2275
Estimation of Glomerular Filtration Rate in a Pediatric Population using Renal Phase Contrast MRI
Alex J Barker1, Lorna P Browne1, Michal Schafer2, Erin K Englund2, Takashi Fujiwara2, Kristen J Nadeau2, and Petter Bjornstad2
1Radiology, University of Colorado, Anschutz Medical Campus, Aurora, CO, United States, 2University of Colorado, Anschutz Medical Campus, Aurora, CO, United States
1Radiology, University of Colorado, Anschutz Medical Campus, Aurora, CO, United States, 2University of Colorado, Anschutz Medical Campus, Aurora, CO, United States
Synopsis
Pediatric patients may experience inaccurate estimates of glomerular filtration rate (GFR) by serum creatinine or cystatin C. Renal blood flow (RBF) is a key physiological determinant of GFR, thus, phase-contrast MRI (PC-MRI) is a promising non-invasive technique to investigate relationships to GFR. An interim prospective analysis (n=18) is presented, which investigates RBF as measured by PC-MRI in pediatric bone-marrow transplant candidates who also underwent gold standard measurement of GFR by 125I iothalamate clearance (GFR-iothalamate). The correlation between GFR-iothalamate and RBF by PC-MRI was markedly superior to that of the commonly used endogenous filtration markers serum creatinine or cystatin C.
Introduction
Glomerular filtration rate (GFR) is a key measure of kidney function and is used to determine dosing of renally cleared medications. Methods to directly measure GFR, such as tracking serum or urine clearance of intravenously (IV) administered exogenous filtration markers (e.g. 125I iothalamate), remain the gold standard, however these approaches are expensive, cumbersome and invasive. In practice, estimated GFR (eGFR) is used instead, typically calculated from serum