2313
Safety Considerations in Neuroimaging of Neonatal and Pediatric Patients Using Portable Low Field MRI
Mark Smith1, Harry Hu2, Ram Krishnamurthy1, John Pitts3, and Mai-Lan Ho1
1Nationwide Children's Hospital, Columbus, OH, United States, 2Hyperfine, Dublin, OH, United States, 3Hyperfine, Cleveland, OH, United States
1Nationwide Children's Hospital, Columbus, OH, United States, 2Hyperfine, Dublin, OH, United States, 3Hyperfine, Cleveland, OH, United States
Synopsis
In 2020, a portable 64mT ultra-low field MRI system designed for point of care bedside use received 510K clearance (Hyperfine, Guilford, CT). Our pediatric institution (Nationwide Children’s Hospital) has acquired one of these systems to meet neuroimaging needs for critically ill NICU or PICU patients who cannot tolerate transport to the MRI department. Prior to scanning patients, safety testing for displacement and heating was conducted on monitoring hardware that will be connected to the patient during the bedside MRI. The monitoring hardware was found safe to stay connected to the patient during the bedside MRI.
Purpose
Over the last several decades, Magnetic Resonance Imaging (MRI) has emerged as a powerful imaging modality. The applications of MRI continue to expand rapidly, but the cost, infrastructure and safety requirements of MRI prohibits its utility in certain patient populations due to logistics, critical illness, contraindicated implanted devices and monitoring equipment. Recently, a portable 64mT ultra-low field MRI system received 510K clearance (Hyperfine, Guilford, CT). This is a point of care (POC) system designed for bedside use (Figure 1), affording neuroimaging to patients in circumstances where conventional MRI is not possible. Our pediatric institution (Nationwide Children’s Hospital) recently acquired one of these systems, with the intent to meet neuroimaging needs for critically ill NICU or PICU patients who cannot tolerate transport to the MRI department. Most of these patients are on continuous monitoring and / or life support, requiring that electronic equipment and associated hardware remain operational and connected to the patient during the bedside MRI exam. Prior to scanning patients with the portable MRI, safety testing should be conducted on monitoring hardware likely to be in place during the bedside MRI, especially hardware that is MR unsafe for conventional high-field MRI. FDA 510K clearance of the Hyperfine system did not include compatibility of any of the tested equipment in this abstract.Methods
Patient monitoring hardware commonly used in our NICU and PICU was identified. This included five types of electrodes (Kendall 1041PTS and 1042PTS neonatal electrodes, Kendall L36-L6 cloth limb band electrodes, Kendall neonatal-pediatric monitoring electrodes with aloe, and 3M Red Dot neonatal ECG monitoring electrodes), a Nellcor neonatal-adult SpO2 sensor and a MEAS 4400 series esophageal temperature probe. Each of these underwent safety tests for displacement and heating within the portable MRI scanner. Wick traditional hemoclips, an