2264
Survey of Acoustic Output in Neonatal Brain Protocols1Food and Drug Administration, Silver Spring, MD, United States
Synopsis
The purpose of this study was to determine the expected sound exposure to the neonate during neonatal brain protocols. To accomplish this, 7 neonatal brain protocols were recorded on 7 different MRI machines across 4 vendors. Neonatal protocol sound levels straddled existing notions of risk, exceeding sound levels known to cause non-auditory stress responses in neonates but not exceeding the IEC MRI hearing safety limit. These results indicate that these sound levels could be risky for the neonate, but that further work is required to clarify this.
Introduction
There is concern that neonates’ hearing could be harmed due to the noise produced during magnetic resonance imaging (MRI) procedures, but knowledge gaps preclude making a safety assessment. As a first step in making a neonatal MRI hearing safety assessment, a sound level survey of MRI scanners was conducted to quantify the expected sound exposure during neonatal brain protocols.Methods
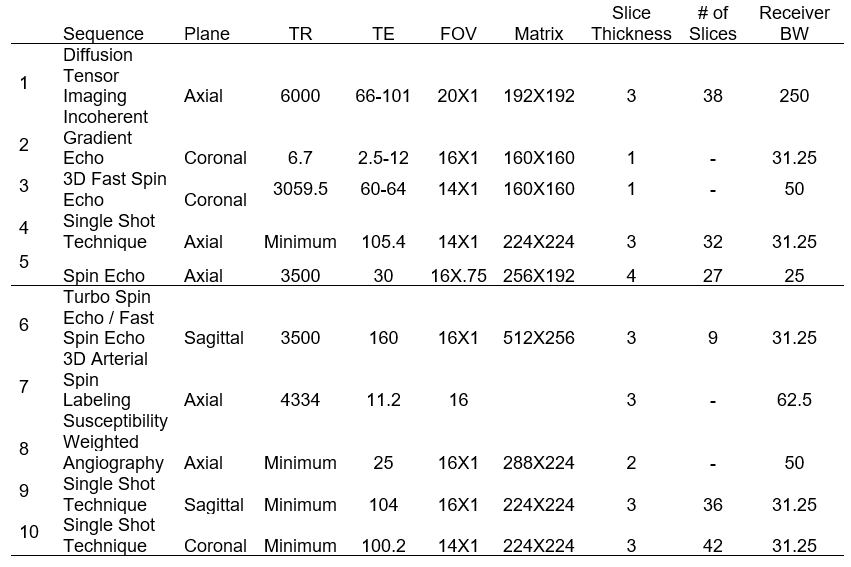
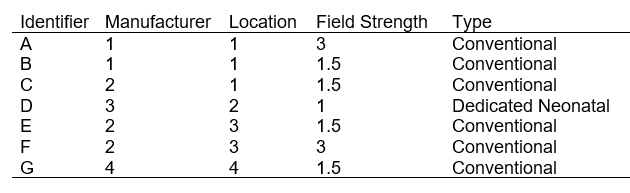
Neonatal brain protocols were recorded using a sound level meter (B&K 2250, Bruel and Kjaer, Nærum, Denmark). The protocols recorded on scanners A, C and D were protocols designed by facilities that regularly scan neonates. The protocols recorded on the remaining scanners (based at facilities that don’t scan neonates) were made to emulate the scanner A protocol (Figure 1).The sound level meter was calibrated using a sound calibrator (B&K 4231, Bruel and Kjaer, Nærum, Denmark) prior to each recording session. The sound level meter was fit with a 1/2’’ pressure field microphone (B&K 4192, Bruel and Kjaer, Nærum, Denmark) and a preamplifier (B&K ZC-0032, Bruel and Kjaer, Nærum, Denmark), mounted on a phantom provided by each facility and then placed in the isocenter of the bore. The microphone and preamplifier were attached to a 10-meter-long cable (B&K AO-0697-D-100, Bruel and Kjaer, Nærum, Denmark), which connected to the sound level meter that was out of reach of the magnetic field.
