2286
Pediatric Patient Positioning Can Reduce Local-SAR at the Pacemaker Lead-tip During MRI Exams
Jessica A. Martinez1 and Daniel B. Ennis1,2,3
1Department of Radiology, Stanford University, Stanford, CA, United States, 2Cardiovascular Institute, Stanford University, Stanford, CA, United States, 3Maternal & Child Health Research Institute, Stanford University, Stanford, CA, United States
1Department of Radiology, Stanford University, Stanford, CA, United States, 2Cardiovascular Institute, Stanford University, Stanford, CA, United States, 3Maternal & Child Health Research Institute, Stanford University, Stanford, CA, United States
Synopsis
Pediatric patients with cardiac implantable electronic devices (CIEDs) are generally contraindicated for MRI exams. Previous work in the adult population suggests that RF heating strongly depends on the patient’s position and orientation within the MRI scanner. The objective of this work was to evaluate in silico several pediatric patient-positions within the MRI scanner as methods to reduce RF-heating.
Introduction
Pediatric patients with cardiac implantable electronic devices (CIEDs) are generally contraindicated for MRI exams. Contraindications may include MR-unsafe devices and the presence of epicardial and/or abandoned leads – each of which raises safety concerns related to RF-induced heating [1]. Nonetheless, if the clinical benefits of an MRI exam outweigh the risk, then it is necessary to ensure that RF-induced heating is mitigated. RF-induced heating is driven by the coupling of the E-field along the CIED’s lead-path. Previous work at 1.5T on the adult population suggests that RF heating depends on the position and orientation of the body within the MRI scanner [2-4]. Thus, when the patient’s position is modified, the incident E-field is also modified. Herein, we sought to analyze several methods to reduce local-SAR at the lead-tip specific to the pediatric population with CIEDs. Compared to the adult population, pediatric patients present a greater number of position options owing to their smaller size. The positions considered in this work include: i) patient orientation (head-first vs feet-first), plus three head-first supine variations: ii) right-left lateral rotation, iii) off-center within the coil (transversal displacement), and iv) a Fowler position. Hence, the objective of this work was to evaluate in silico several pediatric patient-positions within the MRI scanner as methods to reduce RF-heating.Methods
Numerical simulations were performed on a homogeneous (σ=0.47 S/m) six-year-old pediatric human model from the Virtual Family (Thelonious, IT’IS Foundation) with biventricular leads (RA and RV leads, PEC) undergoing a thoracic examination (chest at isocenter). All simulations were performed using a finite element method (FEM) full-wave electromagnetic solver (HFSS, Ansys Inc). The 1-gram local-SAR was used as a reference value for a reference patient position within the coil (supine, left-right centered, head-first). This was compared to four different positional variations (Fig. 1): i) patient orientation (supine and centered for head-first vs. feet-first); ii) right-left lateral rotation (nominally supine and head-first, angled in increments of 30°); iii) transversal displacement (±10cm left-right displacement); and iv) Fowler positions (seated supine, increments of 10°). The model was loaded in a 16-rung high-pass MRI birdcage coil tuned to 1.5T (64MHz) and the input power was adjusted to produce a whole-body SAR of 4W/kg.Results
