2394
Retrospective Cardiac Gating of Simultaneous Coherent/Incoherent Motion Imaging (SCIMI) in the Brain1GE Global Research Center, Niskayuna, NY, United States, 2Walter Reed National Military Medical Center, Bethesda, MD, United States, 3Uniformed Services University of the Health Sciences, Bethesda, MD, United States
Synopsis
We use retrospective cardiac gating with phase-sensitive reconstruction of diffusion tensor data to create a 4D profile of motion in brain parenchyma with velocity encoding value (VENC) of 0.18 mm/s. We imaged the brain of a healthy volunteer in regions surrounding the ventricles with synchronized recording of a PPG signal. We created a velocity profile for the volume spanning the full cardiac cycle by binning individual images according to the local cardiac phase. Results show coherent periodic motion with distinct systolic/diastolic phases. This motion is thought to comprise of both tissue movement and interstitial fluid flow (ISF) in the region.
Introduction
We previously reported on SCIMI reconstruction, which used a PPG-triggered diffusion tensor imaging (DTI) sequence to image sub-millimeter/second velocities with applications in imaging glymphatic circulation in the brain[1]. This method used the diffusion-encoding gradient pulses to simultaneously encode a VENC on the scale of 0.2 mm/s, while phase-sensitive reconstruction was used in parallel to the standard magnitude-based DTI recon to create velocity profiles. By running the sequence multiple times with various trigger delays, we created a limited sequence of “snapshots” over the course of the cardiac cycle showing pulsatility thought to be comprised of both tissue and ISF movement. In this work, we expand further on this technique by using retrospective gating to create a full 4D-movie that spans the full cardiac cycle in a volume with a single diffusion acquisition.Methods
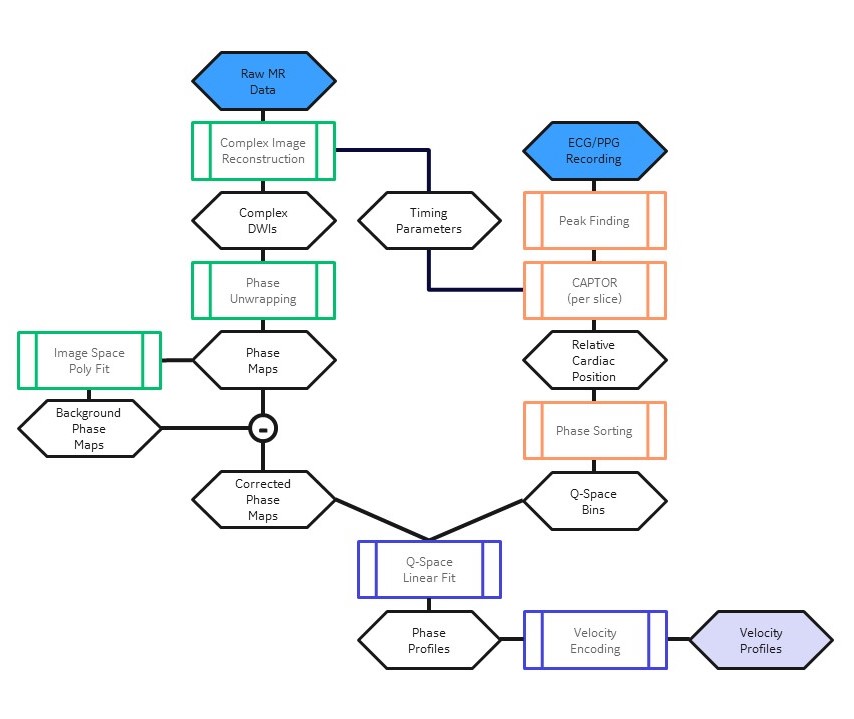
To improve angular resolution, DTI sequences often use a large number of q-space directions distributed in a sphere or more complex arrangements; meanwhile, phase-contrast imaging can be performed with 4 acquisitions to quantify 3-directional flow. The q-space redundancy inherent in phase-contrast reconstruction from a DTI acquisition allows for multiple velocity profiles to be reconstructed from a single scan. We modified the SCIMI sequence (diffusion + phase contrast imaging) to remove gated triggers and instead synchronize recording of the