concentrations of endogenous filtration markers, including creatinine and cystatin C. For example, eGFR has previously been recommended to evaluate kidney function for the purpose of gadolinium-based contrast agent use in MRI; however, recent guidelines warn of the potential for inaccuracy.[1] Furthermore, the equations used to estimate GFR have been shown to be inaccurate in pediatric populations with preserved kidney function.[2] Given that pediatric patients are especially prone to inaccurate eGFR ascertainment, non-invasive methods to determine GFR accurately are needed. Since renal blood flow (RBF) is a key physiological determinant of GFR, phase-contrast MRI (PC-MRI) is a promising approach to non-invasively and accurately quantify RBF without the risks of exogenous IV contrast. We therefore present an interim prospective analysis investigating the relationship between RBF as measured by PC-MRI and GFR by 125I iothalamate clearance (GFR-iothalamate) [3] in pediatric bone-marrow transplant (BMT) candidates.Methods
A total of eighteen pediatric BMT candidates were prospectively recruited for a research kidney MRI (Table 1, demographics). Participants 8 to 21 years of age who were scheduled to undergo a BMT and an 125I iothalamate clearance study to quantify GFR were eligible to participate. Before the MRI, fasting urine and blood were collected to measure eGFR markers, i.e., serum creatinine and cystatin C. After completion of 125I iothalamate clearance, same day PC-MRI measurements were completed of the renal circulation. MRI included balanced-SSFP TRiggered ANgiography non-Contrast Enhanced (B-TRANCE) imaging to position ECG-gated breath-held 2D PC-MRI flow measurements (1.2×1.2×6 mm3, with compressed sensing [CS]). PC-MRI was positioned orthogonal