Local-SAR values with respect to a reference position and patient position variations for the RA and RV lead are summarized in Table 1. Results suggest that local-SAR values will be affected by the patient position. Local-SAR was reduced by switching patient orientation and by laterally rotating the patient (Fig. 2). Compared to the reference position, local-SAR for a feet-first orientation (Fig. 2-B) resulted in a local-SAR decrease of ~87% for both RA and RV leads. Similarly, the different lateral rotation angles (Fig. 2-C) demonstrated lower local-SAR values compared to the reference position. A lateral rotation of 90° resulted in a local-SAR decrease of ~37% for both leads compared to the reference position.Different local-SAR values were observed each transversal displacement (Fig. 3). Compared to the reference position, only the leftward displacement reduced local-SAR for the RA lead, whereas for the RV-lead, local-SAR was reduced for both left and right displacements. The lowest local-SAR was observed for the left displacement where the percentage change was decreased 10% for the RA-lead, and 33% for the RV-lead.The local-SAR magnitude also depends on the Fowler position (Figure 4). Compared to the reference position, local-SAR for the RA-lead was 33% decreased for the 10° fowler position and 25% and 15% increased for the 20° and 30° fowler positions respectively. In contrast, local SAR for the RV lead was reduced for all Fowler positions, and the 30° Fowler position yielded the lowest local-SAR value (30% decrease).Discussion and Conclusion
MRI exams for pediatric patients with CIEDs are routinely denied mostly due to the presence of epicardial and abandoned leads. Herein, we proposed several pediatric patient-positions within the MRI scanner as a method to reduce local-SAR and hence, RF-induced lead-tip heating. Our results suggest that for a thoracic examination, local-SAR is affected by the patient position within the coil. This is due to the fact that when the patient’s position is modified, the incident E-field is also modified. Our results suggest that for MRI exams that can be performed in either a supine head-first or feet-first patient orientation, a supine feet-first orientation can substantially reduce local-SAR. For examinations that can only be performed in a head-first orientation, a leftward transversal displacement, lateral rotation, or limited Fowler positions, may help to mitigate local-SAR. Future work needs to be performed in non-homogeneous models, a range of pediatric models, and for different lead-paths and lead types and CIED complexities.Acknowledgements
No acknowledgement found.References
- Indik JH, Gimbel JR, Abe H, Alkmim-Teixeira R, Birgersdotter-Green U, Clarke GD, Dickfeld TM, Froelich JW, Grant J, Hayes DL, Heidbuchel H. 2017 HRS expert consensus statement on magnetic resonance imaging and radiation exposure in patients with cardiovascular implantable electronic devices. Heart Rhythm. 2017 Jul 1;14(7):e97-153.
- Martinez JA, Serano P, Ennis DB. Patient orientation affects lead-tip heating of cardiac active implantable medical devices during MRI. Radiology: Cardiothoracic Imaging. 2019 Aug 29;1(3):e190006.
- Xia M, Zheng J, Yang R, Song S, Xu J, Liu Q, Kainz W, Long SA, Chen J. Effects of patient orientations, landmark positions, and device positions on the MRI RF‐induced heating for modular external fixation devices. Magnetic Resonance in Medicine. 2020 Sep 24.
- Golestanirad L, Kazemivalipour E, Keil B, Downs S, Kirsch J, Elahi B, Pilitsis J, Wald LL. Reconfigurable MRI coil technology can substantially reduce RF heating of deep brain stimulation implants: First in-vitro study of RF heating reduction in bilateral DBS leads at 1.5 T. PloS one. 2019 Aug 7;14(8):e0220043.
