2306
Impact of 1.5T SAR Limits on the MRI Scan Time for Implantable Devices1Axonics Modulation Technologies, Irvine, CA, United States, 2Purdue University, West Lafayette, IN, United States
Synopsis
Implant device manufacturers often specify a RF exposure limit based on specific absorption rate (SAR) or B1+rms and a continuous active scan time in the device magnetic resonance imaging (MRI) labelling. Due to the restriction of the labeled SAR, MR sequence parameters may need to be adjusted to reduce RF power, resulting in prolonged scan time. The patient examination duration may be extended by up to 67% when compared to standard protocols. The overall session may be further prolonged due to additional wait time requirements from certain implanted devices, which can result in great inconvenience and extra cost to patients.
Purpose
To ensure the safety of MRI scans for patients with medical implants, device manufacturers often specify a Radio Frequency (RF) electromagnetic exposure limit based on SAR or B1+rms and a maximum continuous active scan time. Exam duration from multiple imaging centers for patients without medical implants has been studied1; however, these scans were performed under Normal Operating Mode (NOM) without further RF power limitation. For patients with implants, scan sequence parameters may need to be adjusted to reduce RF power. As a result, the scan time may be prolonged. This study aims to investigate the effect of SAR limit on scan time, and the impact on overall MRI exam duration.Methods
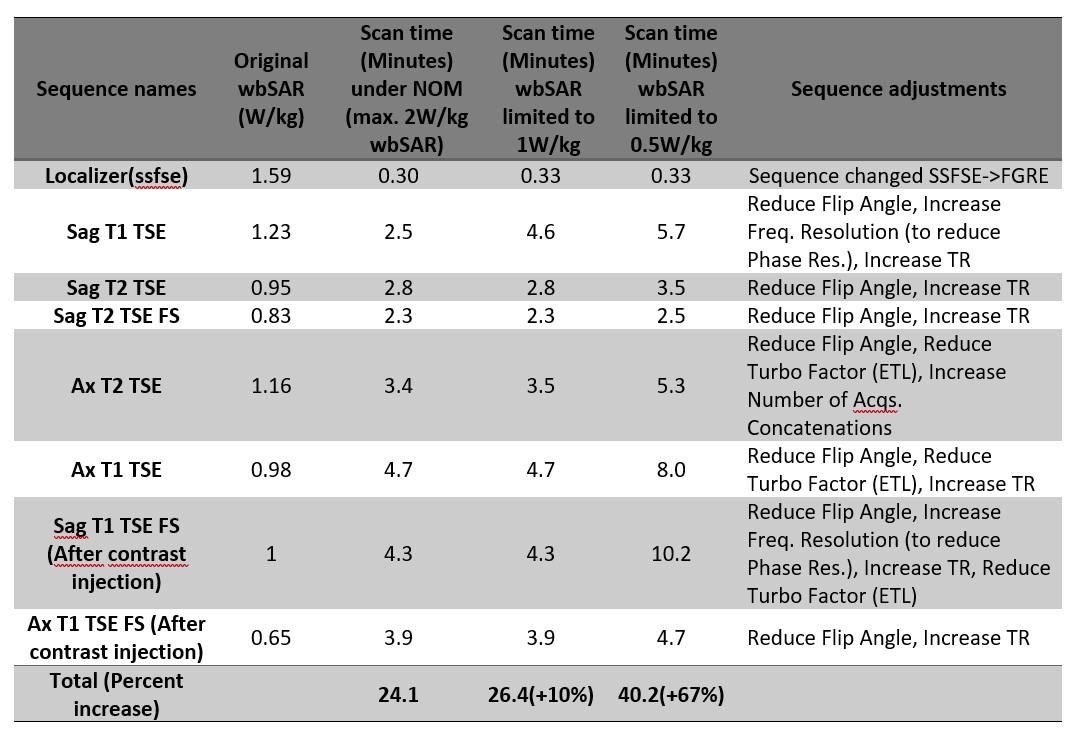
In this study, exam duration refers to the elapsed time from the start of image acquisition to the end of the scan, and scan time refers to the active scan time when the standard sequences for a specific region are executed. For Head/Brain, Lumbar Spine, Prostate and Breast scans, exam duration is representative of the scan time with minimal deviation, as pauses (or interscan time) between sequences are negligible1. NOM in this study refers to scans performed with whole body SAR (wbSAR) limited to 2W/kg and head SAR limited to 3.2W/kg.1.5T MRI exam duration data was reported and default scan time was collected on standard protocols for various scan regions1. These standard protocols are designed for routine clinical scanning using whole body RF transmit coils in NOM. For patients with medical implants, RF energy may need to be reduced such that the resulting SAR levels do not exceed safety limits specified by the implant manufacturer. To reduce RF energy, sequences from standard protocols were adjusted by an experienced technologist using approaches including: a)Reducing the flip angle (while maintaining acceptable image quality); b)Increasing repetition time; c)Decreasing turbo factor; d)Applying low SAR mode when applicable and e)Changing Fast Spin Echo based sequences to Gradient Echo based sequences. Table 1 shows an example of Lumbar Spine scan adjustments. The prolonged scan time was recorded from the restricted RF powers (1W/kg and 0.5W/kg in this study) and the percent increase was computed.