to the left and right renal artery at the takeoff of the descending aorta. When venous renal flow was not visible, additional images were acquired of the venous return. In all cases, velocity sensitivity (venc≈100 cm/s) was adjusted to avoid velocity aliasing. Bilateral, time-resolved arterial and venous RBF were measured using ROI’s drawn in Circle CVI42 (Calgary). Right, left, and total arterial and venous net flow, peak flow, and peak velocity were computed. Total bilateral blood flow was computed as the sum of the left and right renal vessels (Table 1). Pearson correlations to eGFR measures and GFR by 125I iothalamate clearance were computed.Results
All participants completed the MRI study. Standard estimates of GFR, i.e., serum creatinine and cystatin C did not correlate with the gold-standard GFR-iothalamate by Pearson correlation (R2=0.019, p=0.94; R2=0.036, p=0.89, respectively). Average peak RBF in both the left and right renal artery (combined) strongly correlated with GFR-iothalamate (R2=0.40, p=0.007). A trend toward significance was observed between total RBF and GFR-iothalamate (R2=0.20, p=0.07). No correlations were found for peak blood flow velocity.Discussion & Conclusion
The gold standard measurement of GFR by radioactive tracers is expensive, arduous, time-consuming, and invasive. Given the known inaccuracy of the commonly used eGFR calculations, especially in pediatric populations with preserved kidney function, improved GFR measurement approaches are crucial to patient care. This is the case for BMT candidates at our institution, who are at high risk of acute and chronic kidney injury. Additionally, decisions regarding the type of transplant and post-transplant immunosuppressive therapies are often based on renal