Figures
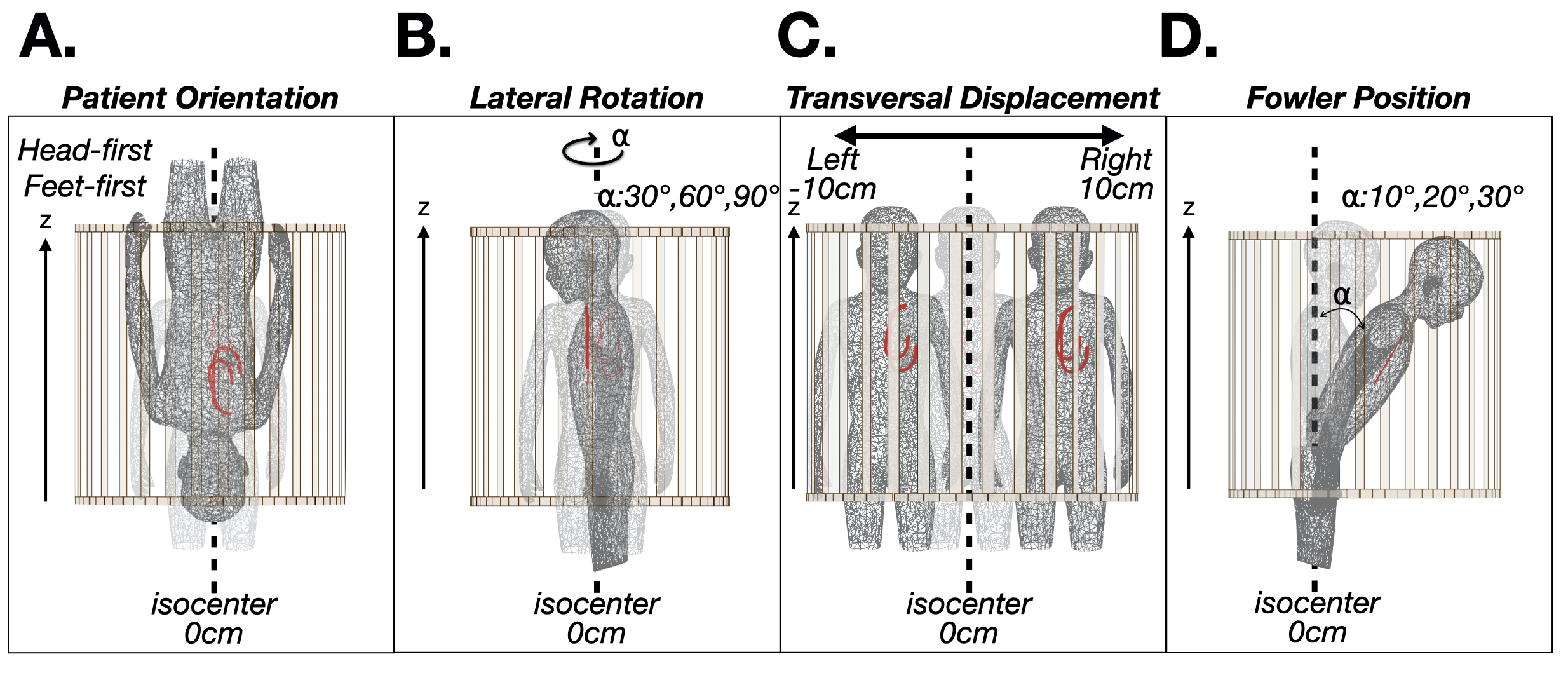
Figure 1. Patient position and orientation variations: (A) head-first vs. feet-first; (B) lateral rotation; (C) transverse left-right displacement; and (D) Fowler position. Each was compared to the local-SAR value with respect to a reference position (shaded, supine and head-first) for a thoracic exam.
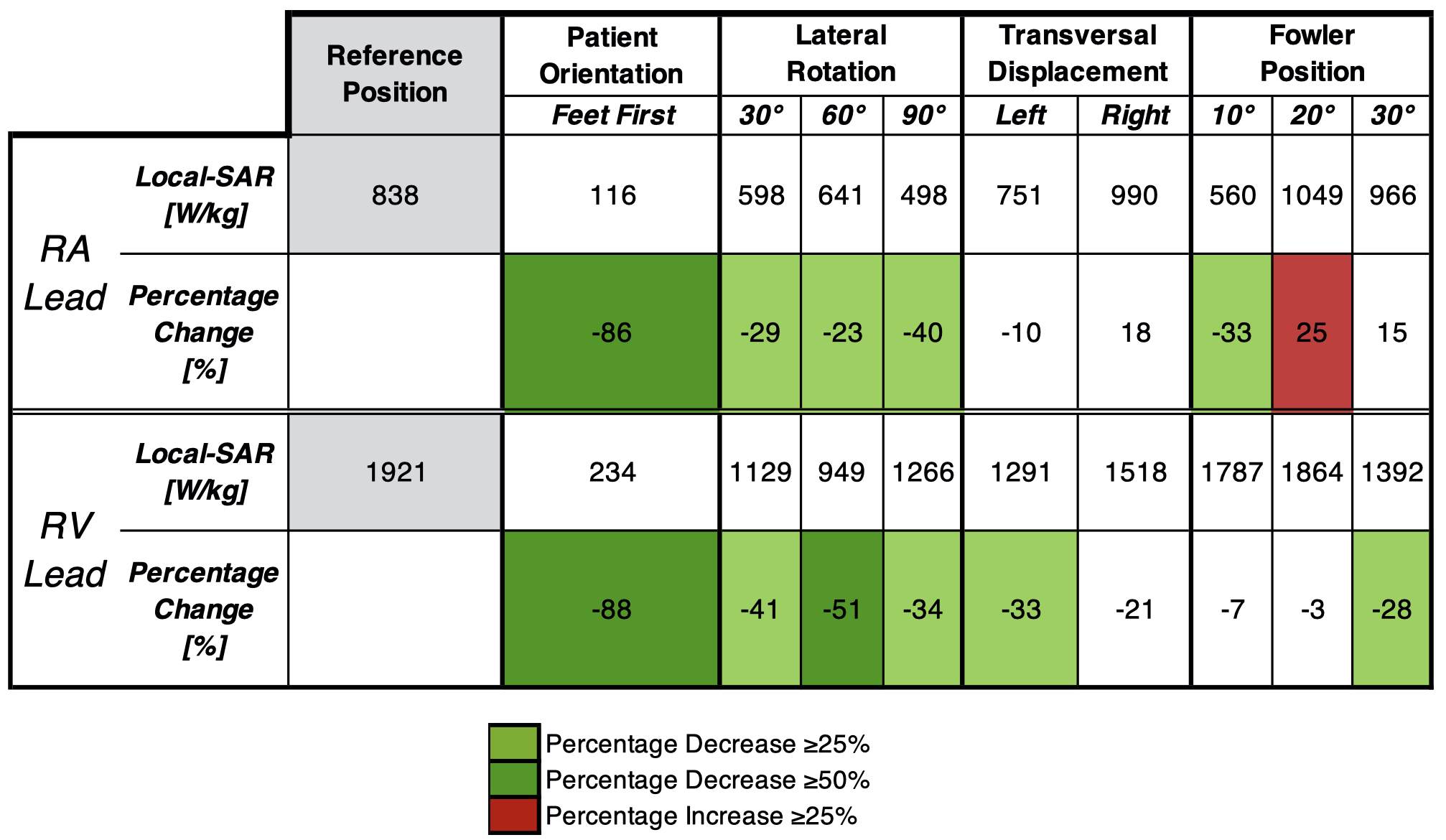
Table 1. Local-SAR (1-gram) values obtained from numerical simulations for different pediatric position variations within the MRI scanner for a 4W/kg thoracic (chest at isocenter) MRI examination. Local-SAR percentage change values ≥25% were considered substantial and are highlighted (green percentage decrease red percentage increase) with respect to a reference position (gray, supine and head-first).