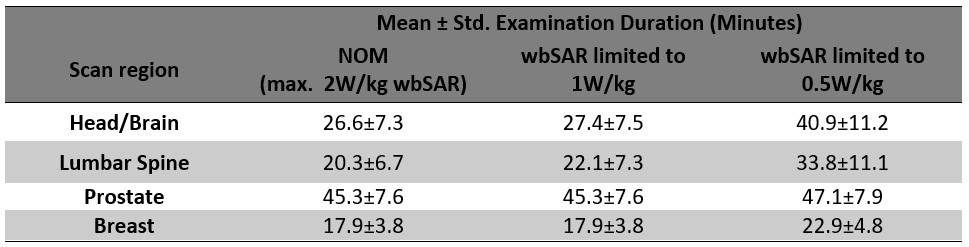
Exam duration was analyzed for a total of 341 patients under NOM from a single imaging site. Projected exam duration for the restricted wbSAR levels (1W/kg and 0.5W/kg) was computed based on the percent increase factor relative to the baseline exam duration. The prolonged MRI exam duration was further analyzed for statistics and distribution.
Results
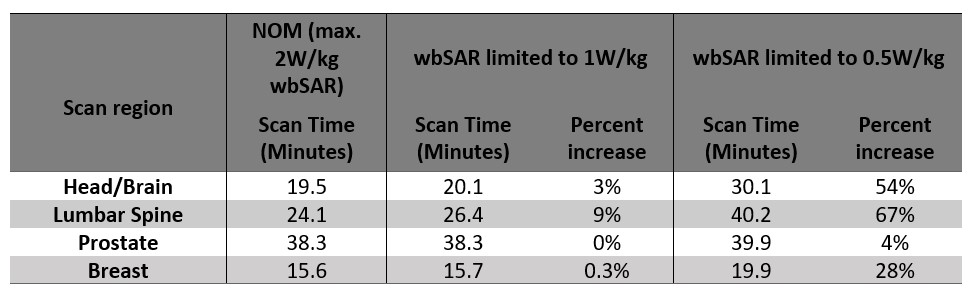
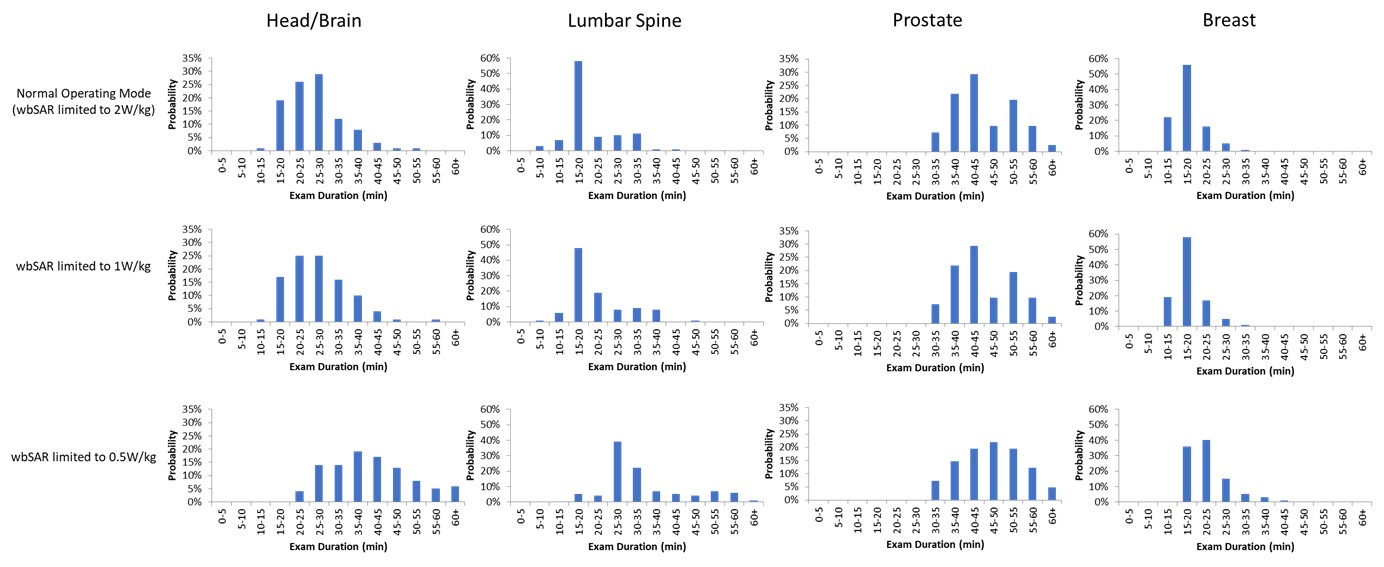
Table 2 shows the scan time based on standard protocols under NOM and the prolonged scan time for the same regions when wbSAR is limited to 1W/kg and 0.5W/kg. The percent increase is also computed for each scan region.Table 3 shows the projected MRI exam duration statistics. The distributions at different wbSAR limitations are shown in Figure 1.