Results
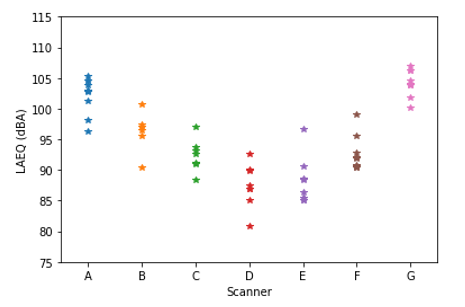
We measured the sound pressure levels of 7 neonatal brain protocols on 7 different MRI machines (Figure 2) across 4 manufacturers. The average scan level A-weighted equivalent value (LAEQ) was 96.88 dBA and the range was 80.8 – 109.3 dBA.Our data also enables within-scanner and between-scanner comparisons. The protocol recorded on the neonatal scanner was found to be significantly quieter than the other scanners using the Mann-Whitney U-Test (P = 4.44e-05, f =.0811, Cohen d = 1.68). Further, the LAEQ ranges of the scans from each protocol vary between 8.49 – 11.9 dBA, which may indicate that scan type can, at most, alter the sound pressure level by about 10 dBA. In addition, the range of neonatal brain protocol average LAEQs across the scanners is 14.87 dBA.
The sound level results are summarized in Figure 3.
Discussion
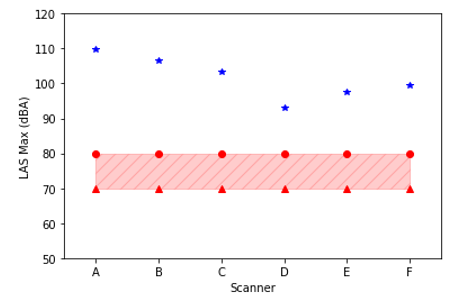
The recorded neonatal protocol sound pressure levels exceeded sound pressure levels that have been associated with negative non-auditory outcomes in infants including changes in heart and respiratory rates, transcutaneous oxygen tension, and intracranial pressure1,2, indicating that neonates likely experience non-auditory reactions to loud sounds during neonatal brain protocols (Figure 4). However, the degree to which these non-auditory outcomes are dangerous is unknown 3.The recorded neonatal protocol sound pressure levels did not exceed the dosage prescribed by the IEC 60601-2-33 MRI hearing safety limit 4 (Figure 5), though a comparison to the IEC 60601-2-33 MRI hearing safety limit may not be appropriate for neonates.
Previous sound level studies report adult scan LAEQs between 84 dBA and 112.5 dBA over the past 31 years 5-12. Though adult and neonatal MRI scans are different, the scan LAEQs from our neonatal sound level survey are in-line with the adult scan LAEQs from the literature. This suggests that adult scans may not be louder than neonatal scans.
However, in practice, the acoustic exposure to the neonatal patient may be significantly louder, as the amount of attenuation from infant hearing protection varies wildly depending on the options used. The sites we visited that routinely scanned infants (location 1 and 2) reported using the following neonatal hearing protection devices (HPDs): neonatal noise attenuators (Minimuffs, Natus, Pleasanton, CA) only, neonatal noise attenuators and a soft silicone putty (Macks pillow soft silicone earplugs, McKeon Products, Inc., Warren, MI), and foam earplugs designed for adults cut-to-infant-size (such as E-A-Rsoft Yellow Neons, E-A-R, Boulder, CO). The noise reduction rating (NRR) 13 of Minimuffs is only 7 dBA, Macks silicone earplugs is 22 dBA and E-A-Rsoft Yellow Neons is 33 dBA, though when cut, this NRR is no longer dependable. Based on the calculations in an OSHA standard 14 and using these NRRs, Minimuffs alone are expected to offer no attenuation in practice, the dual-use of Minimuffs and Macks is expected to offer 12.5 dBA of attenuation and the use of E-A-Rsoft Yellow Neons on adults is expected to attenuate the exposure by 12.5 dBA.
