2266
Free-breathing T2-weighted multi-shot TSE BLADE for pediatric abdominal imaging1Radiology, Massachusetts General Hospital, Boston, MA, United States, 2Radiology, Harvard Medical School, Boston, MA, United States, 3MGH Martinos Center for Biomedical Imaging, Boston, MA, United States
Synopsis
Abdominal MRI respiratory triggered acquisitions in pediatric populations often fail due to shallow or irregular breathing patterns, degrading image quality and increasing acquisition time. A free-breathing T2-weighted multi-shot TSE BLADE acquisition could overcome these limitations, but through plane motion of respiration causes substantial signal loss from long T2 (such as biliary ducts). We hypothesized that by modifying the refocusing pulse width of the sequence we could mitigate signal loss. Our results show that a 2x refocusing pulse modified free breathing sequence provides comparable image quality and contrast. Furthermore, it offers a fixed acquisition time independent of respiratory patterns.
Introduction
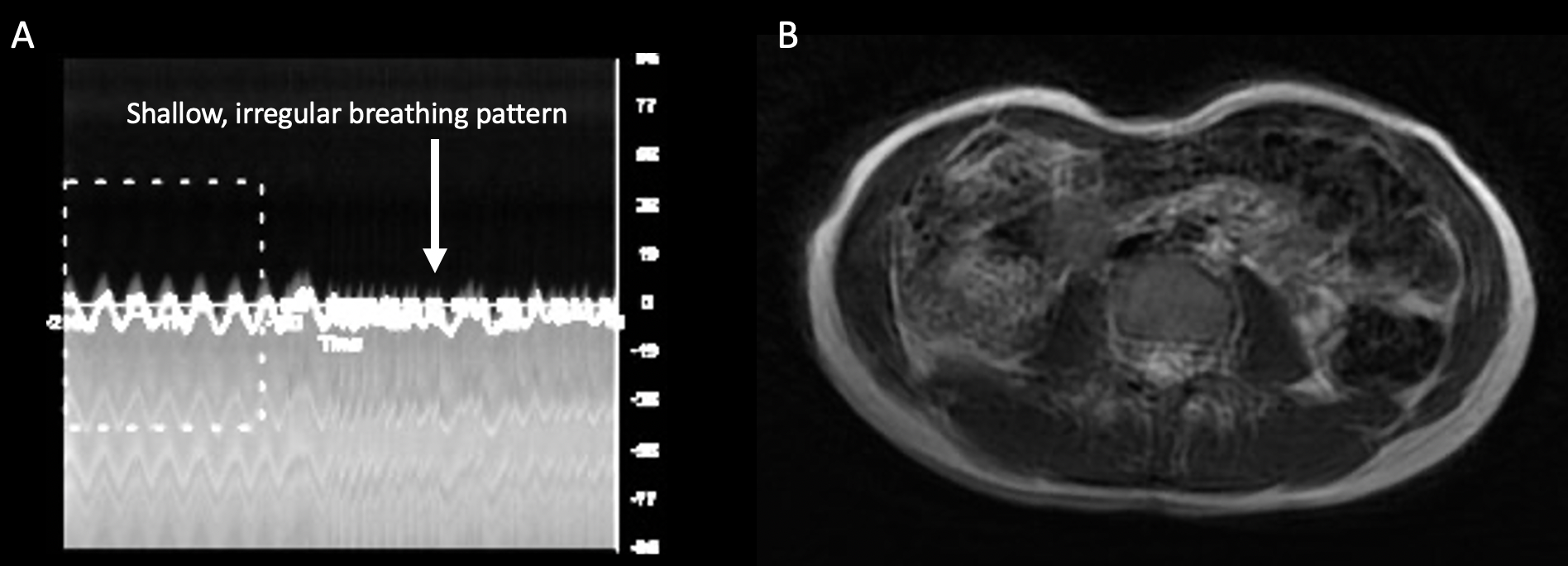
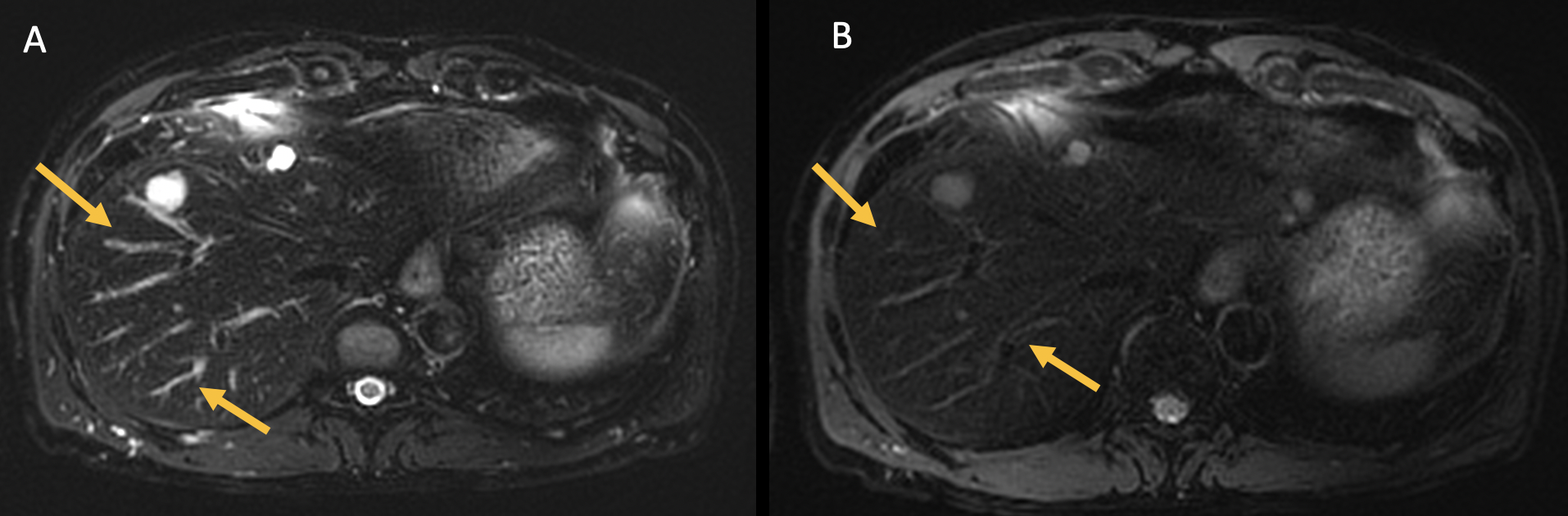
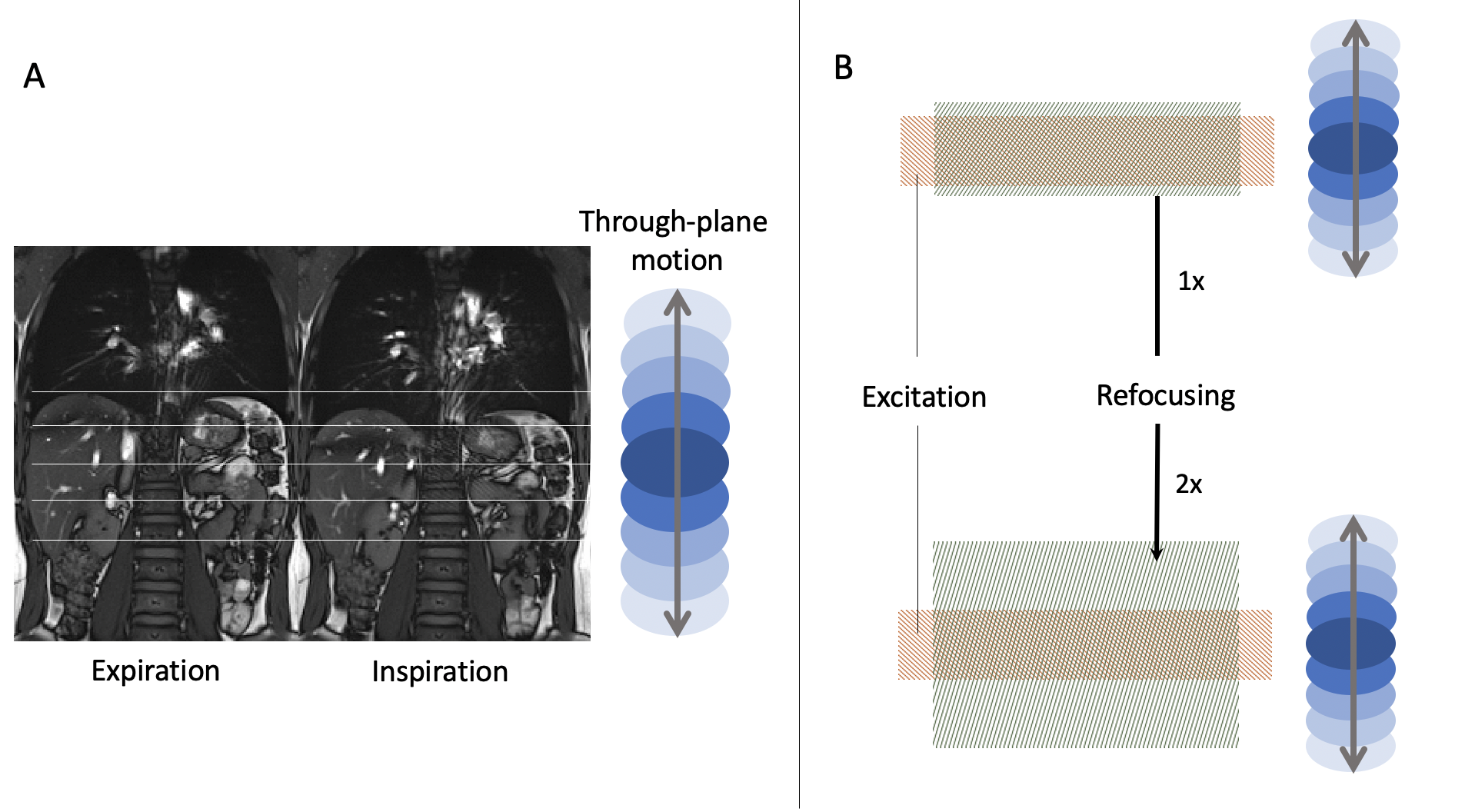