Abbott ECMO CentriMag pump (Figure 2) and six ECMO catheters (Medtronic Biomedicus 17 Fr. 50 cm. femoral-venous, 17 Fr. 18 cm arterial, 14 Fr. 12 cm arterial, 14 Fr. 12 cm venous, DLP 14 Fr. “bullet tip”, and Getinge Avalon 16 Fr. bi-caval dual lumen) were also subject to the same tests. Displacement testing simply consisted of placing each hardware item on the scanner magnet plate and observing attractive forces. Testing for heating consisted of placing each item in a tissue mimicking agar gel tub within the scanner, and taking photos and thermal images using a hand held thermal camera (Ideal Industries, Model # 61-844) to record temperature changes before and after 30 minutes of continuous scanning (Figure 3). The 30 min scan consisted of typical spin echo pulse sequences (T1, T2, T2 FLAIR, DWI). Additional thermal images were taken with the ECMO catheters lying on the bare neck of a volunteer before and after a 40 min scan conducted under IRB approval (Figure 4). All testing was done and data evaluated by a MRSO / MR physicist.Results
All five types of electrodes, the SpO2 sensor, temperature probe and hemoclips were non-ferrous and were not subject to translational forces nor displacement, and pre / post scan temperature changes were ≤ 2o C. The ECMO CentriMag pump housed a magnet in the impeller wheel, resulting in displacement of the impeller, and translational force exerted on the pump at a 50 cm. distance from the edge of the scanner. Because of this, a heating test was not performed on the pump. All six ECMO catheters exhibited weak displacement within the scanner due to ferrous coiling within catheter tubing. Pre / post scan temperature changes were ≤ 2o C for all six ECMO catheters when placed on the gel tub. There was a pre / post scan 4o C temperature increase in the Medtronic Biomedicus DLP 14 Fr. “bullet tip” catheter when placed on the bare neck of the volunteer, but this may have been due to inconsistency in positioning of the thermal camera. Pre / post scan temperature changes in the rest of the ECMO catheters when placed on the bare neck of the volunteer were ≤ 2o C, and went unnoticed by the volunteer.Conclusion
Our initial tests on this portable ULF MRI scanner revealed no safety concerns due to displacement or heating, apart from the ECMO CentriMag pump. In a patient setting, positioning the CentriMag pump and the integrated ECMO system apparatus at least one meter in distance from the scanner edge is recommended. All the hardware tested above is MR unsafe or conditional at 1.5T and 3T. Other equipment that we have not tested but we consider potentially unsafe include Camino ICP monitors, LVAD, cardiac pacing wires and the Pleuraflow Chest tube with magnetic strip..Acknowledgements
No acknowledgement found.References
1. Sheth KN, et al. Assessment of Brain Injury Using Portable Low Field MRI at the Bedside of Critically Ill Patients. JAMA Neurology 2020; E1-7. doi:10.1001/jamaneurol.2020.3263.Figures

Figure 1

Figure 2
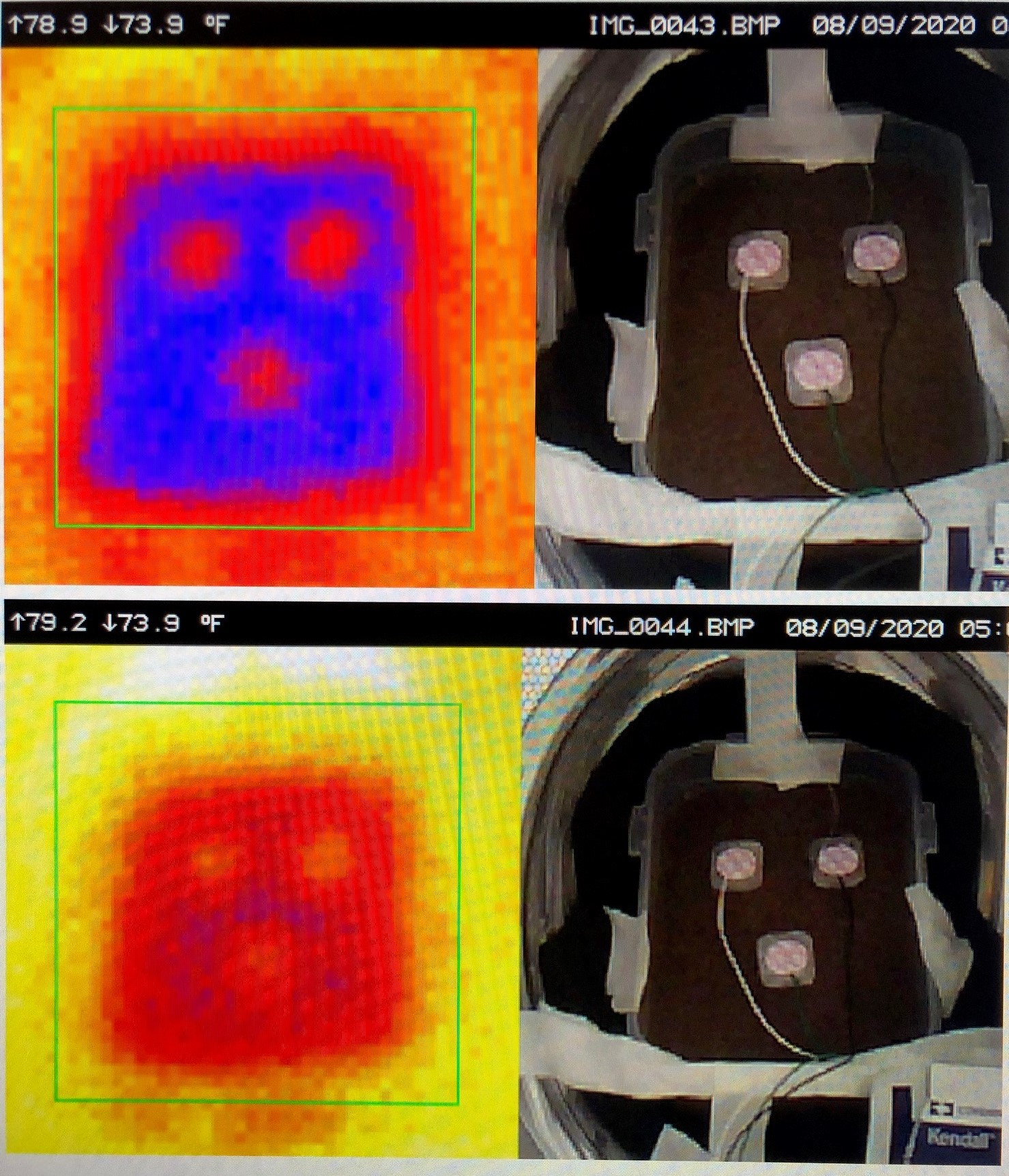
Figure 3
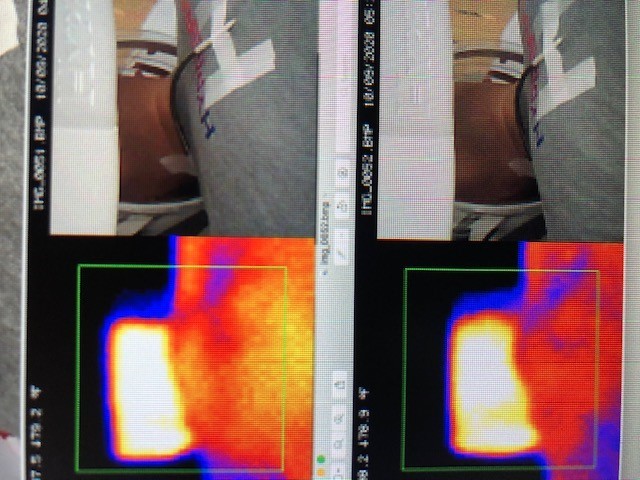
Figure 4