PPG signal (100 Hz sampling) with the scan. We imaged a healthy volunteer on a 3.0T SIGNA Architect (GE Healthcare, Waukesha, WI) scanner using a 36-channel head coil with a single-shell sequence (151 directions) with b = 1000 s/mm2 and VENC = 0.18 mm/sec. Figure 1 shows the reconstruction pipeline to generate 4D velocity images using the acquired data and cardiac recording. We divided the cardiac cycle into 10 bins based on the average R-R interval and used the timing parameters of the scan to sort each q-space direction into the corresponding cardiac bin using the CAPTOR method[2]. After dividing the average R-R interval into bins of equal time, the CAPTOR method determines where each bin lies in its respective cardiac phase (e.g., “15% systole” or “82% diastole”). A given timepoint is compared to the cardiac phase of the R-R interval that it lies in and binned accordingly. This method thus accounts for variability in individual R-R intervals, rather than relying on fixed delays to represent the cardiac phases. Each slice was assigned an individual set of timings to account for the order of slice acquisition and delay between each successive slice and therefore had different q-space directions assigned to each bin. Phase profiles for every bin were calculated based on the q-space directions in that bin.Results & Discussion
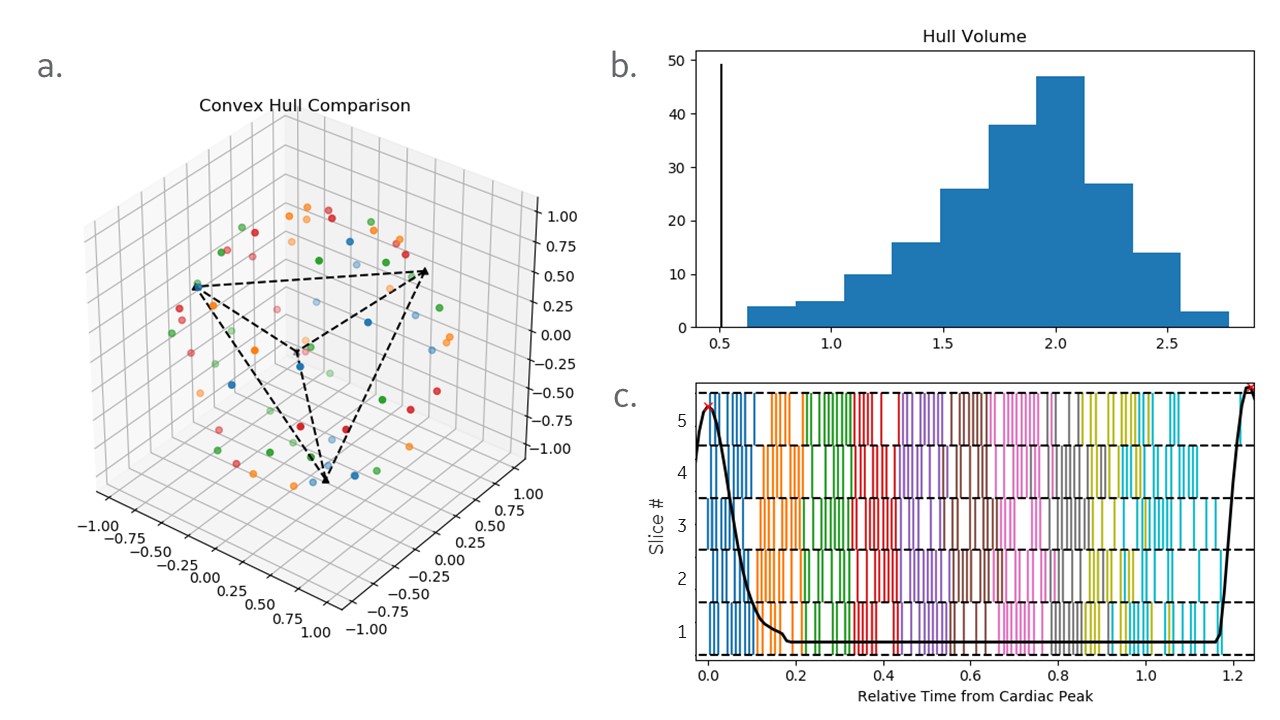
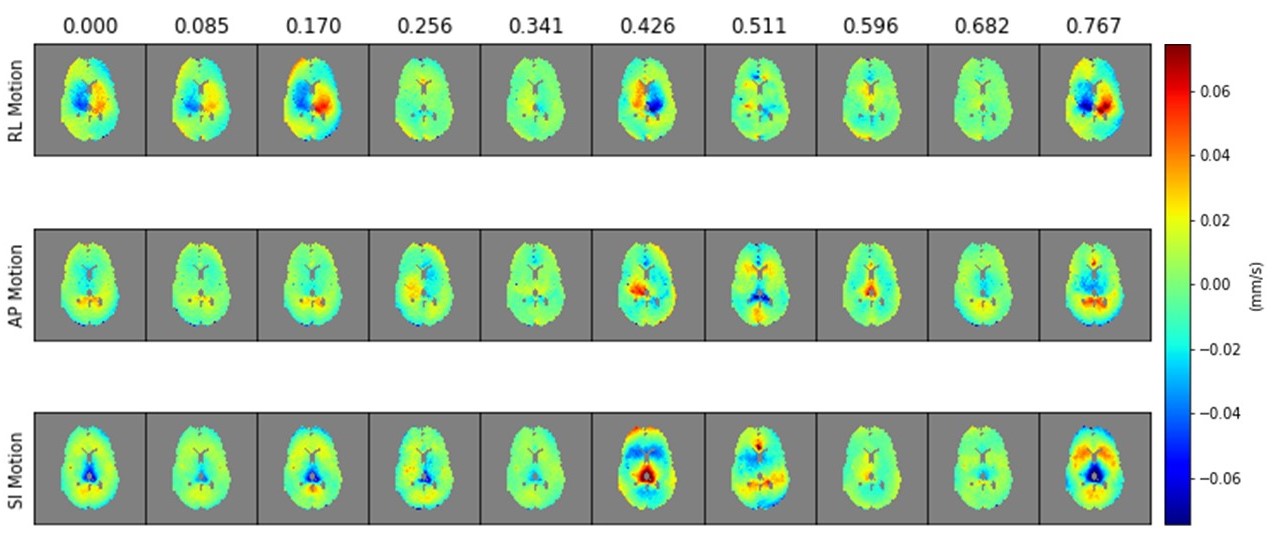
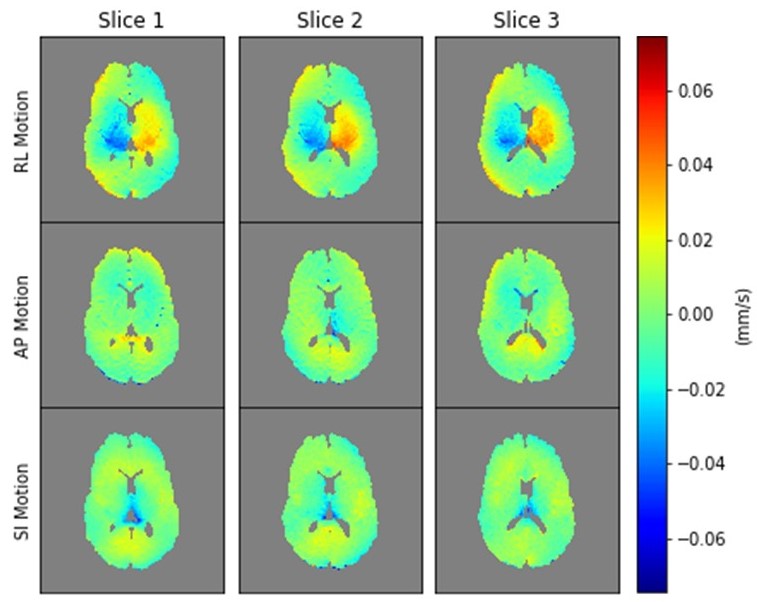
Some q-space redundancy is required for SCIMI reconstruction: it both recovers SNR (needed with a low VENC/long TE) and compensates for the non-uniform q-space distribution created by an arbitrary sub-selection of directions. Figure 2 shows a triggered “still frame” image (30 directions), as well as the same image reconstructed using random subsets of q-space. Careful inspection shows a slight change in SNR, but the overall image remains the same. To confirm that each cardiac bin contained a representative sample of q-space, we compared the volume of thr convex hull of the q-space points with that of one created from a tetrahedron of representative points (Fig 3a, 3b). The cardiac bins avoided “trigger-like” effects (rare but possible if the heartbeat synchronized with TR), and each slice contained a largely uniform distribution of the number of directions in each bin. In Fig 3c, the mixing of bins in the latter half of the cycle shows changes in diastole as the length of the R-R interval varies. Figures 