Respiratory motion is a challenge for abdominal MRI acquisitions. The expansion of the thoracic cavity during inspiration displaces the contents of the abdomen, creating through-plane motion for axial acquisitions. Breath-hold acquisitions are unfeasible in infants and small children. Furthermore, respiratory triggered acquisitions (such as diaphragmatic navigators) often fail due to shallow or irregular breathing patterns1 (Figure 1) and have been associated with an increase in acquisition time of up to 6-8 minutes in clinical practice.A free-breathing multi-shot TSE BLADE acquisition could theoretically prevent motion degradation and overcome some of the limitations of respiratory triggered acquisitions2. However, there is substantial signal loss from long T2 structures such as the bile ducts that move through-plane in transverse slices from respiratory motion (Figure 2). This can be attributed to signal loss during the excitation and refocusing process of the turbo spin echo (TSE) technique and is a consequence of refocusing pulse width. Given this clinical problem and the limitations of current sequences, this study aims to explore the feasibility of a modified refocusing pulse free-breathing multi-shot TSE BLADE sequence for pediatric abdominal imaging.
Theory
Excitation of magnetization in a given thickness of tissue will not align with action of refocusing during movement through-plane leading to insufficient spin echo formation and loss of signal. This can be exacerbated by using small slice thicknesses and refocusing pulses that are on the order of the thickness dimensions of the excitation pulse. Since SAR can be problematic at 3T, reduction of the dimension of the refocusing pulse that dominates SAR is sometimes strategically used as well.In order to overcome this sensitivity to motion, we employed a modified TSE technique that uses a user-controlled variable refocusing thickness that can be increased to account for through-plane tissue motion as shown in Figure 3. This was accomplished by reducing the gradient amplitude rather than increasing the transmission bandwidth with no increase in SAR. In our study we used a refocusing thickness equal to twice that of the excitation thickness (2x refocusing pulse). In conventional multi-slice imaging, slice to slice crosstalk interference can be potentially problematic in such cases, but was avoided by using multiple time-sequential slice concatenations which were necessary anyway due to SAR restrictions associated with obtaining sufficient tissue coverage.
