2270
DWI and 3D SWAN improve the knowledge of pathophysiological mechanism of neonatal bilirubin encephalopathy1The First Affiliated Hospital of Dalian Medical University, Dalian, China
Synopsis
Exposure to high levels of bilirubin can cause serious severe motor symptoms and cerebral palsy,but the pathophysiological mechanism of brain injury is still unclear.The aim of this study was to explore the possible pathophysiological mechanism of brain tissue injury using diffusion weighted imaging (DWI) and three dimensions T2* weighted angiography( 3D SWAN).
Introduction
Bilirubin encephalopathy (BE) is the most serious complication of hyperbilirubinemia. Currently, the exact pathology of bilirubin brain damage is still poorly understood. The purpose of this study was analyze the possible pathophysiological mechanism of brain tissue injury in children with hyperbilirubinemia (HB) using DWI and 3D-SWAN, and to analyze the relationship between total serum bilirubin (TSB) and the ADC ratio of frontal white matter (FWM) and globus pallid (GP) in full-term neonates with HB.Methods
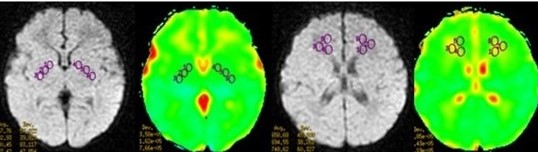
The imaging data of DWI and SWI were analyzed retrospectively and semi-quantitatively in 75 neonates with HB clinically confirmed from October 2014 to March 2019, including 46 males and 29 females, median age of 9 days, mean weight (3.38±0.47) kg. All children were divided into two groups based on their GP T1WI signal intensity: including normal signal intensity group (HBn group): 46 patients, 29 males, 17 females, median age of 9 days, mean weight (3.38±0.47) kg) and high signal intensity group (HBh group): 29 patients, 17 males and 12 females, median age 8 days, mean weight (3.36± 0.46) kg). In addition, forty-four healthy subjects (HC group) who matched the HB group by gender, age and weight were recruited, including 32 males and 12 females, with median age of 8 days and mean weight of (3.40±0.55) kg. On the GE ADW 4.6 workstation, the maximum levels of GP and FWM on DWI and ADC were selected and the ROI was manually selected The ADC values of GP and FWM on both sides were measured three times to obtain the average value (Fig.1 ), and the GP/FWM ratios of ADC were calculated (referred to as rADC). The differences of parameters were assessed using multiple independent samples Krukal- Wallis H test among the three groups. The number of low-signal lesions (cerebral microbleeds, CMBs) of 3D-SWAN was counted, and Fisher's precise test was used to analyze the difference in the incidence of CMBs. Spearman correlation analysis and point-two column correlation analysis were used to analyze the relationship between rADC value, CMBs incidence and serum total bilirubin (TSB) level.Results
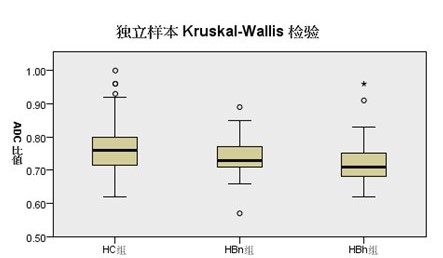
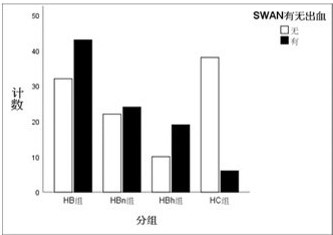
The rADC value of GP in HC group, HBn group and HBh group decreased successively (p<0.05) (Fig.2), while the difference between HC and HBh groups was significant (p<0.05) .Compared with HC group, the number of intrcerebral microbleeds (CMBs) in HB group was significantly increased (p<0.05) (Fig.3). The rADC value of HB group had a positive correlation with TSB (r = 0.202, p=0.013). However, no correlation was found between the number of CMBs in HB group and TSB (p=0.278).Discussion
GP involvement is a well-known MRI finding of BE1, 2, However, it has been controversial whether there is limited diffusion of water molecules in GP of BE, and some scholars believe that no definite abnormal signal was found in GP on DWI sequence 3, 4.Therefore, in this study, the ADC ratio of GP/FWM was used as a reference to quantitatively evaluate the microscopic changes of the diffusion of water molecules in GP. It was found that the limited diffusion of water molecules is present in bilateral GP in children with HB, which enabled us to have a deeper understanding of the pathogenesis of bilirubin encephalopathy, and contribute to accurate clinical evaluation and treatment. In addition, it is a new finding that children with HB are more likely to accompany intracerebral microbleeds than healthy children, but the incidence of CMBs is not significantly related to the level of TSB, indicating that the level of TSB cannot accurately determine the incidence of hemorrhage.To sum up, the limited diffusion of water molecules is present in GP and related to the level of total bilirubin in children with HB. CMBs more likely occur in children with HB and need to attach importance to it during treatment.
Acknowledgements
No acknowledgement found.References
1. Katar S, Akay HO, Taskesen M, et al. Clinical and cranial magnetic resonance imaging (MRI) findings of 21 patients with serious hyperbilirubinemia.J Child Neurol, 2008, 23 (4) :415-417.
2. Wu WL, Zhang P, Lou MW, et al. The application of DWI and MRI in bilirubin encephalopathy and hyperbilirubinemia of the newborn. JPract Radiol, 2011, 27 (8) :1242-1244.
3. Yi MG, Jiang ZQ, Zhao JS, et al. The value of T1WI signal intensity ratio of globus pallidus to putamen in grading and predicting prognosis of neonatal acute bilirubin encephalopathy. Chin J Radiol, 2017, 51(3): 214-218.
4. Jin JY, Li HY, Clinical value of MRI and functional imaging in newborn bilirubin encephalopathy. Chin J CT MRI, 2019,17(1): 12-14, 24.
Figures