Conclusion
The sound levels achieved during neonatal protocols likely induce negative non-auditory outcomes in infants, but it is inconclusive whether they cause negative auditory outcomes due to the dearth of information surrounding neonatal hearing tolerance. In response to this gap, we are pursuing a prospective cohort study to evaluate whether MRI machine sound levels induce a negative auditory outcome in infants. Without this information, a definitive safety evaluation cannot be made. For additional future work, we would like to clarify whether neonatal MRI protocol sound levels are comparably loud to adult MRI protocol sound levels, which the data suggested.Acknowledgements
We thank Maggie Johnson, Stanley Fricke, Nathan Macdonald and John Mugler for providing access to the MRI machines. We would also like to thank Dr. Jana Delfino for helpful discussions and editing.
References
1. Long JG, Lucey JF, Philip AGS. Noise and Hypoxemia in the Intensive Care Nursery. Pediatrics. 1980;65(1):143.
2. Anderssen SH, Nicolaisen RB, Gabrielsen GW. Autonomic response to auditory stimulation. Acta Paediatr. 1993;82(11):913-8.
3. Morris B, Philbin, M. Kathleen, Bose, Carl. Physiological Effects of Sound on the Neonate. Journal of Perinatology. 2000;20.
4. IEC. Medical Electrical equipment - Part 2-33: Particular requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis. 2010.
5. Hurwitz R, Lane SR, Bell RA, Brant-Zawadzki MN. Acoustic analysis of gradient-coil noise in MR imaging. Radiology. 1989;173(2):545-8.
6. McJury PhD M, Shellock PhD FG. Auditory Noise Associated With MR Procedures: A Review. Journal of Magnetic Resonance Imaging. 2000;12(1):37-45.
7. McJury MJ. Acoustic noise levels generated during high field MR imaging. Clin Radiol. 1995;50(5):331-4.
8. Counter SA, Olofsson A, Grahn HF, Borg E. MRI acoustic noise: Sound pressure and frequency analysis. Journal of Magnetic Resonance Imaging. 1997;7(3):606-11.
9. Price DL, De Wilde JP, Papadaki AM, Curran JS, Kitney RI. Investigation of acoustic noise on 15 MRI scanners from 0.2 T to 3 T. J Magn Reson Imaging. 2001;13(2):288-93.
10. Radomskij P, Schmidt MA, Heron CW, Prasher D. Effect of MRI noise on cochlear function. The Lancet. 2002;359(9316):1485-6.
11. Hattori Y, Fukatsu H, Ishigaki T. Measurement and evaluation of the acoustic noise of a 3 Tesla MR scanner. Nagoya J Med Sci. 2007;69(1-2):23-8.
12. McNulty JP, McNulty S. Acoustic noise in magnetic resonance imaging: An ongoing issue. Radiography. 2009;15(4):320-6.
13. NIOSH. Occupational Noise Exposure. 1998 June. Contract No.: 98-126.
14. OSHA. Methods for Estimating HPD Attenuation. https://www.osha.gov/SLTC/noisehearingconservation/attenuation.html.
Figures
Maximum A-weighted slow-time constant sound level (LAS Max) of neonatal protocols by scanner relative to sound levels associated with non-auditory reactions to sounds. Compared to the non-auditory infant reaction data from Anderssen et al 2 (red dots) and Long et al 1 (red triangles), every recorded neonatal protocol (blue stars) likely induces changes in heart rate, transcutaneous oxygen saturation and intracranial pressure.
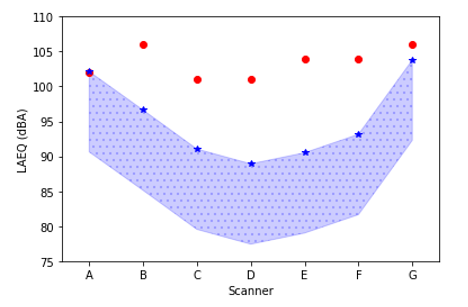
LAEQ of neonatal protocols by scanner relative to the IEC MRI hearing safety threshold. Compared to the IEC MRI hearing safety limit (red dots), every neonatal protocol LAEQ (blue stars) with hearing protection (blue spotted area) is below the limit. The maximum hearing protection limit was calculated using an OSHA standard 14.