2133
MultiBand-SENSE EPI with Variable-Rate Selective Excitation (VERSE) pulses for accelerating abdominal DWI with respiratory triggering
Kosuke Morita1, Masami Yoneyama2, Hiroshi Hamano2, Takeshi Nakaura3, Seitaro Oda3, Akira Sasao3, Hiroyuki Uetani3, Shogo Fukuda3, Masahiro Hatemura3, and Toshinori Hirai3
1Radiology, Kumamoto university, kumamoto-shi, Japan, 2Philips Japan, shinagawa, Japan, 3Kumamoto university, kumamoto-shi, Japan
1Radiology, Kumamoto university, kumamoto-shi, Japan, 2Philips Japan, shinagawa, Japan, 3Kumamoto university, kumamoto-shi, Japan
Synopsis
We used respiratory triggered MultiBand SENSE (MB-SENSE) DWI using variable-rate selective excitation (MB-VERSE). We first measured ADC values of liver and kidney and subsequently performed visual assessment. The MB-VERSE DWI reduced the imaging time while improving the image quality and robustness of ADC values.
INTRODUCTION
Respiratory triggering or navigator diaphragmatic triggering is commonly used in abdominal DWI. Since wider coverage for slice direction is needed to include main abdominal organs such as liver pancreas and kidney, the number of slices is increased, and it leads to prolong the acquisition time. Recently, simultaneous multi-slice (SMS) or MultiBand SENSE (MB-SENSE) technology has become available in clinical studies, and multi-slice exciation can be performed in one TR, contributing to shortening the acquisition time. However, the use of MB-SENSE in the body may lead to degradation of image quality due to degradation of Signal-to-noise ratio (SNR), increase of Specific Absorption Rate (SAR) and decrease of RF peak voltage. In this study, we used a combination of MB-SENSE and variable-rate selective excitation (MB-VERSE) pulse, which has the advantages of reducing SAR, RF energy and transmit pulse width, as shown in Figure 1. Purpose of our study was evaluated the usefulness of MB-VERSE with respiratory triggered abdominal DWI.METHODS
Eight healthy volunteers (age; 37.4 ± 6.8 y.o., weight: 78.5 ± 9.9 kg) were performed with a Philips Ingenia 3.0T CX and ds-TORSO coils. Scan parameters of DWI were as follows: TR / TE = 1090 - 2180 / 56 - 61 ms, field-of-view = 350 × 350 mm2, acquisition matrix = 112 × 133 (reconstruction matrix = 256 × 256), slices thickness = 7.0 mm, voxel size = 3.1 × 2.6 × 7.0 mm, number of slices = 25, NSA = 3, EPI factor = 67, Band width = 3102.1 Hz, SENSE factor = 2.0, b-values = 0 and 800 sec/mm2, Acquisition time = 1:09 - 2:18, Transverse plane acquisition. The three conditions to be compared were MB-SENSE, MB-VERSE, and conventional SENSE DWI (with no-MB and no-VERSE) as the reference images. For quantitative evaluation, mean ADC values of liver and kidney were measured from the obtained ADC maps, respectively. In the qualitative evaluation, the overall image quality was assessed by a two-person consensus visual assessment (4 grades; 4: excellent, 3: good, 2: acceptable, 1: poor) with reference to conventional no-MB.RESULTS
Figure 2 shows results of ADCs of liver and kidney between MB-VERSE and MB-SENSE. A volunteer images are shown in Figure 3. ADCs in the liver of reference and MB-SENSE and MB-VERSE were 1.12 ± 0.04, 1.06 ± 0.11, and 1.11 ± 0.07, respectively; similarly, ADCs in the kidney were 2.08 ± 0.13, 2.18 ± 0.14, and 2.10 ± 0.19. Visual assessment showed better results for MB-VERSE than for MB-only (2.5 ± 0.5 vs. 2.8 ± 0.4).DISCUSSION
The MB-VERSE provided more stabilized ADC values, presumably due to the improved SNR particularly in the slice direction thanks to its excitation profile compared to MB-SENSE. Furthermore, with MB factor = 2, the acquisition time can be halved, or the data acquisition time can be halved. Moreover, the prolongation of diffusion time was prevented by using VERSE pulses: 21.9 ms, 23.6 ms and 21.3 ms for reference, MB-SENSE and MB-VERSE. This may have contributed to the suppression of image noise since TE was also not extended.CONCLUSION
The use of MB-VERSE provided more improved image quality and robust ADC values compared with MB-SENSE in abdominal DWI. It is suggested that the image quality can be assured even if the acquisition time is shortened in clinical studies.Acknowledgements
We thank Dr. Kay Nehrke from Philips Research Laboratories Hamburg, Germany, for implementing the MB-VERSE pulse sequence.References
- Brian A Hargreaves, Charles H Cunningham, Dwight G Nishimura, Steven M Conolly. Magn Reson Med. 2004;52(3):590-7.
- Jan M Warnking, G Bruce Pike. Magn Reson Med. 2004;52(5):1190-9.