Methods
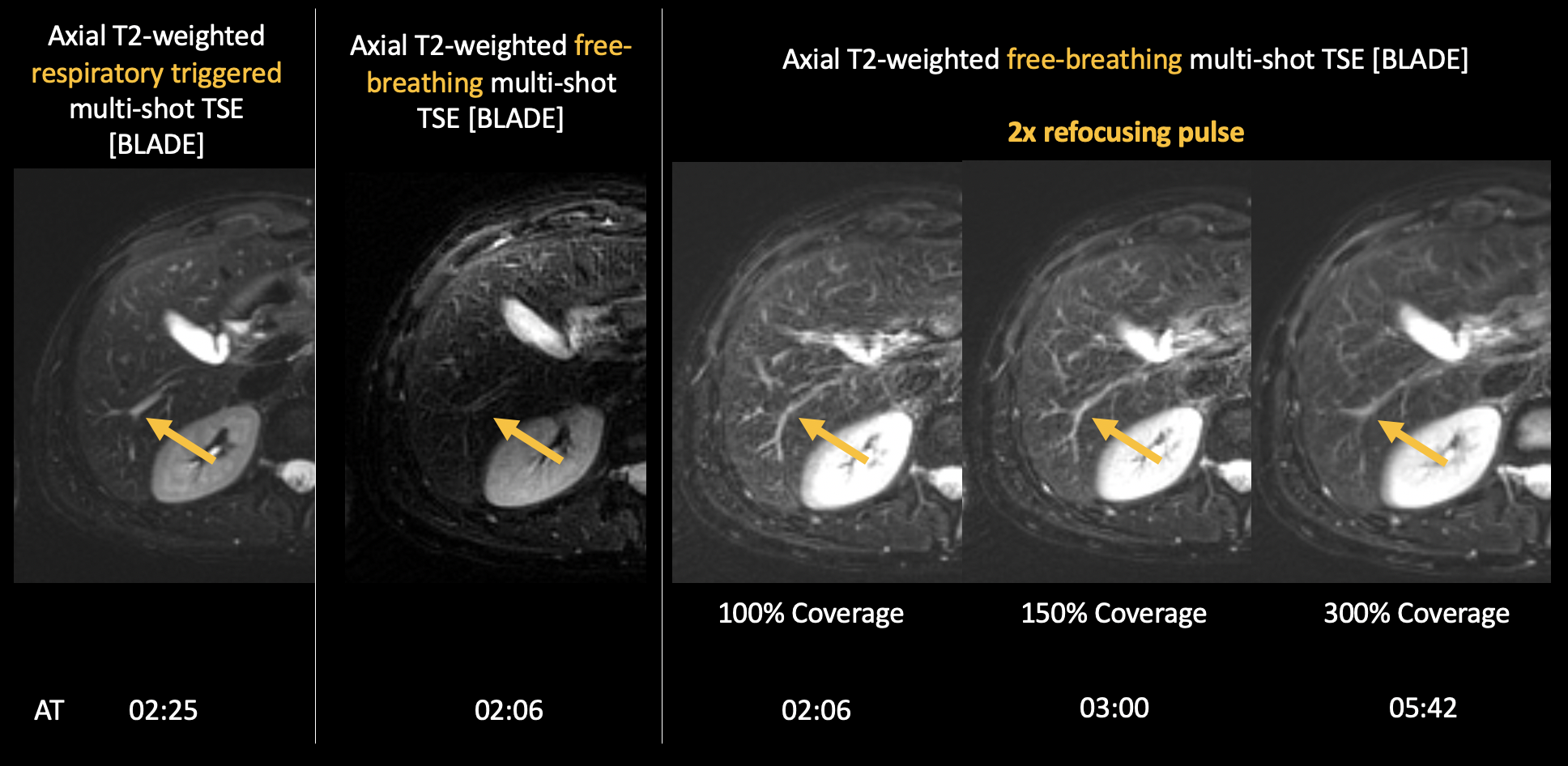
A healthy volunteer underwent imaging at 3 Tesla [Magnetom Skyra, Siemens, Erlangen] and the following sequences were acquired: a) Axial T2-weighted fat-suppressed respiratory triggered multi-shot TSE (BLADE) [FOV= 380mm, matrix= 256 x 76, slices 23, slice thickness 3mm, slice gap 10%, TE= 98ms, TR=2000ms, 02min 25sec], b) Axial T2-weighted fat-suppressed free-breathing multi-shot TSE (BLADE) [FOV= 380mm, matrix= 256 x 76, slices 23, slice thickness 3mm, slice gap 10%, TE= 116ms, TR=2000ms, 02min 06sec], c) Axial T2-weighted fat-suppressed free-breathing multi-shot TSE (BLADE 100% coverage) with modified 2x refocusing pulse [FOV= 380mm, matrix= 256 x 76, slices 23, slice thickness 3mm, slice gap 10%, TE= 116ms, TR=2000ms, 02min 06sec], d) Axial T2-weighted fat-suppressed free-breathing multi-shot TSE (BLADE 150% coverage) with modified 2x refocusing pulse [FOV= 380mm, matrix= 256 x 76, slices 23, slice thickness 3mm, slice gap 10%, TE= 116ms, TR=2000ms, 03min], and e) Axial T2-weighted fat-suppressed free-breathing multi-shot TSE (BLADE 300% coverage) with modified 2x refocusing pulse [FOV= 380mm, matrix= 256 x 76, slices 23, slice thickness 3mm, slice gap 10%, TE= 116ms, TR=2000ms, 05min 42s].Two board certified radiologists rated each acquisition using a Likert scale in a blind assessment. Overall image quality, biliary duct contrast, CSF contrast (1 poor – 5 excellent), and degradation by motion artifacts (1 very degraded – 5 not affected) were scored. Average of scores were added and compared.
Results
Figure 4 shows standard and refocusing pulse modified acquisitions, and compares changes in biliary duct signal. Acquisition time for each sequence is also shown. Figure 5 summarizes scores given by raters to each sequence.Discussion