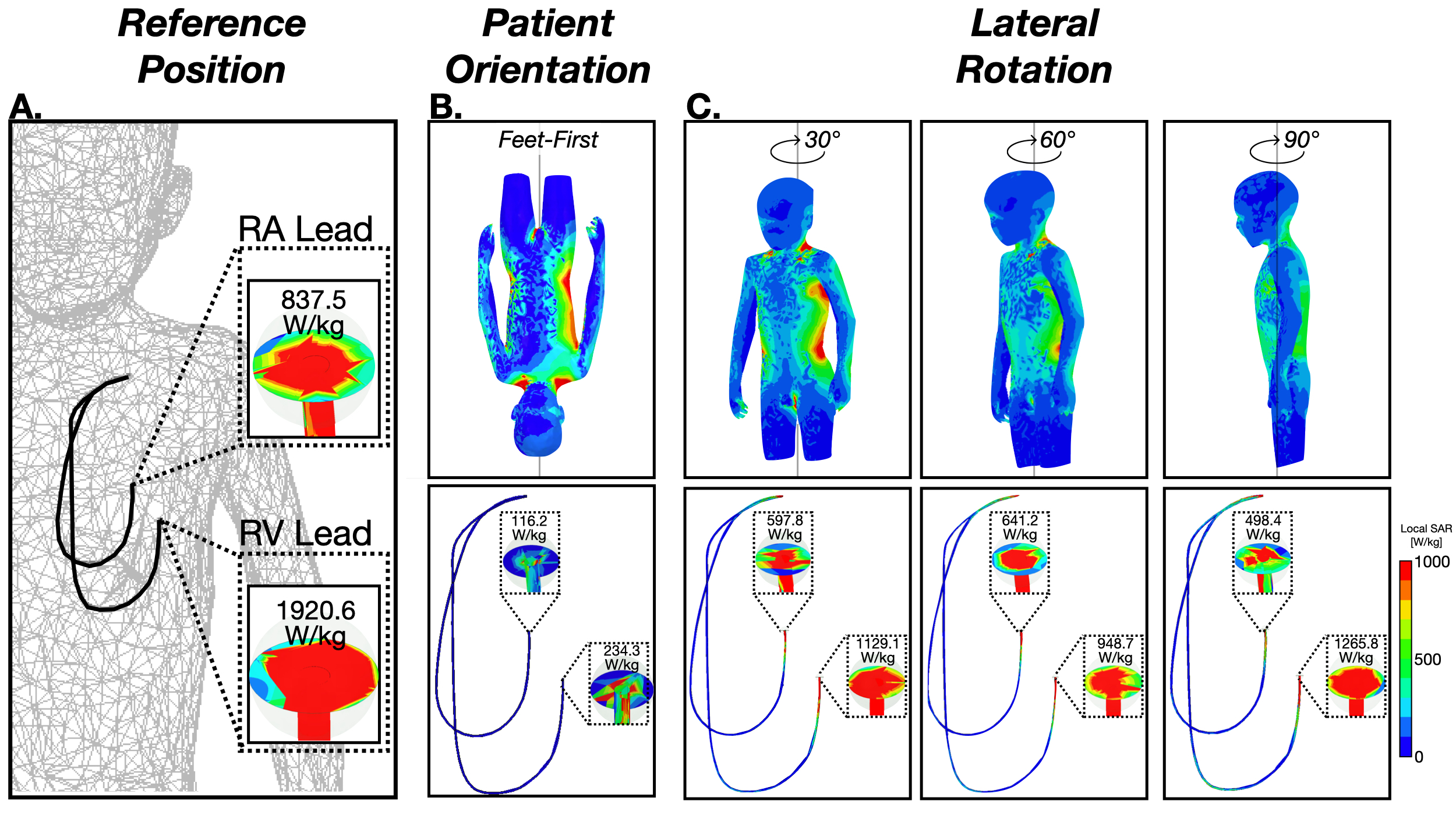
Figure 2. (A) SAR maps and 1-gram local-SAR values for RA and RV leads for the reference position (supine and head-first). (B) SAR maps and 1-gram local-SAR values for a feet-first patient orientation is substantially reduced. (C) Right-left lateral rotations also substantially reduce the 1-gram local-SAR.
