2583
NODDI in detecting cognitive decline in patients with radiation-induced brain injury: comparison with DTI1Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, China, 2MR Scientific Marketing, Siemens Healthcare, Guangzhou, China
Synopsis
This study aimed to demonstrate the feasibility of neurite orientation dispersion and density imaging (NODDI) for in exploring the pathological mechanism of cognitive impairment in RI compared to DTI. We evaluated the differences of all diffusion parameters between patients with and without cognitive decline confirmed by Montreal Cognitive Assessment (MoCA) scores, as well as the correlation between diffusion maps and cognitive decline. Results demonstrated that NODDI was more sensitive than DTI in detecting cognitive decline in patients with radiation-induced brain injury. Cognitive decline in radiation-induced brain injury was associated with the reduction of neurite density
Introduction
Radiation-induced brain injury (RI) is a nonnegligible issue in patients treated by radiotherapy[1]. Some of them may suffer from aphasia, hemiplegic paralysis, dysphagia to seizures and neurocognitive decline depending on the region of the injury[2]. Clinically, cognitive decline could be assessed by series of scales including Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE)[3]. But its pathological mechanism needs to be further explored. Diffusion imaging, based on the Gaussian diffusion, provides a noninvasive way to probe the white matter integrity of brian, but their specific microstructural mechanisms remain unclear. Neurite Orientation Dispersion and Density imaging (NODDI), a more complex model with a combination of three basic compartments of CSF, extracellular, and intracellular, can quantitatively assess tissue characteristics[4]. The purpose of this study was to demonstrate the feasibility of NODDI in exploring the pathological mechanism of cognitive impairment in patients with RI.Methods
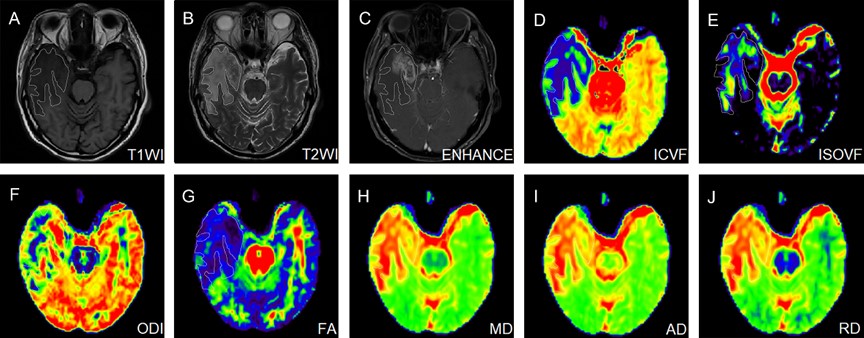
A total of 39 patients were collected in the study, 14 patients were with normal cognitive function while 25 patients had cognitive decline assessed by using Montreal Cognitive Assessment (MoCA) scores, and a total MoCA score of ≤ 25 is considered cognitive decline. All patients underwent MRI examinations on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) using a 20-channel head coil. Diffusion spectrum imaging (DSI) using q-space half coverage diffusion mode (TR/TE, 4900 ms/93 ms; flip angle, 90°; NEX,1; voxel dimension of 2 × 2 × 4 mm3; 32 slices; matrix, 110 × 110; FOV, 220 × 220 mm; ) along 128 gradient directions with maximum b-value at 2000 s/mm2 were performed to obtain diffusion-weighted (DW) data. All DW data were calculated by software (NeuDiLab) developed in-house based on the open-resource tool DIPY (Diffusion Imaging In Python, http://nipy.org/dipy). The parameters of NODDI, including intra-neurite volume fraction (ICVF), decreased orientation dispersion index (ODI) and volume fraction of the isotropic compartment (ISOVF) values, and DTI including fractional anisotropy (FA), mean diffusivity (MD), axial (AD) and radial diffusivity (RD) were calculated. For each patient, the maximum cross-sectional area of the edema focal on the T2WI was manually drawn as the region of interest (ROI) of the edema lesions of RI by visual inspection. And then the ROI was copied to all diffusion maps to calculate the corresponding average (figure 1). The differences of all diffusion parameters between patients with and without cognitive function impairment were analyzed by the Mann-Whitney U test. Logistic regression shown by odds ratio (OR) and corresponding 95% confidence interval (CI) were used to the correlation between diffusion maps and cognitive decline. Receiver operating characteristic (ROC) curve analysis was used to determine the level of diffusion parameters that provided the best sum of sensitivity and specificity. It was considered significant when the P-value <0.05.Results
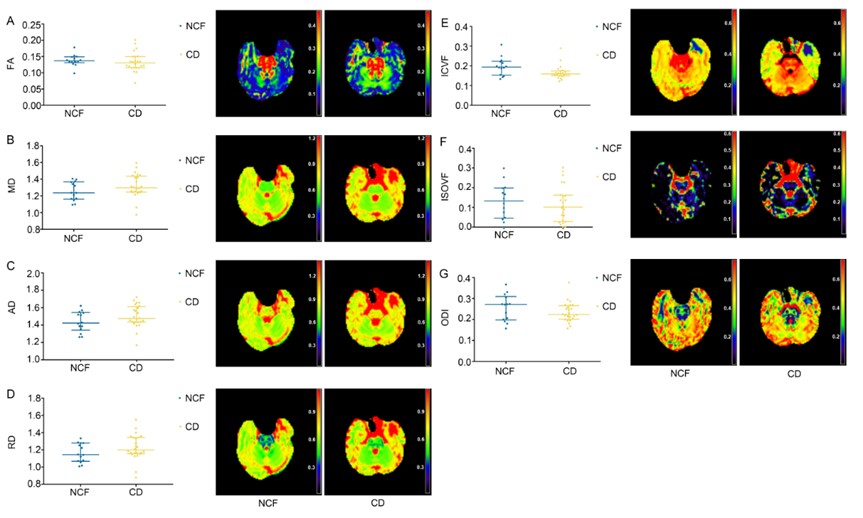
A comparison of diffusion parameters between patients with normal cognitive function and those with cognitive decline was shown in figure 2. The median of ICVF values (ICVFmedian) of the edema lesions in patients with cognitive decline was 0.16 (0.15-0.17), which was significantly decreased (P=0.037) compared with that of patients with normal cognitive function (ICVFmedian =0.19, range from 0.15 to 0.22). However, DTI parameters showed no differences between patients with cognitive decline and normal cognitive function. ICVF values of the edema lesions of RI were significantly associated with cognitive decline (P=0.048; OR, 0; 95%CI, 0, 0.85). According to the ROC curve analysis, the ICVFmedian < 0.18 was identified as the best threshold to be associated with cognitive decline.Discussion
ICVF values derived from NODDI model in patients with cognitive decline were significantly lower than that of patients with normal cognitive function. Furthermore, ICVF in RI was significantly correlated with cognitive decline while DTI indices showed no correlation. NODDI is more specific to characterize alterations of microstructural integrity than DTI. Therefore, NODDI was more sensitive and specific than conventional DTI in identifying the alterations of microstructural integrity and cognitive impairment in the RI.Conclusion
Decreased ICVF value in brain edema lesion indicated the reduction of neurite density, and was associated with cognitive decline in RI. NODDI as a new MRI diffusion technique may contribute to better understanding of pathophysiology of cognitive decline in RI.Acknowledgements
No acknowledgement found.References
[1].Yang, L., et al., Pathophysiological Responses in Rat and Mouse Models of Radiation-Induced Brain Injury. Mol Neurobiol, 2017. 54(2): p. 1022-1032.
[2].Stone, J.B. and L.M. DeAngelis, Cancer-treatment-induced neurotoxicity--focus on newer treatments. Nat Rev Clin Oncol, 2016. 13(2): p. 92-105.
[3].Tsoi, K.K., et al., Cognitive Tests to Detect Dementia: A Systematic Review and Meta-analysis. JAMA Intern Med, 2015. 175(9): p. 1450-8.
[4]. Chandana, K. et al. Age Effects and Sex Differences in Human Brain White Matter of Young to Middle-Aged Adults: A DTI, NODDI, and q-Space Study. Neuroimage. 2016 ; 128: 180–192
Figures