Respiratory-triggered acquisitions of the abdomen can be a challenge for the shallow and irregular breathing patterns of some pediatric populations, and free-breathing acquisitions may be better suited to address respiratory motion. However, as expected, our results show that respiratory triggered acquisitions are the gold-standard if acquired correctly. Nonetheless, the loss of signal of fluid containing structures (long T2) associated with through-plane motion can be mitigated by modifications to the refocusing pulse. Our results show comparable image quality and contrast in the 2x refocusing pulse modified sequences, improving greatly from the conventional free-breathing technique.As discussed above, acquisition time in triggered sequences depends on respiratory patterns and correct respiratory motion gating3. Although the 150% BLADE coverage 2x refocusing pulse modified sequence is 19.4% longer than a correctly respiratory triggered sequence, the free-breathing sequence offers a fixed acquisition time independent of respiratory patterns.
Lastly, motion artifact degradation scores suggest that increasing the BLADE coverage more than 150% in our modified sequence is not useful. Furthermore, it comes at a cost of lengthening acquisition time which should be avoided in pediatric scans4.
Conclusion
Widening of the refocusing pulse of T2-weighted multi-shot TSE can mitigate signal loss associated with through-plane respiratory motion. This approach enables a free-breathing alternative to respiratory triggered abdominal acquisitions in the pediatric population.Acknowledgements
No acknowledgement found.References
1. Jaimes, C., Kirsch, J. E. & Gee, M. S. Fast, free-breathing and motion-minimized techniques for pediatric body magnetic resonance imaging. Pediatr Radiol 48, 1197–1208 (2018).
2. Serai, S. D. et al. Newly Developed Methods for Reducing Motion Artifacts in Pediatric Abdominal MRI: Tips and Pearls. American Journal of Roentgenology 214, 1042–1053 (2020).
3. Chavhan, G. B., Babyn, P. S. & Vasanawala, S. S. Abdominal MR Imaging in Children: Motion Compensation, Sequence Optimization, and Protocol Organization. RadioGraphics 33, 703–719 (2013).