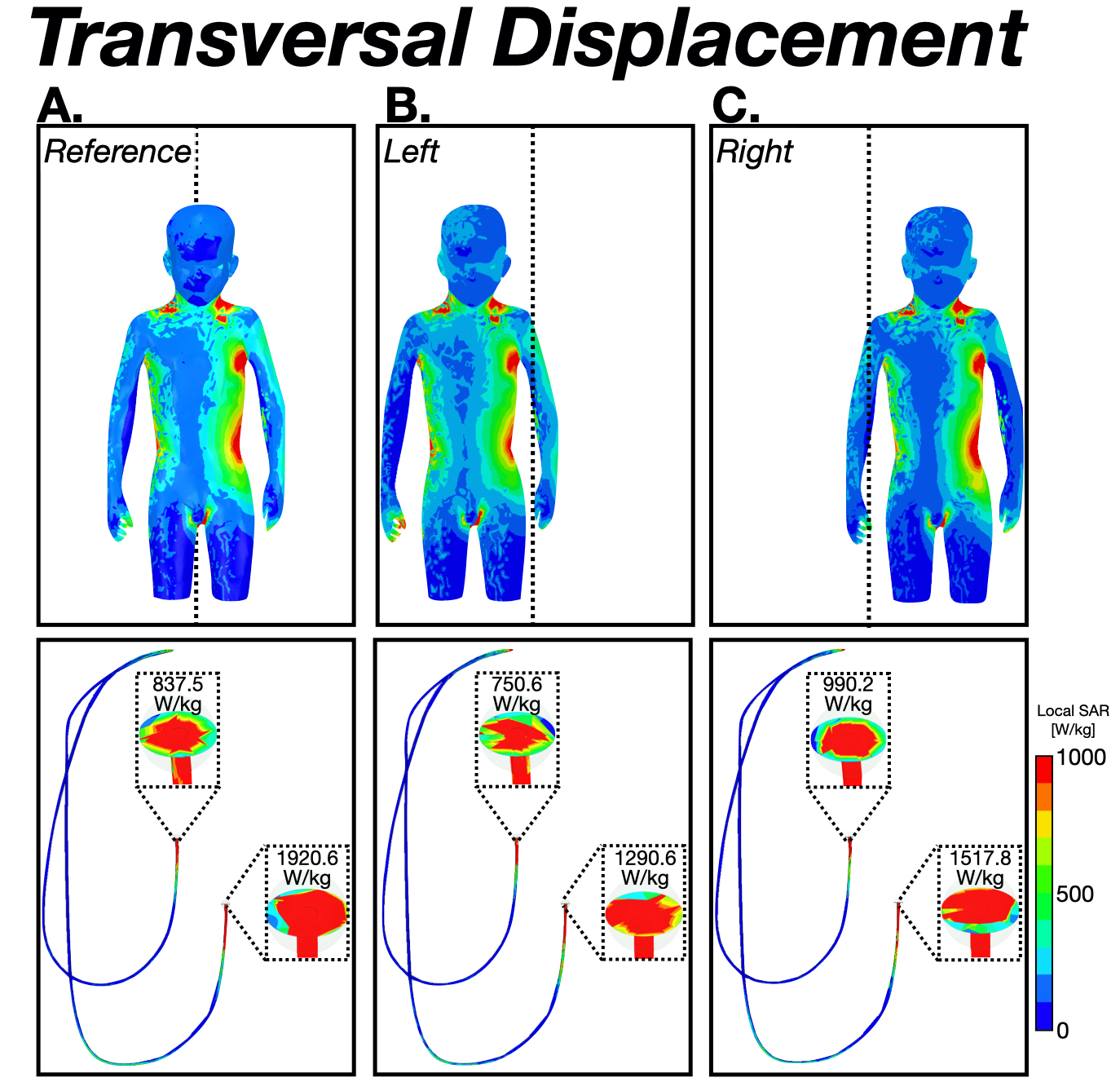
Figure 3. SAR maps and 1-gram local-SAR values for RA and RV leads for (A) the reference position (supine and head-first) and a thoracic exam (chest at isocenter), (B) 10cm leftward displacement, and (C) 10cm rightward displacement. Lower local-SAR values were obtained for a leftward displacement.