- Gregory R Lee, Jean A Tkach, Mark A Griswold. Magn Reson Med. 2012;67(1):127-36.
- Simon Konstandin, Lothar R Schad. Magn Reson Med. 2013;70(3):791-9.
Figures
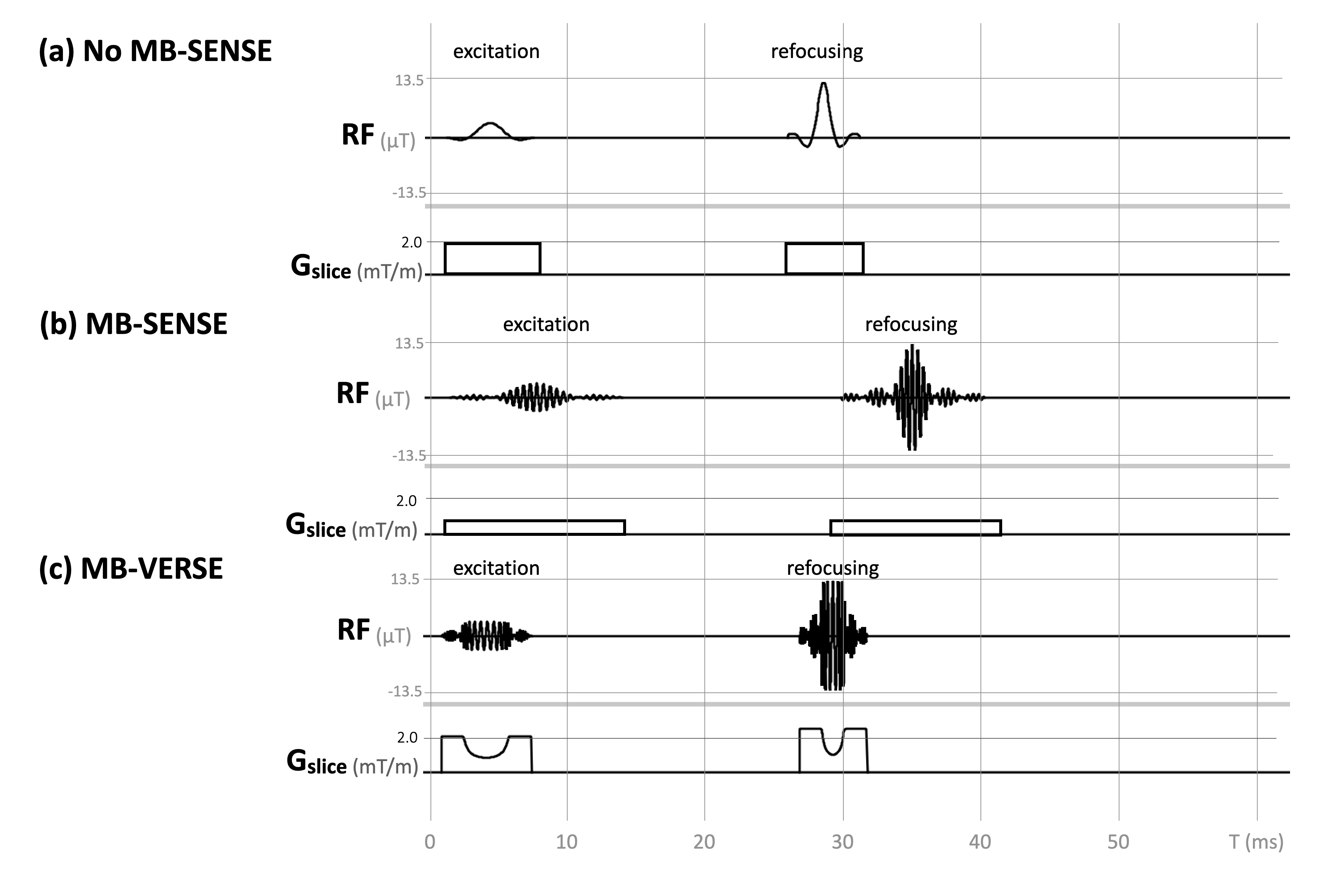
Comparison of VERSE pulse and SINC
pulse. VERSE pulse algorithm is a way to
simultaneously reshape an RF pulse and its slice-select gradient waveform while
maintaining the same excitation profile for on-resonance spins. In short, if
some portion of an RF waveform is stretched in time, a corresponding reduction
in RF amplitude must be made to maintain the same flip angle.