4. Kozak, B. M., Jaimes, C., Kirsch, J. & Gee, M. S. MRI Techniques to Decrease Imaging Times in Children. RadioGraphics 190112 (2020) doi:10.1148/rg.2020190112.
Figures
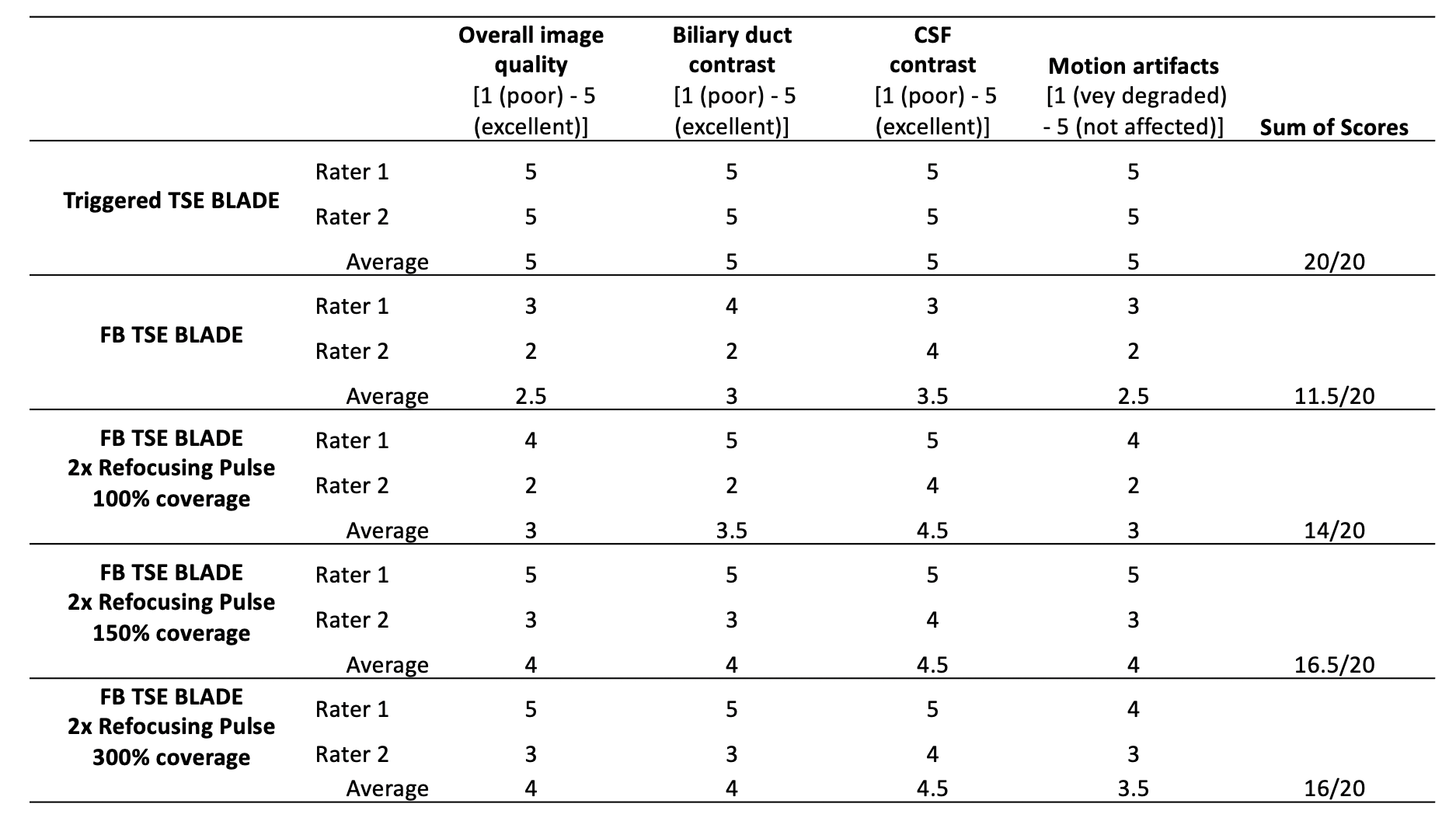
Blind assessment scores of each expert rater and averages for each sequence evaluated.
FB Free breathing