2300
Assessing the In-Vivo RF Heating Effects of Short-Duration B1+RMS in MRI Sequences
Negin Behzadian1 and Shiloh Sison2
1Research and Development, Abbott, Sylmar, CA, United States, 2Research and Development, Abbott, Sunnyvale, CA, United States
1Research and Development, Abbott, Sylmar, CA, United States, 2Research and Development, Abbott, Sunnyvale, CA, United States
Synopsis
Exposure to the RF energy of an MRI shall be limited to prevent potential harm to biological tissues. Whole-body SAR, averaged over any 6-minute interval, shall be limited to 2W/kg and 4W/kg under the limits of Normal and First Level Controlled Operating Mode, respectively, and is further restricted to twice the operating mode limit over any 10-second period. Our study investigates whether similar short-duration assessments are necessary for the alternative RF exposure metric of B1+RMS, in the context of RF heating safety of cardiac protocols with leaded cardiac implants.
Introduction
Exposure to the RF energy of an MRI scanner may cause an increase in the systemic and local temperature of biological tissues and shall be limited to prevent potential harm. Standards such as the IEC 60601-2-33 conservatively use a 6-minute averaging period to estimate Specific Absorption Rate (SAR), thereby limiting whole-body SAR to 2W/kg under Normal Operating Mode (NOM), and 4W/kg under First Level Controlled Mode (FLCM) over any 6-minute exposure interval. A twofold excess in whole-body SAR is permissible, for exposures of short duration (i.e. 10s) given the 6 min average is maintained. B1+RMS is an alternative RF exposure metric to SAR and is displayed on modern MRI scanners for each sequence, averaged over the worst 10s period. Little has been published however, on the need for similar short-duration limits for B1+RMS. Our study aims to investigate the effect of short-duration exposure to high B1+RMS levels in the context of a 3T cardiac protocol, to determine if there is an impact, and therefore whether a limit is necessary.Methods
We leveraged Penne’s bioheat model to calculate the temperature and thermal dose at each time step:$$$ ρtissueCtissue δT/δt = Ktissue∇2T + Q - ρbloodCbloodWblood (T - Tblood) $$$
For the local hotspot, a (2cm)3 muscle tissue (10g) was examined with blood and muscle diffusion parameters obtained from Wang et al1 and perfusion parameters obtained from Jeynes et al2. Relevant sequence parameters were extracted from a 3T cardiac MRI session of a 47-year old female consisting primarily of RF shimming and pre-scan prep sequences in addition to gradient recalled echo, spoiled gradient echo, turbo spin echo, and echoplanar imaging sequences. For sub-10s sequences, a short-duration B1+RMS was conservatively estimated as the nominal 10s averaged value multiplied by the ratio of 10s to the sequence duration.
Local E-fields scaled to the per-sequence B1+RMS levels, both the 10s averaged and the short-duration estimate, were simulated along cardiac leaded pathways inside a V3 distribution of human body models in Sim4Life, and used to derive a non-perfused temperature rise and ultimately, a volume rate of heat deposition, Q, as a quadratic function of B1+RMS. We used the perfused model to calculate the temperature time course and thermal dose in terms of CEM43°C for both the 10s-averaged and short-duration estimated B1+RMS levels for the entire 3T scan protocol using a time step of 0.1s.
Results
The temperature at the end of the 3T cardiac scan protocol is identical at 42.8°C for both the long-duration and short-duration B1+RMS inputs (Figure 1). However, the cumulative CEM43°C for the protocol is approximately 10 CEM43°C longer at 14.09 CEM43°C when accounting for short-duration B1+RMS exposures (Figure 2).Discussion
This study confirms that accounting for the effects of short-duration B1+RMS, as is common in pre-scan prep, RF shimming adjustment, and Echoplanar imaging sequences, does not affect the temperature rise at the end of the scan. Furthermore, the cumulative thermal dose in terms of CEM43°C, is ~10 CEM43°C higher when short-duration B1+RMS exposure is considered; this difference is less than 10% of the most restrictive CEM43°C acceptance criterion across all tissues that need to be evaluated in AAMI PC76, namely 112 CEM43°C3.Conclusion
Accounting for the effects of short-duration B1+RMS does not result in a significant difference in final temperature or cumulative thermal dose. Accordingly, the short duration B1+RMS case need not be independently assessed for RF heating safety in the context of a cardiac protocol with a leaded cardiac implant.Acknowledgements
No acknowledgement found.References
- Wang Z, Lin J, Mao W, et al. SAR and Temperature: Simulations and Comparison to Regulatory Limits for MRI. JMRI. 2007; 26:437-441.