Discussion
This study presents the increase in scan time for MRI procedures due to restrictive RF exposure requirements imposed by certain medical implants. Based on standard scanning protocols, scan duration may increase by up to 67% when wbSAR is limited to 0.5W/kg compared to the same protocol performed under NOM.Patient exam duration under NOM can vary from standard protocols because the protocols are adjusted for each patient’s individual needs. There are several other reasons contributing to the variations in the patients’ exam duration, including 1) Repeating sequences due to motion; 2) Region of interest requiring different scanning coverage; 3) Addition of sequences per Radiologist’s request; 4) Pauses during scanning for patient comfort; 5) Patient refusal and 6) Sequence modifications for safety reasons.
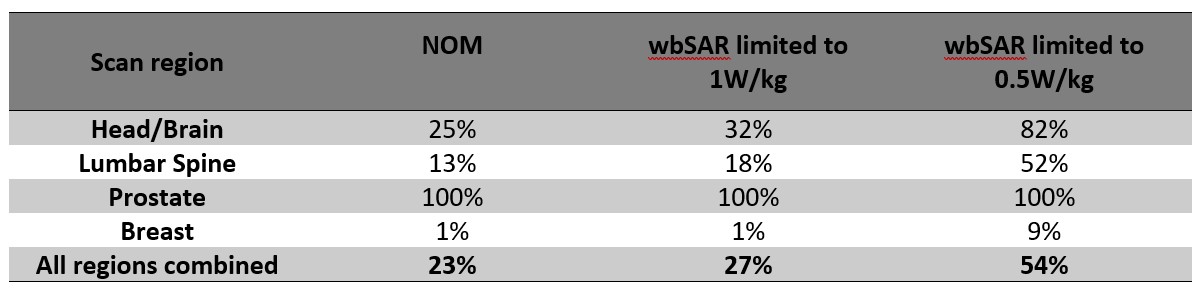
Table 4 summarizes the percentage of scans that are expected to exceed 30 minutes under various RF exposures. Many implant manufacturers specify a wait time after a maximum continuous active scan time is reached2, or an active scan time limit in a scanning window3. This could further extend the patients’ imaging session. For example, for Lumbar Spine scans, it is estimated that 13% of patient scans exceed 30 min under NOM. But if the implant requires RF level to be lower than 0.5W/kg, 52% of the scans are now expected to last more than 30 min. If the device requires another 60 min of wait time after 30 min of active scanning, then the scan session would last at least 1.5 hours, posing challenges in scanner/schedule availability and/or increased cost for patients.
The sequence adjustments made in this study intend to maintain a similar level of image quality to the original protocols. Therefore, an extended scan time was expected when the RF level was reduced. Alternatively, MRI operators may also choose to prioritize scan time at the cost of image quality, e.g. by reducing the flip angle4. The effect of reduced image quality on final diagnosis is outside the scope of this study and is worth exploring in the future.
Conclusion
We presented the increased scan time for standard protocols and extended MRI exam duration when the RF exposure is limited due to the presence of an implant device. With further potential wait time requirements, the overall session may be much further prolonged, resulting in difficulty or great inconvenience and added cost to patients with implant devices.Acknowledgements
No acknowledgement found.References
1. Y Wan et al, Analysis on 1.5T MR clinical scan time of patients from multiple imaging centers, ISMRM 2021
2. MRI Guidelines, Axonics Sacral Neuromodulation System, 110-0092-001rM. https://www.axonics.com/hcp/resources/resource-library
3. MRI Guidelines for InterStim systems 97810 3058 3023, 2020-07-15. http://manuals.medtronic.com/content/dam/emanuals/neuro/M980291A_a_015_view_color.pdf
4. S Kim et al, Effect of Flip Angle for Optimization of Image Quality of Gadoxetate Disodium–Enhanced Biliary Imaging at 1.5 T, American Journal of Roentgenology 2013 200:1, 90-96
Figures