function. Therefore, accurate and precise measurements of GFR is imperative in this patient population. For example, youth scheduled for BMT at our institution currently have their GFR determined by radioisotope disappearance with nuclear medicine (125I iothalamate). The use of radioisotopes outside of select clinical indications is problematic due to logistics, cost, and exposure to radiation, especially in asymptomatic children and/or adolescents. Therefore, a major clinical and research impediment is a practical way to accurately quantify GFR in populations where eGFR is ineffective to ascertain early GFR changes. We leverage a unique opportunity in this patient population to show strong correlations between GFR-iothalamate and RBF biomarkers from a noninvasive, 20-minute PC-MRI study, that are superior to serum creatinine or cystatin C. Additional participants are being recruited to this study for further assessment.Acknowledgements
No acknowledgement found.References
- ACR Committee on Drugs and Contrast Media, Manual on Contrast Media, American College of Radiology, 2020
- Bjornstad P, et al. Update on Estimation of Kidney Function in Diabetic Kidney Disease. Curr Diab Rep. 2015;15(9):57.
- Agarwal R, et al. Assessment of iothalamate plasma clearance: duration of study affects quality of GFR. Clin J Am Soc Nephrol. 2009;4(1):77-85.
Figures
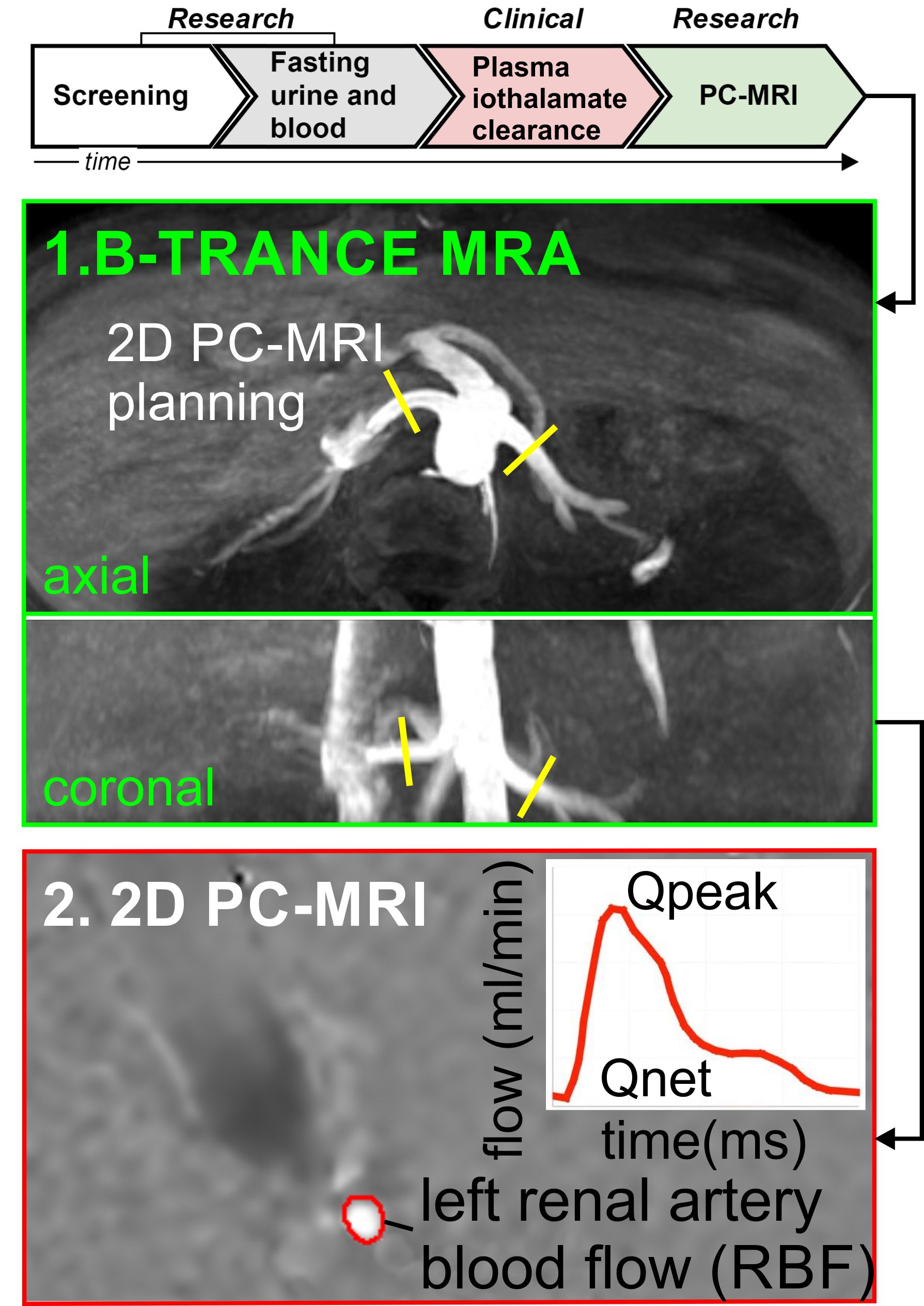
Figure 1:
Study protocol, MRI planning, and quantitative flow measurements obtained with
PC-MRI (note: renal veins not shown).
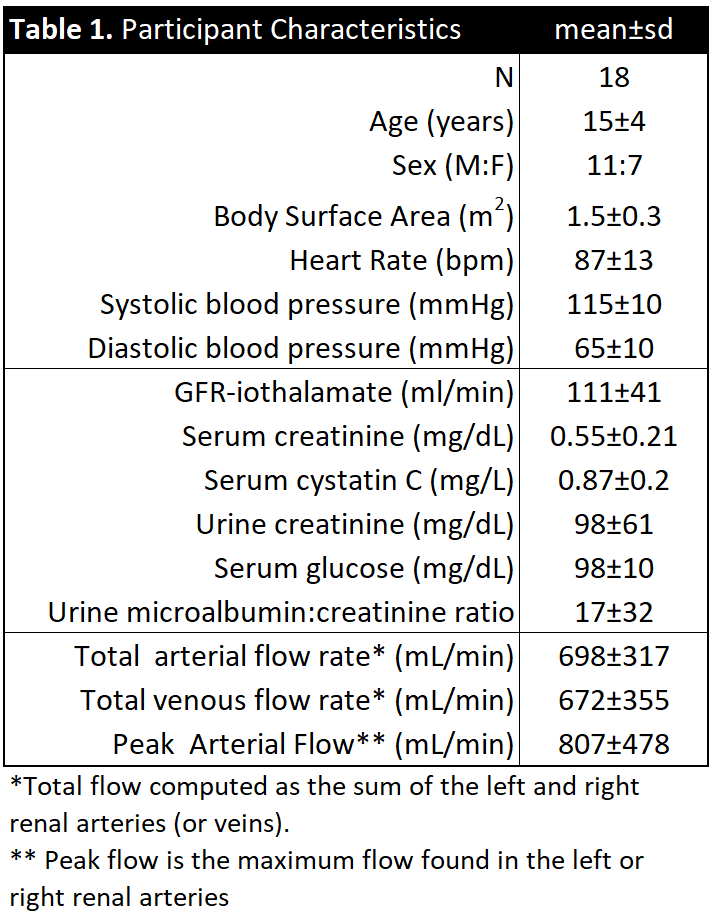
Table 1. Patient Characteristics
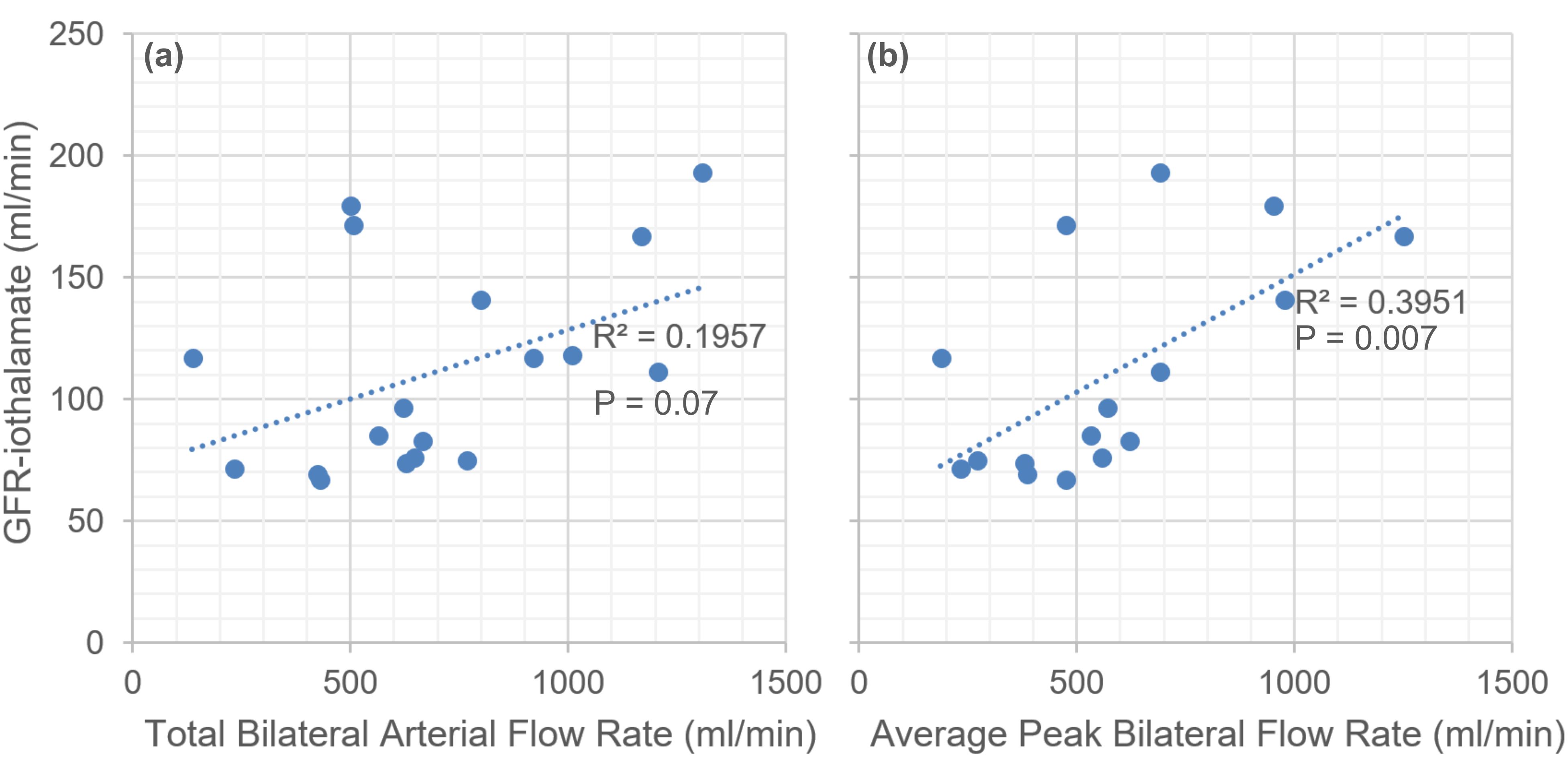
Figure 2: Scatter plots of: (a) total left and right arterial renal blood flow, and (b) the average left and right peak renal blood flow.