4 & 5 show the resulting velocity profiles. In Fig. 4, the full cardiac cycle is shown for a single slice. The brain shows a pulsatility characteristic of the cardiac cycle, with symmetrical (RL) lateral motion around the ventricles in systole (0-170 ms) that reverses at the start of diastole (420 ms). The delay between the true cardiac cycle and the recorded PG signal is observed as the final frame at 767 ms appears to be the true start of systole. Figure 5 shows the volume at a single timepoint, confirming that the motion is consistent throughout the volume. The motion observed has not yet been clinically interpreted but is thought to consist of both parenchymal tissue movement due to pulsation and cerebrospinal/interstitial fluid flow as it moves through the tissue.Conclusion
Our method of using retrospective cardiac gating with a SCIMI sequence images in-vivo motion in the brain parenchyma on the order of 100 um/s. By utilizing q-space redundancy, we created a sequence of motion covering the full cardiac cycle from a single scan, while simultaneously allowing the full dataset to be used in DTI reconstruction. The motion imaged is believed to be a combination of ISF flow through the region and tissue pulsatility due to the cardiac cycle. This reconstruction method may be useful for investigating the mechanics of glymphatic circulation. Longer scans with more q-space directions may be useful in determining other potential influences on ISF flow in the region beyond the effects of the cardiac cycle, e.g., respiration or brain waves during sleep[3].Acknowledgements
Funding for this research was provided in part by CDMRP W81XWH-16-2-0054.
The views expressed in this abstract are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, Walter Reed National Military Medical Center, the Department of Defense, of the U.S. Government.
References
1. Heukensfeldt Jansen, I., et al. (2020, August 10-13). Simultaneous Imaging of Diffusion and Coherent Motion in Slow-Flow Compartments in the Brain [Conference Presentation]. ISMRM 2020, Virtual Conference. https://www.ismrm.org/20/program_files/PP26.htm
2. Feinstein, Jeffrey A., et al. "Using CArdiac Phase To Order Reconstruction (CAPTOR): A method to improve diastolic images." Journal of Magnetic Resonance Imaging 7.5 (1997): 794-798.
3. Fultz, Nina E., et al. "Coupled electrophysiological, hemodynamic, and cerebrospinal fluid oscillations in human sleep." Science 366.6465 (2019): 628-631.
Figures