- Jeynes J, Wordingham F, Moran L, et al. Monte Carlo Simulations of Heat Deposition during Photothermal Skin Cancer Therapy Using Nanoparticles. Biomolecules. 2019; 9: 343.
- AAMI PC76 (Draft), “Requirements and Test Protocols for Safety of Patients with Pacemakers and ICDs Exposed to MRI”, to be published.
Figures
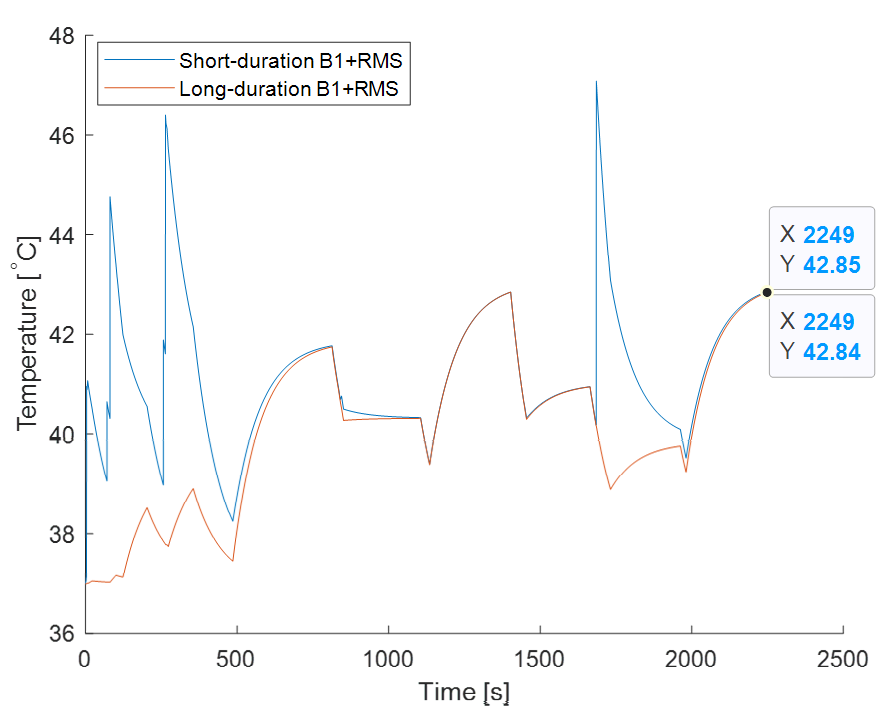
Figure
1: Temperature vs. time for long-duration (i.e. 10s averaged) vs.
short-duration B1+RMS exposure
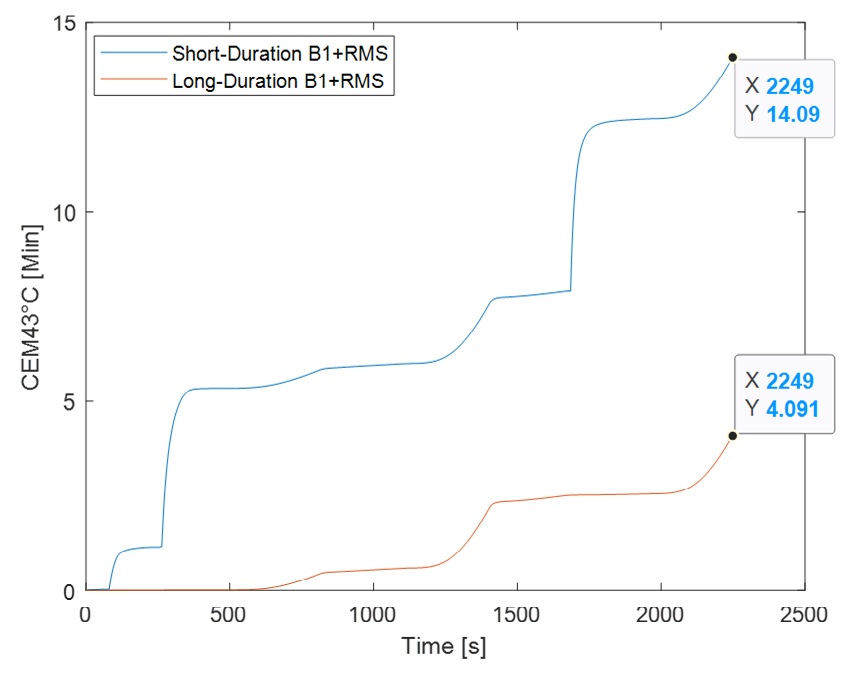
Figure 2: Thermal dose vs. time for long-duration (i.e. 10s averaged)
vs. short-duration B1+RMS exposure