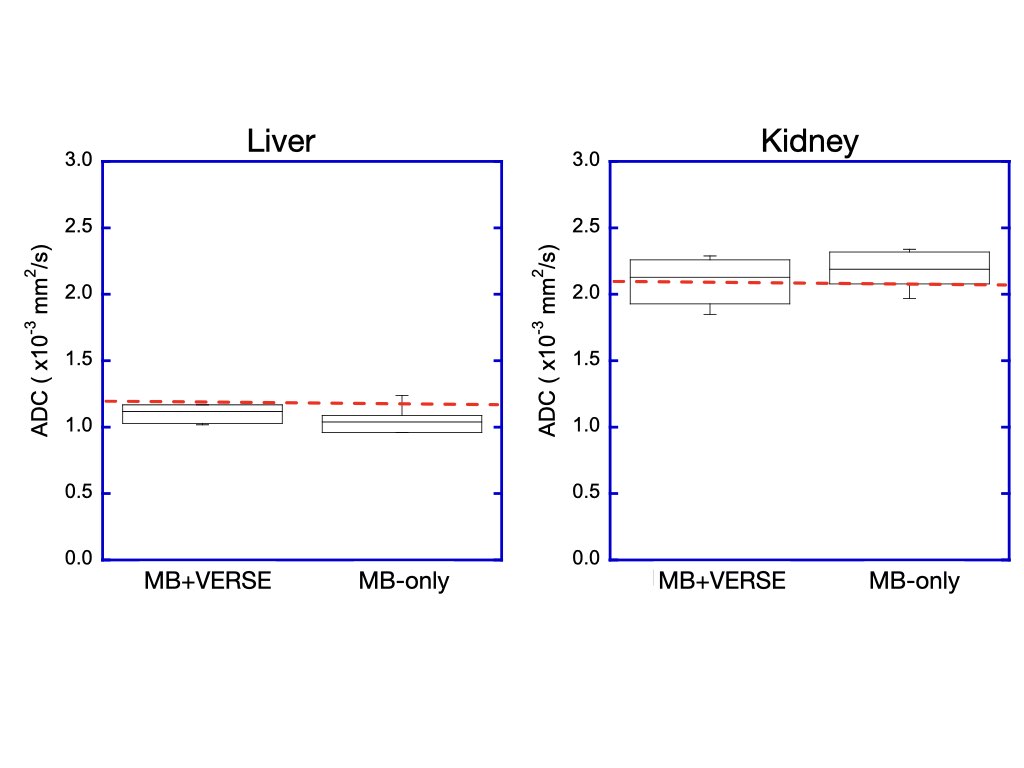
Comparison of ADCs (b = 800) between
MB+VERSE and MB-only. Red line (dots) shows ADC of reference image,
respectively.
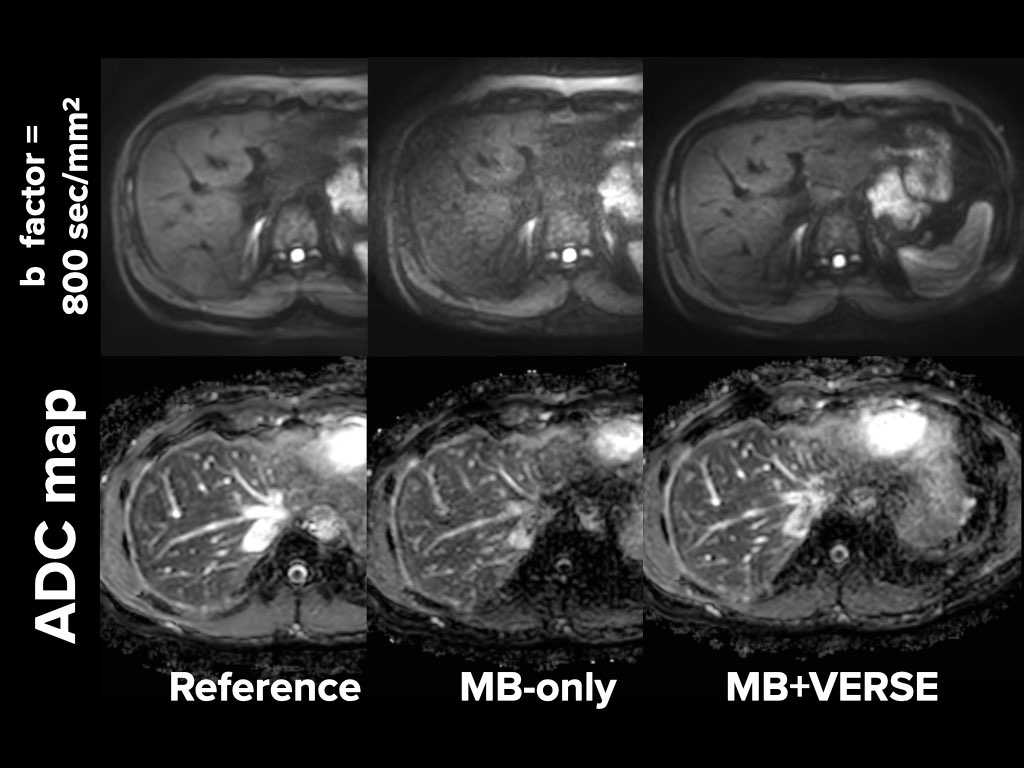
Representative volunteer images. DWI of b
= 800 sec/mm2 images and ADC maps between reference, MB-only and MB+VERSE.