinical evaluation of demyelinating disease from June-October 2020 were scanned on 3T MRI systems (MAGNETOM Prisma and Vida, Siemens Healthcare, Erlangen, Germany). The imaging protocol included accelerated prototype 3D Wave-SWI (acceleration factor [R]=6, acquisition time [TA]=1:58min, 0.8x0.8x1.8mm) and 3D Wave-FLAIR (R=4, TA=2:30min, 1x1x1mm) sequences. Taken together with other sequences used in the protocol (Table 1), the Wave-FLAIR and Wave-SWI sequences helped to shorten the clinical MS protocol from 30 min to <20 min. Each patient’s Wave-FLAIR and Wave-SWI images were co-registered using built-in 3D registration software within the PACS (Visage). Two neuroradiologists (9 and 13 years of experience) blinded to clinical diagnosis independently reviewed the co-registered image series and determined the number of lesions with paramagnetic rims and/or CVS. Discrepancies between raters were discussed, and consensus was reached on the number of lesions with paramagnetic rims and CVS per case. We calculated the proportion of confirmed MS or clinically isolated syndrome (CIS) patients with paramagnetic rim lesions and/or CVS. We also assessed the agreement between raters in their independent review.Results
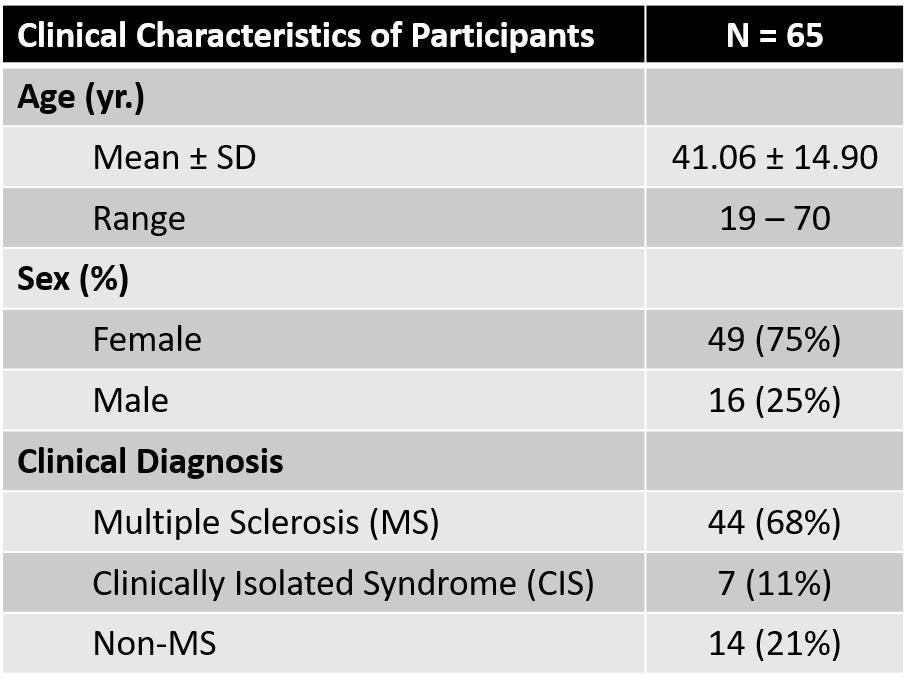
Of the 65 patients evaluated in this study, 44 patients (68%) had confirmed MS by 2017 McDonald criteria, 7 had clinically isolated syndrome (CIS) (11%), and the remaining 14 had a non-MS diagnosis (21%)[IG(1] . Of the 51 patients with MS or CIS, paramagnetic rims were identified in 23 cases (45%). 37 cases had at least one lesion with CVS (72.5%). There was substantial agreement between raters in the visualization of paramagnetic rims before consensus (89.23% - Cohen k = 0.75, p < 0.01). No paramagnetic rims or CVS were identified in the non-MS patients.Discussion
The frequencies of paramagnetic rims and CVS identified on highly accelerated 3D Wave-SWI and Wave-FLAIR sequences in our cohort were comparable to those reported by other groups using longer sequences with standard image encoding techniques1. MR imaging-pathologic correlation studies have reported that paramagnetic rims on susceptibility-based MRI identify a subset of MS lesions with compartmentalized inflammation at the lesion boundary and associated failure of remyelination2. Considering that T2/FLAIR images alone are unable to separate chronic active lesions from inactive stable demyelination, SWI may help in distinguishing them. Moreover, the paramagnetic rims that are seen in chronic active MS plaques are associated with more aggressive disease3 and can aid in the identification of persistent perilesional inflammation. Our findings suggest that it is feasible to implement a clinical MS MRI protocol with Wave-SWI and Wave-FLAIR sequences to provide additional information in the characterization of demyelinating lesions, thereby improving confidence in the diagnosis of MS and assessment of disease progression. The use of Wave-CAIPI accelerated images enable a more comprehensive protocol to be performed within 20 minutes of total acquisition time, without compromising exam throughput and patient comfort. The future adoption of susceptibility-weighted imaging in MS protocols may also prove to be a promising tool for more detailed assessment of disease activity and stratification of patients for neuroprotective therapy.Conclusion
The combined use of highly accelerated Wave-CAIPI SWI and FLAIR in clinical MRI protocols for the comprehensive evaluation of MS lesions can afford time-savings that may enable the more widespread adoption of imaging signs such as the paramagnetic rim sign and CVS in the clinical follow-up and evaluation of patients with suspected or confirmed multiple sclerosis.Acknowledgements
This study was supported by a research grant from Siemens Healthineers.References
1. Clarke MA, Pareto D, Pessini-Ferreira L, et al. Value of 3T susceptibility-weighted imaging in the diagnosis of multiple sclerosis. Am J Neuroradiol. 2020;41(6):1001-1008. doi:10.3174/ajnr.A6547
2. Dal-Bianco A, Grabner G, Kronnerwetter C, et al. Slow expansion of multiple sclerosis iron rim lesions: pathology and 7 T magnetic resonance imaging. Acta Neuropathol. 2017;133(1):25-42. doi:10.1007/s00401-016-1636-z
3. Absinta M, Sati P, Masuzzo F, et al. Association of Chronic Active Multiple Sclerosis Lesions with Disability in Vivo. JAMA Neurol. 2019;76(12):1474-1483. doi:10.1001/jamaneurol.2019.2399
Figures