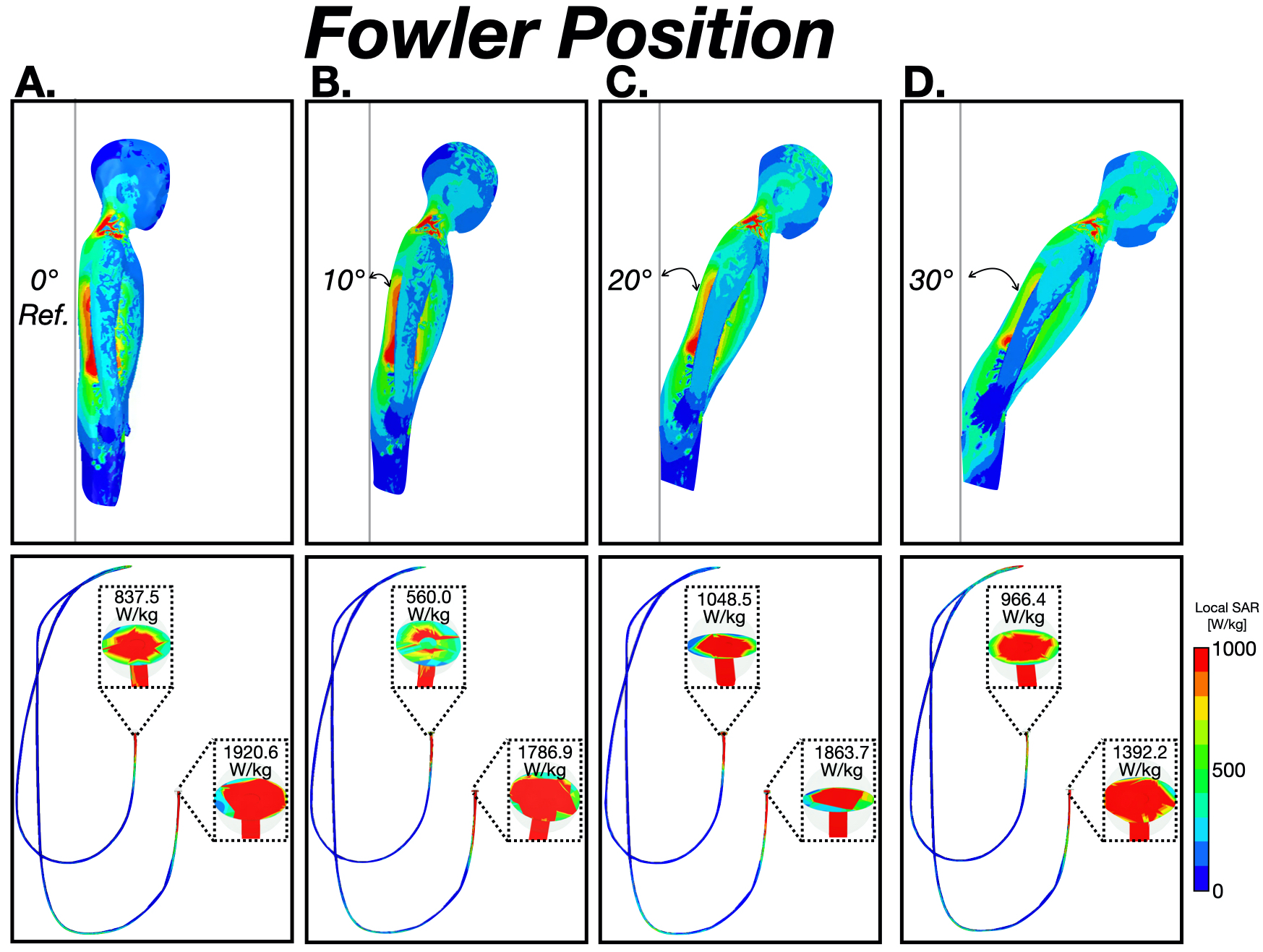
Figure 4. SAR maps and 1-gram local-SAR values for RA and RV leads for the reference thoracic position (supine and head-first). (A) 0°, (B) 10°, (C) 20°, and (D) 30° Fowler positions. Lower 1-gram local-SAR values were obtained at 10° for the RA lead and at 30° for the RV lead.